


Large femoral geode associated with osteoarthritis of the hip joint
The plain radiograph of the right hip (Fig. 1) demonstrated a large lytic lesion in the proximal femur, which on magnetic resonance imaging (Fig. 2) was shown to be cystic and consistent with a large subarticular cyst. The large femoral geode was confirmed at right total hip arthroplasty.

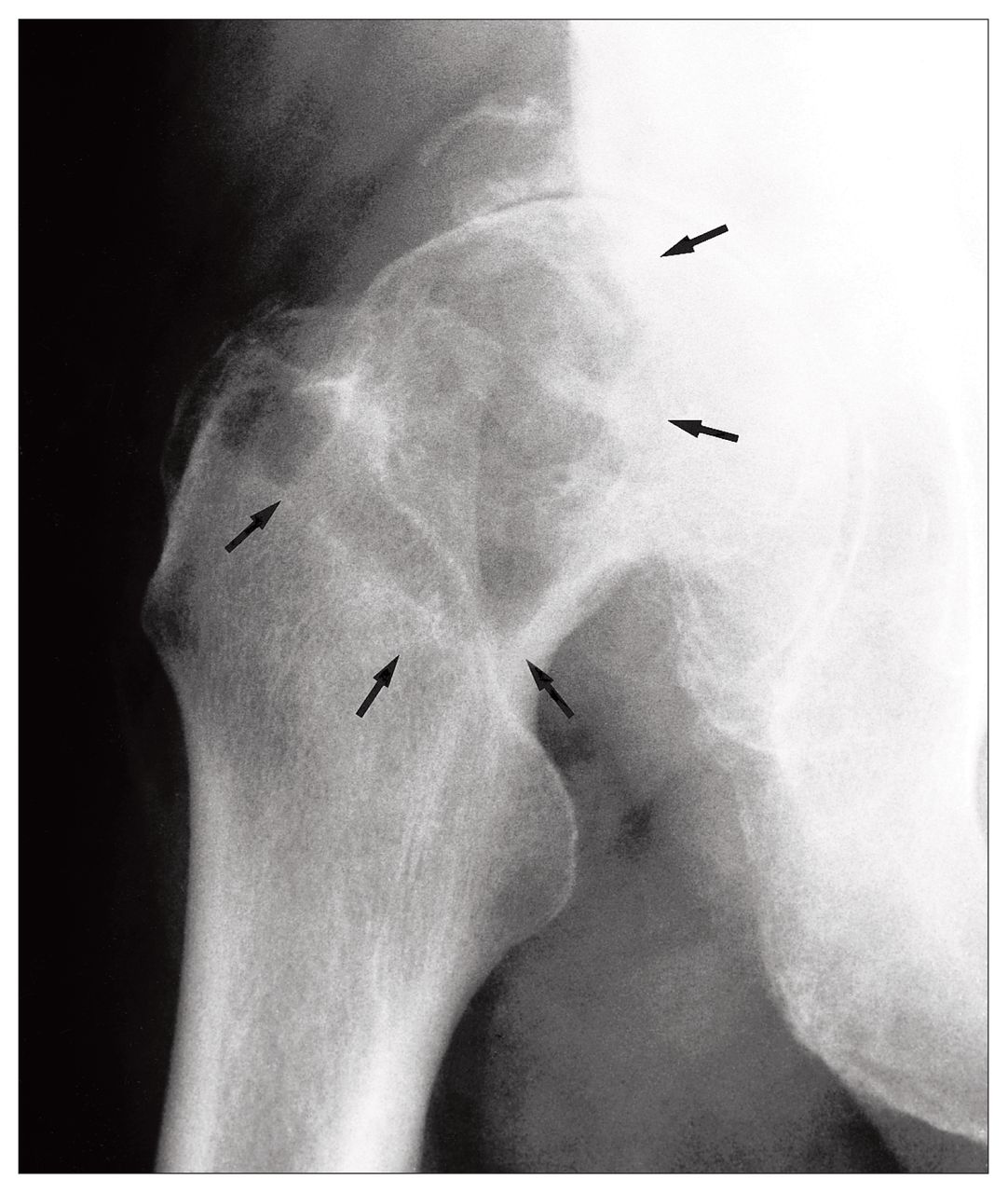
Anteroposterior radiograph of the right hip reveals a large well-defined lytic lesion in the lateral aspect of the proximal femoral meta-piphysis and epiphysis (arrows). Extensive degenerative changes are present with joint space loss, osteophytes and subchondral sclerosis.

Coronal spin-echo, T1-weighted (left) and T2-weighted (right) images of the right hip show the lesion having well-defined borders with low signal on T1 and high signal on T2 consistent with fluid. The lesion did not enhance after administration of contrast medium. The extensive degenerative changes are shown.
The term geode is used in geology to describe small hollow rocks lined with crystals.1 Subchondral cysts, or geodes, are common findings in degenerative joint disease. They can be seen in rheumatoid arthritis, osteoarthritis, calcium pyrophosphate deposition disease and avascular necrosis.2 The cysts typically form within the weight-bearing portion of subchondral bone. Pathologically, they appear between thickened trabeculae and are of variable size and multiplicity. The pathogenesis is thought to be due either to synovial fluid intrusion or to bony contusion with subsequent fracture and vascular compromise of subchondral bone, causing cystic necrosis.1
A geode can mimic a more ominous process such as chondroblastoma, giant cell tumour and skeletal metastasis, especially when it occurs in the presence of a normal-appearing joint.2 A femoral neck geode without joint involvement in a rheumatoid patient has been reported.3
The MRI appearance of the geode in this case is typical. With the use of appropriate imaging techniques, biopsy of such a lesion can be avoided.2,3
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.