


In 1962, Stout1 first introduced the term “leiomyoblastoma” into the English literature with a report of 69 cases of myogenic gastric tumour, 2 of which were malignant. He suspected that these tumours were myogenic, but this was proved only recently by ultrastructural studies. In the recent classification of soft-tissue tumours proposed by the World Health Organization, these tumours are called epithelioid leiomyomas or leiomyosarcomas.2
Since epithelioid leiomyosarcoma of gastric origin is rare, there have been only a few published reports of a limited number of patients. 3–7 Occasionally, the tumour becomes evident as an abdominal mass, in which case laparotomy shows extensive tumour involvement of the gastrocolic ligament and the greater omentum, with diffuse thickening of each. We describe another case of gastric epithelioid leiomyosarcoma.
Case Report
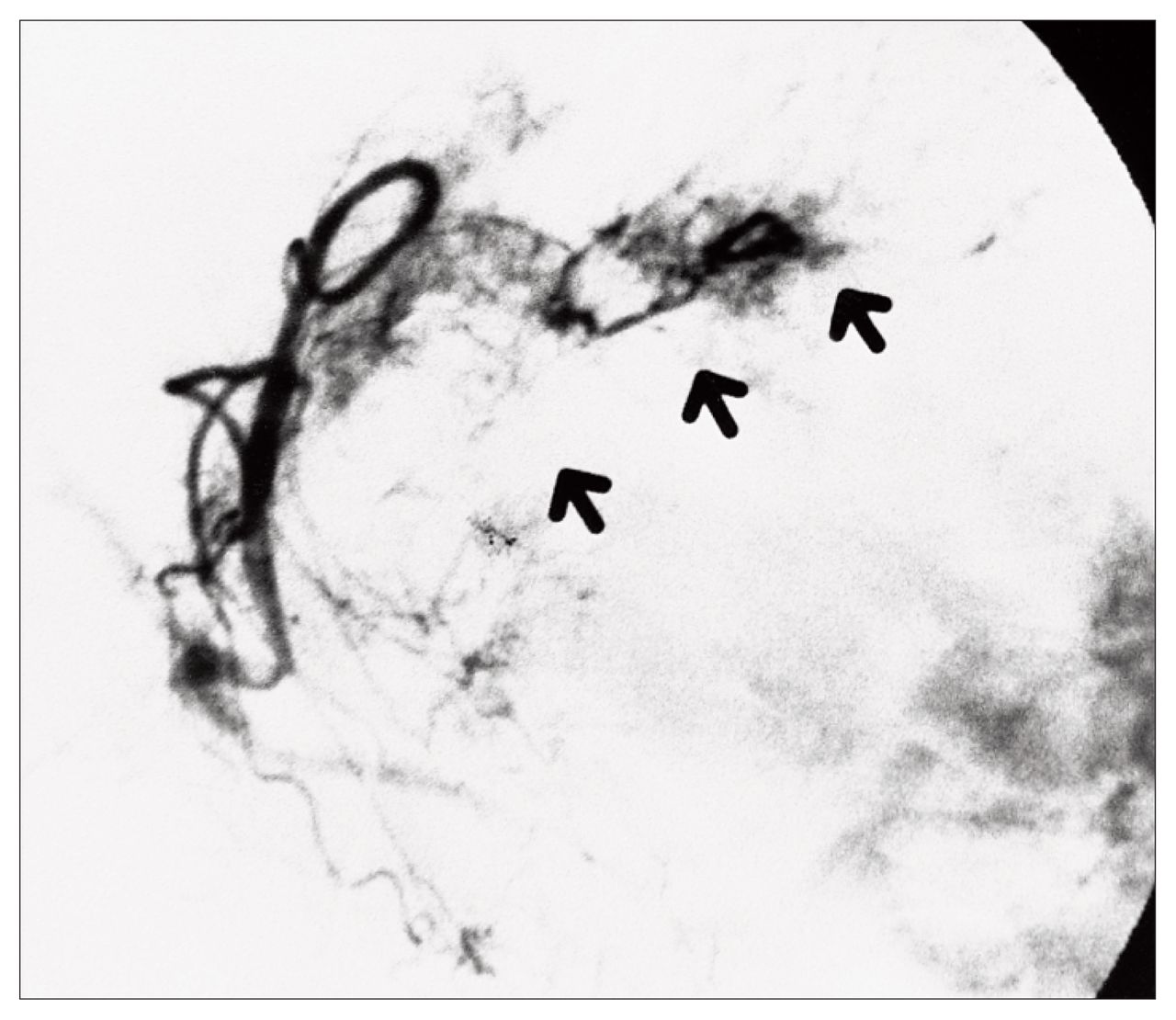
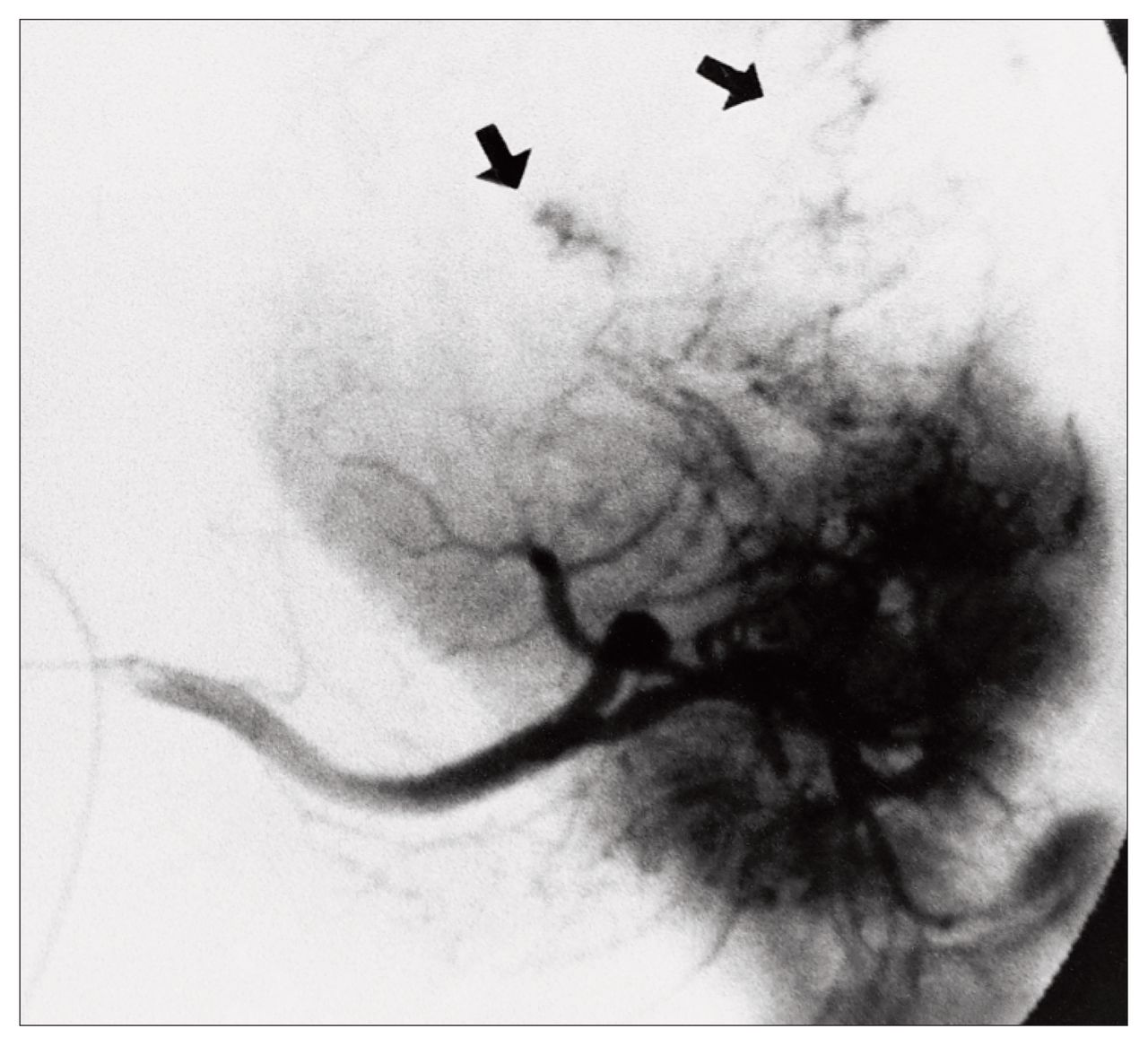
A 63-year-old man was admitted for the evaluation of upper abdominal pain. Laboratory data, including complete blood count and blood chemistry, were normal. On physical examination he had a large, tender, firm mass in the right upper abdomen with a clear contour and smooth surface. The echogram showed a high echogenic mass with a clearly defined margin in the right subcostal area. Computed tomography revealed a large mass with heterogeneous low-density contents, compressing the anterior gastric wall (Fig. 1). Upper gastrointestinal series also demonstrated right lateral deviation and extrinsic compression of the stomach by a large abdominal mass (Fig. 2). Abdominal angiography showed a giant hypervascular mass with stretching of the left gastric artery, from which numerous vessels fed the tumour (Fig. 3). Feeding vessels from the splenic artery also entered the tumour (Fig. 4).

On computed tomography a large mass with heterogeneous low-density contents is seen compressing the anterior gastric wall.

An upper gastrointestinal series shows right lateral deviation and extrinsic compression of the stomach by a large abdominal tumour (arrows).

Selective angiography of the left gastric artery demonstrates a hypervascular mass with stretching of the artery (arrows).

Feeding vessels (arrows) entering the tumour from the splenic artery.
Laparotomy revealed a large upper abdominal mass, measuring approximately 23 × 13 × 13 cm, located on the anterior serosal surface of the fundus, from which numerous feeding arteries were visible (Fig. 5). The mass elevated the lateral segment of the liver superiorly and the spleen laterally. Because the mass adhered to the diaphragm, excision using electrocautery included full-thickness of the diaphragm with an adequate margin of normal tissue. The resultant defect was closed in a transverse fashion. Total gastrectomy, omentectomy and splenectomy were performed, and continuity was re-established by an esophagojejunostomy according to the jejunal pouch interposition principle. Intraoperatively, 50 mg of mitomycin C adsorbed on activated carbon particles (MMC-CH)8 was instilled into the peritoneal cavity.

The large upper abdominal mass located on the anterior surface of the gastric fundus.
Examination of the resected specimen showed that the tumour was well encapsulated. It weighed 2300 g, had a smooth surface and was of yellowish colour. The cut surface revealed extensive central necrosis, with the periphery consisting of faintly lobulated cells.
Microscopically, the specimen consisted of sheets of round, oval and polygonal cells with ill-defined borders (Fig. 6). Tumour cells had round or oval nuclei and abundant eosinophilic cytoplasm. There was a transition from round to spindle cells in some sections. Over 20 mitotic figures per 50 high-power fields were seen. Thus, microscopic features were consistent with a pathological diagnosis of epithelioid leiomyosarcoma.

The epithelioid tumour cells contain a rounded nucleus with one or more usually small or moderate-sized nucleoli. There were epithelioid tumour cells with fairly abundant cytoplasm, which was vacuolated or clear.
Discussion
Epithelioid leiomyosarcomas arise from the muscularis propria of the gastrointestinal tract and uterus.3 It has been reported to occur most often in the stomach; of 155 leiomyoblastomas, 146 occurred in the stomach.3 These tumours primarily affect middle-aged men and usually present with upper gastrointestinal bleeding or peptic-ulcer-like symptoms. The epithelioid leiomyosarcomas often arise in the proximal stomach, especially on the posterior wall. Microscopically, they are composed of a mixture of round epithelioid and spindle cells, many of which have clear cytoplasm.
Epithelioid leiomyosarcomas are distinguished from “benign” epithelioid leiomyomas principally on the basis of mitotic figures and size.3 When the tumours are larger than 6 cm in dimension, they should be considered malignant. Metastases occur most commonly in the liver and peritoneal surfaces and are strongly correlated to mitotic activity and size. Since the resected tumour in our patient measured 23 cm and had 20 mitoses per 50 high-power fields, he should be closely followed up postoperatively. It is believed that these residual tumour cells usually take some time to reach a sufficient size to compress the gastrointestinal tract, and by that time widespread metastases are evident. Thus, it is important to observe the enlargement of these tumours carefully by ultrasonography or CT.
Anticancer drugs should be given to suppress the proliferation of the residual tumour cells. Although several requirements should be met for a drug to be considered for intraperitoneal use in patients with locally recurrent or persistent peritoneal disease, no specifically effective drugs against leiomyosarcomas are known.
Surgical resection is the treatment of choice for gastric leiomyosarcomas. Every effort should be made to excise the tumour completely with an adequate margin of uninvolved tissue. In the experience of Appelman and Helwig,3 the extent of surgical excision does not affect survival; total or subtotal gastrectomy offered no better chance for survival than segmental resection, if the resection margins were negative for tumour cells. It is sometimes difficult, however, to resect such a tumour segmentally due to numerous feeding arteries at its surface. The great deterrent to resection of an abdominal tumour is the risk of hemorrhage due to the tumour’s vascularity. It might be argued that although some lesions may be pathologically benign at the time of removal, they could become malignant if left alone. Therefore we believe that total gastrectomy offers the best palliation for patients having this tumour. Resection of adjacent organs may be necessary to accomplish complete excision. In our patient, the stomach, spleen and a part of the diaphragm were also removed.
The liver and peritoneal surfaces are the most common sites of metastasis. The retroperitoneal soft tissues are frequently involved. MMC-CH has been used during operation to suppress residual lesions of a wide variety of tumours.8 MMC-CH has been effective in the treatment of effusion of malignant cells into peritoneal and pleural cavities due to metastatic tumour, which is usually resistant to other forms of chemotherapy. The direct instillation of MMC-CH into the peritoneal cavity is effective in treating malignant effusions. It compares favourably with the results obtained by the use of MMC alone. MMC solution administered intraperitoneally is easily absorbed through the blood capillary walls into blood plasma, and the MMC level in the peritoneal cavity is lower than that of MMC-CH. The mechanism of action of the MMC-CH presumably is due to the presence of a high concentration of MMC in direct contact with the tumour cells. Such a high local concentration may permit a more effective cytotoxic action.
Most metastasizing epithelioid leiomyosarcomas have an unfavourable prognosis.4 The clinical behaviour of the epithelioid leiomyomatous tumour of gastric origin, however, often is difficult to predict. Only approximately 20% of epithelioid leiomyomatous gastric tumours follow a malignant course. Large size and multinodularity, high mitotic activity and mucosal infiltration have been reported to be of prognostic significance.3,5
- Accepted March 5, 1998.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.