


Resection of solitary small-bowel metastases from bronchogenic carcinoma may be curative in the absence of residual or other metastatic disease.1 Although most cases of small-bowel metastases have occurred in patients with advanced disease, in whom small-bowel resection is followed by imminent demise,2 we report a case of isolated metachronous jejunal metastases from a squamous cell carcinoma that were resected for potential cure.
Case Report
A 62-year-old man underwent a right upper lobectomy for a poorly differentiated epidermoid carcinoma with involvement of the visceral pleura. The hilar resection margin was free of carcinoma and the hilar, interlobar and tracheobronchial-angle lymph nodes were all negative for metastases. Preoperative computed tomography showed no evidence of spread to the liver, adrenal glands or other viscera. Bone scanning was negative for metastatic disease.
Ten months later, he complained of feeling generally unwell with decreased energy, nausea, abdominal cramps and diarrhea. CT of the abdomen demonstrated a large intraluminal mass in the small bowel (Fig. 1). Colonoscopy was also performed and found to be normal. Laparotomy revealed 2 lesions in the jejunum, confirmed as discrete nodular carcinomatous deposits, ulcerating into the bowel mucosa with transmural involvement of the bowel wall. These were resected, and primary anastomoses were performed. The resection margins were clear of malignant cells, and the mesenteric lymph nodes were negative for metastases. Histologically, the lesions were similar to the previously resected lung carcinoma and were thought to represent metastatic disease.
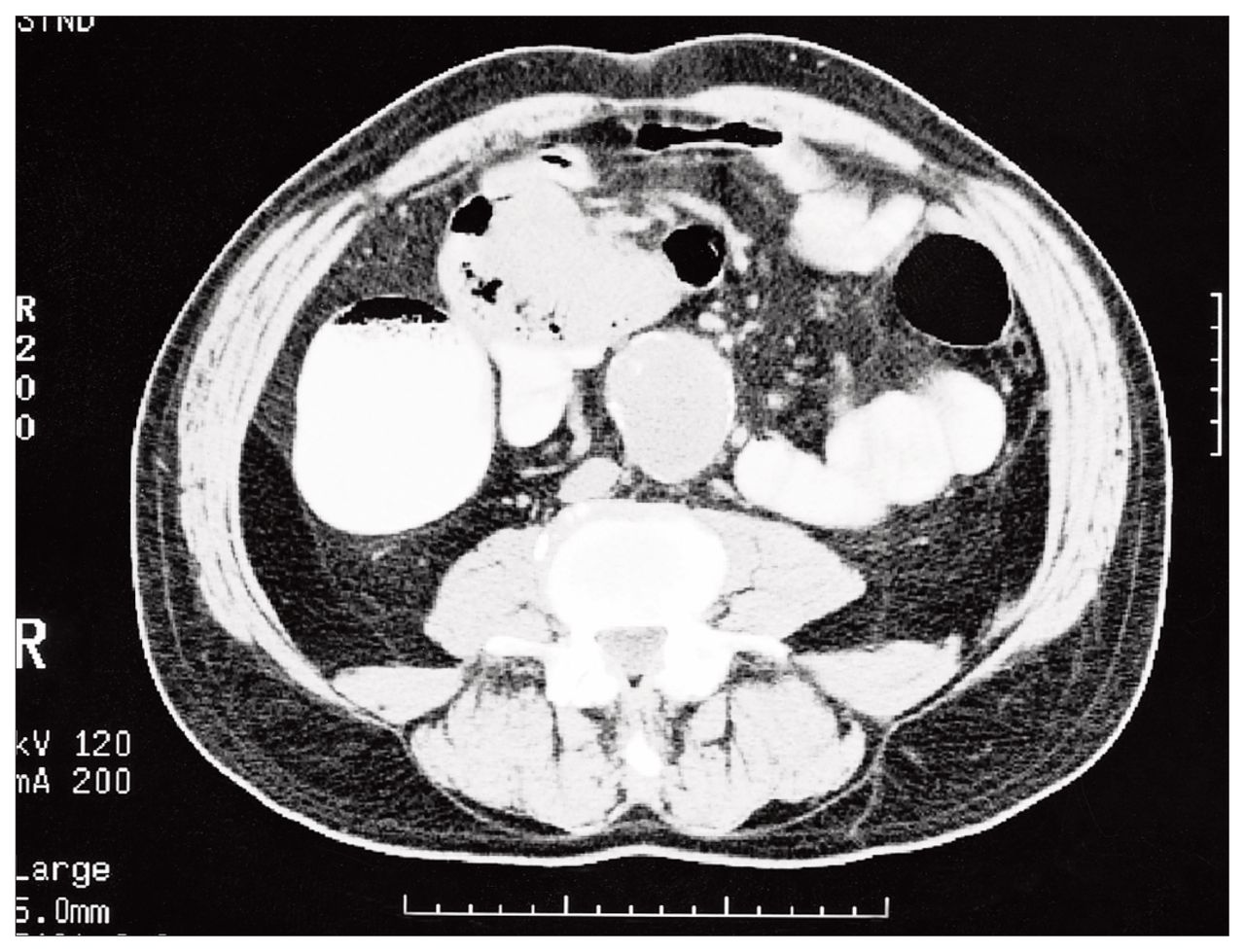
Computed tomography scan demonstrating jejunal tumour. Incidentally, an abdominal aortic aneurysm is present.
The patient had no clinical or radiologic evidence of disease at 45 months’ follow-up.
Comment
Metastasis from bronchogenic carcinoma to the small bowel is usually considered a late finding and is characteristic of highly aggressive disease. Although small-bowel metastases may result in either obstruction or bleeding, intestinal perforation is by far the most common presentation and is thought to be due to necrosis of the metastatic nodule.3 Most tumours spreading to the small bowel from the lung are of high grade, are poorly differentiated and are non-small cell in type.
In the majority of reported cases of small-bowel metastases, the primary lung tumour was unresectable at the time of presentation, was accompanied by widespread metastatic disease or was found as a result of the abdominal complaints. Palliative radiotherapy, chemotherapy and occasionally palliative resection were the usual treatment modalities. It is therefore not suprising that the prognosis in these patients was so poor, with most surviving less than 16 weeks after laparotomy.
Other primary malignant lesions that metastasize to the small bowel (e.g., those of skin, cervix, colon and ovary) have been shown to be discrete events in which “vigorous surgical therapy does not imply a hopeless prognosis,”4 as long as the primary tumour has been adequately resected and there are no other signs of metastasis. The evidence of this same phenomenon for bronchogenic carcinoma is less abundant. We are aware of only 2 other case reports of previously resected primary bronchogenic carcinoma in which isolated small-bowel metastases were subsequently found and resected with intent to cure.1,5 In both of these cases, patients were alive and well at the time of publication (5 months and 8 years after laparotomy). This case report adds to the evidence that perhaps isolated small-bowel metastasis from bronchogenic carcinoma, in the absence of other metastatic or residual disease, may have a better prognosis with resection. This finding should therefore prompt surgeons to pay close attention to subtle abdominal complaints in patients in whom a “curative” pulmonary resection has been performed for bronchogenic carcinoma. As with other extracranial solitary metastases of non-small cell carcinoma of the lung, aggressive treatment with resection of isolated small-bowel metastases when the primary tumour has been resected should be considered since this approach may improve long-term survival.6
- Accepted August 13, 1998.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.