


Metabolic disease should be considered when investigating a lesion in bone. The radiographic changes associated with hyperparathyroidism are well described, but magnetic resonance imaging (MRI) appearances are not.
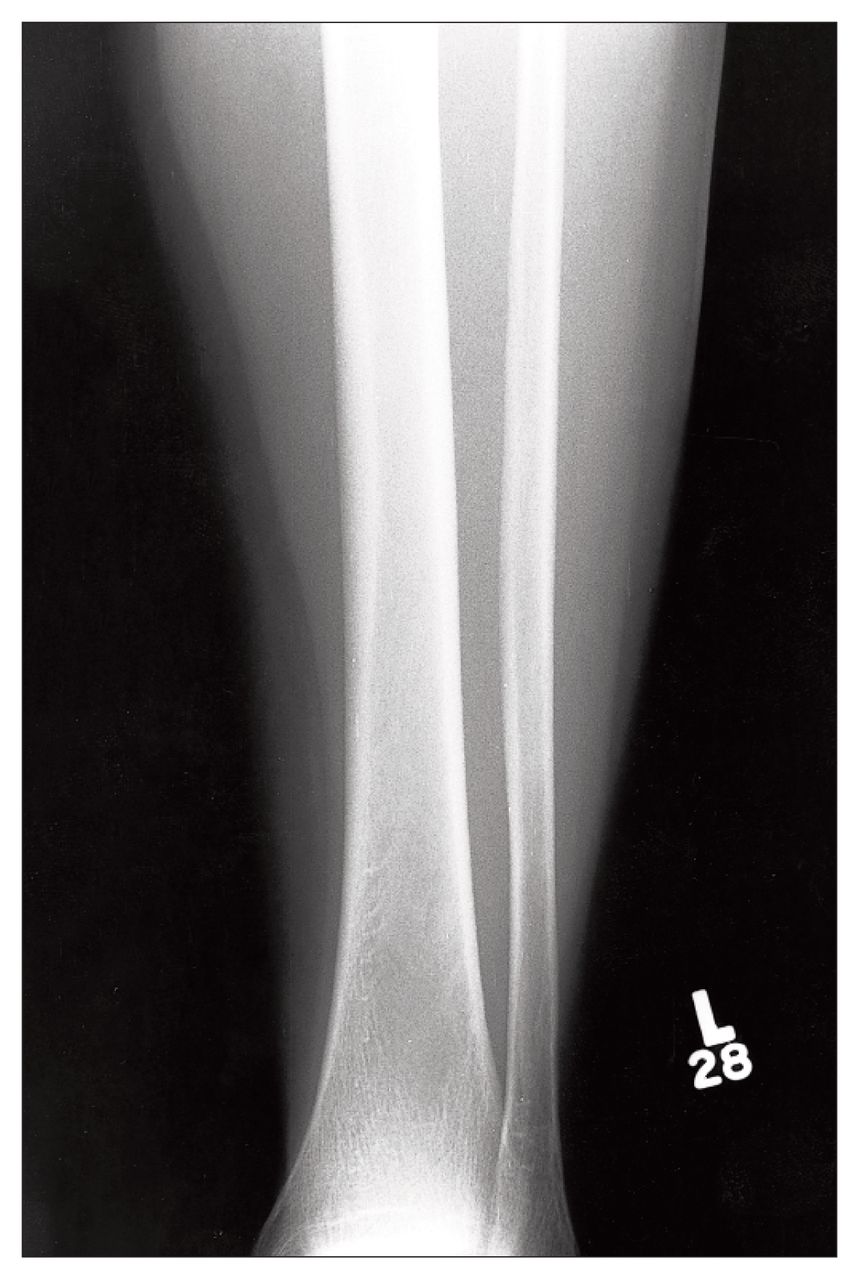
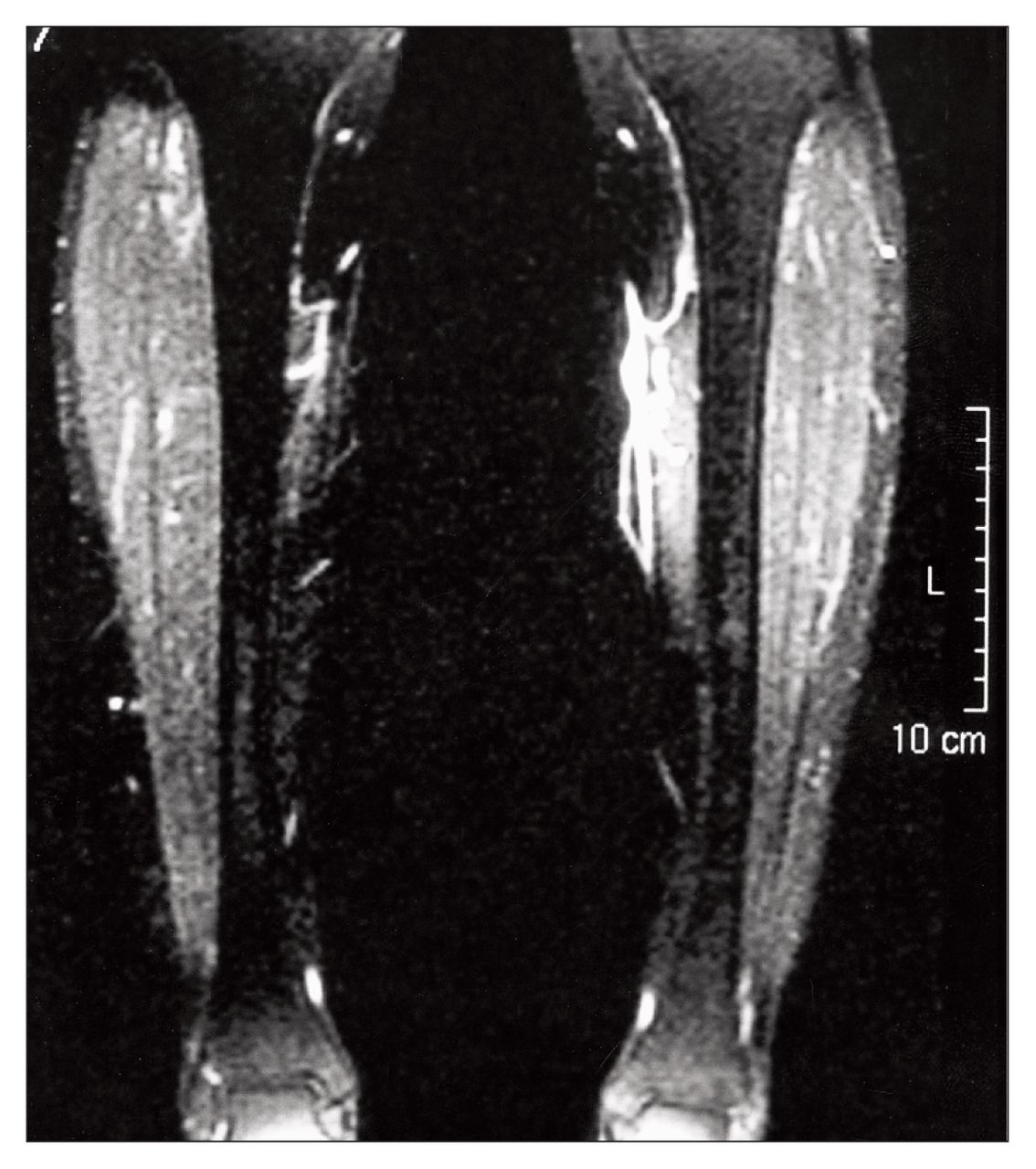
A 53-year-old woman presented with pain in her distal tibia. Plain radiographs were normal (Fig. 1). Blood tests revealed an elevated total serum calcium level of 3.05 mmol/L (normal range from 2.2 to 2.6 mmol/L), a total protein level of 71 g/L (normal range from 60 to 80 g/L) and a low serum phosphate level of 0.63 mmol/L (normal range from 0.90 to 1.45 mmol/L). The serum parathyroid hormone level was raised at 35.6 pmol/L (normal range from 1.3 to 7.6 pmol/L). Isotope bone scanning showed increased uptake in the distal tibia and confirmed that this was a solitary lesion. MRI revealed high signal intensity changes on T2-weighted images in the marrow of the distal tibia (Fig. 2).

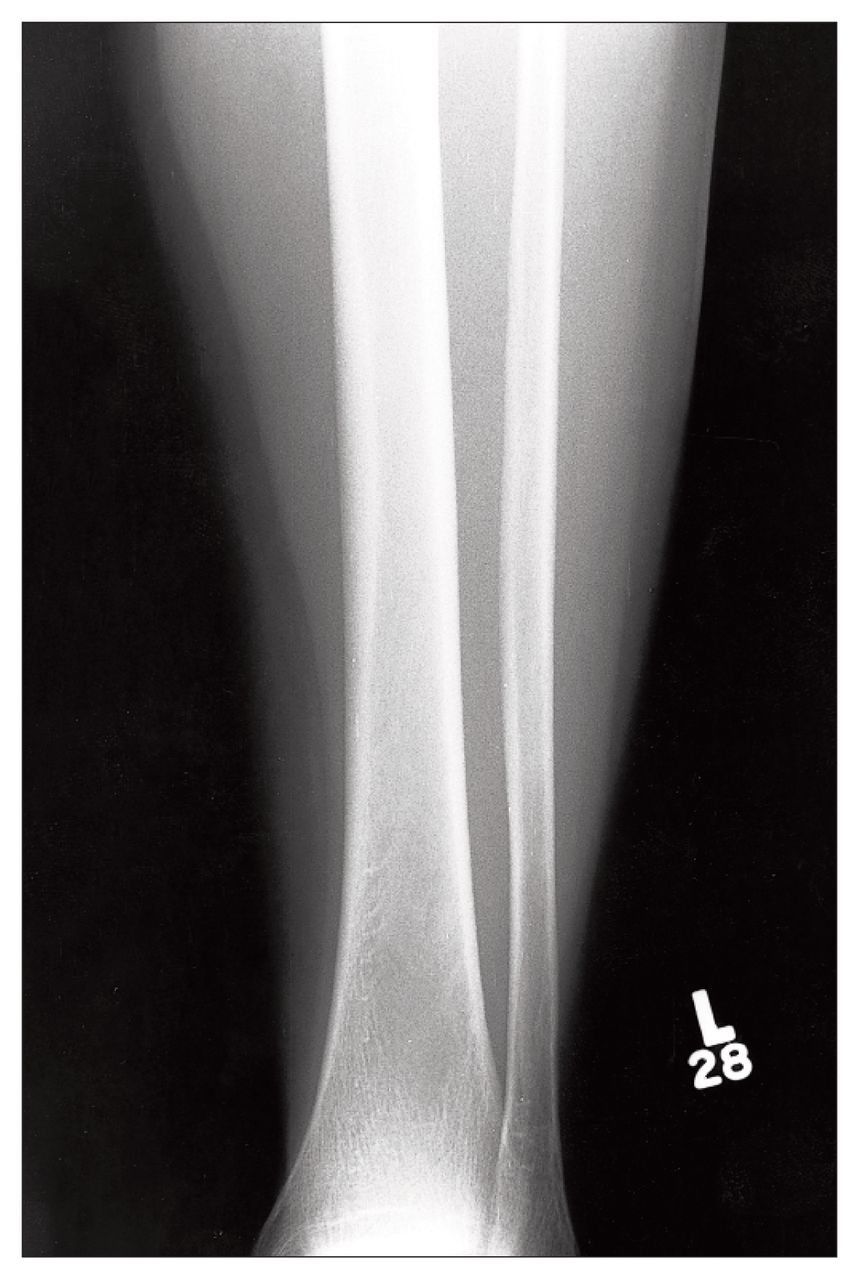
At operation, the right upper parathyroid was found to be enlarged and was excised. Histologic examination of the gland confirmed a parathyroid adenoma. Postoperatively, the serum calcium level returned to normal. At 2 months postoperatively, the symptoms of bone pain had resolved, and a further scan showed that the MRI changes had also resolved (Fig. 3).
Primary hyperparathyroidism is most commonly caused by a solitary parathyroid adenoma. Excessive parathyroid hormone causes a net increase in serum calcium by increasing absorption of calcium from intestine, kidney and bone. Changes in bone include replacement of marrow by fibrous tissue (osteitis fibrosa cystica) and brown tumours, which arise secondary to increased osteoclastic activity and histologically are indistinguishable from giant cell tumours of bone. In this case MRI abnormalities were detected before any radiographic changes and reverted to normal after parathyroidectomy.
Footnotes
Section Editor: Robert S. Bell, MD
Submissions to Surgical Images, musculoskeletal section, should be sent to Dr. Robert S. Bell, University Musculoskeletal Oncology Unit, Ste. 476, 600 University Ave., Toronto, ON M5G 1X5; fax 416 586-8397.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.