


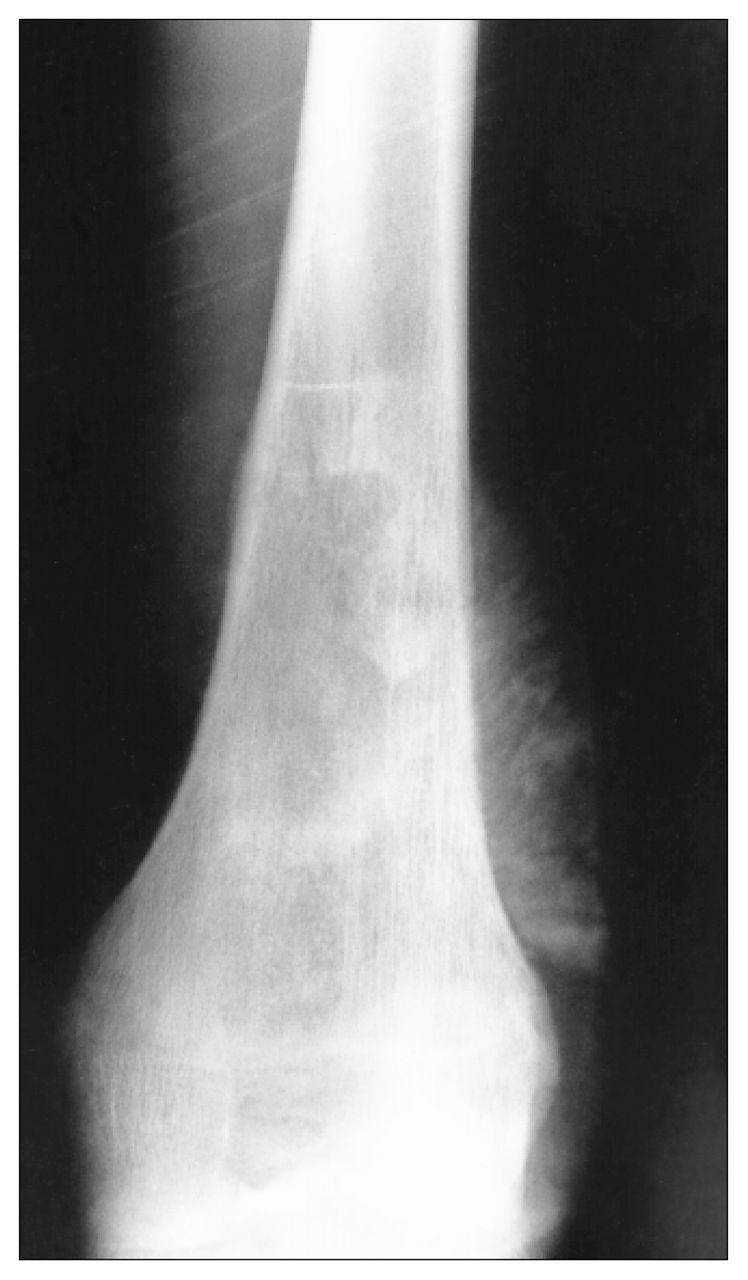
A 19-year-old man presented with pain in the distal femur (Fig. 1). A diagnosis of osteosarcoma was made after open biopsy of the mass. Staging studies revealed multiple pulmonary metastases. Neoadjuvant chemotherapy, including vincristine, methotrexate, cisplatinum and doxorubicin was given with good clinical response. Because of joint involvement, an extra-articular resection of the knee was done together with the distal femur. The patella was resurfaced. Pulmonary metastases were resected after treatment of the primary tumour was completed.

Radiograph of the femur demonstrating a mixed lytic and sclerotic pattern in the metaphysis. There is a marked periosteal reaction with spiculation.
Nine years later, the patient presented to a vascular surgeon with an acutely ischemic leg. Angiography revealed partial occlusion of the popliteal artery from a displaced patellar component (Figs. 2 and 3). Vascular bypass resulted in a successfully perfused limb. The patellar component was removed at a second procedure several weeks later.

Angiogram illustrating displacement of the popliteal artery by the displaced patellar component.

Digital subtraction angiogram illustrating partial occlusion of the popliteal artery by one of the fixation pegs of the patellar component.
Recognized complications of patellar resurfacing include fracture or loosening of the component, patellar subluxation and patellar fracture.1 Late vascular complications are rare. Excision of the soft tissues behind the knee en bloc may have made this complication more likely after a resection for tumour than after a conventional total knee arthroplasty. At present, we do not routinely resurface the patella. It is not clear whether primary removal of the patellar component would have avoided the need for vascular bypass.
Active management of osteosarcoma with pulmonary metastases can lead to long-term survival, and clinicians should be aware of the potential for late complications.
Footnotes
Section Editor: Robert S. Bell, MD
Submissions to Surgical Images, musculoskeletal section, should be sent to Dr. Robert S. Bell, University Musculoskeletal Unit, Ste. 476, 600 University Ave., Toronto ON M5G 1X5; fax 416 586-8397.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.