


Ruptured Baker’s cyst producing a pseudothrombophlebitis syndrome
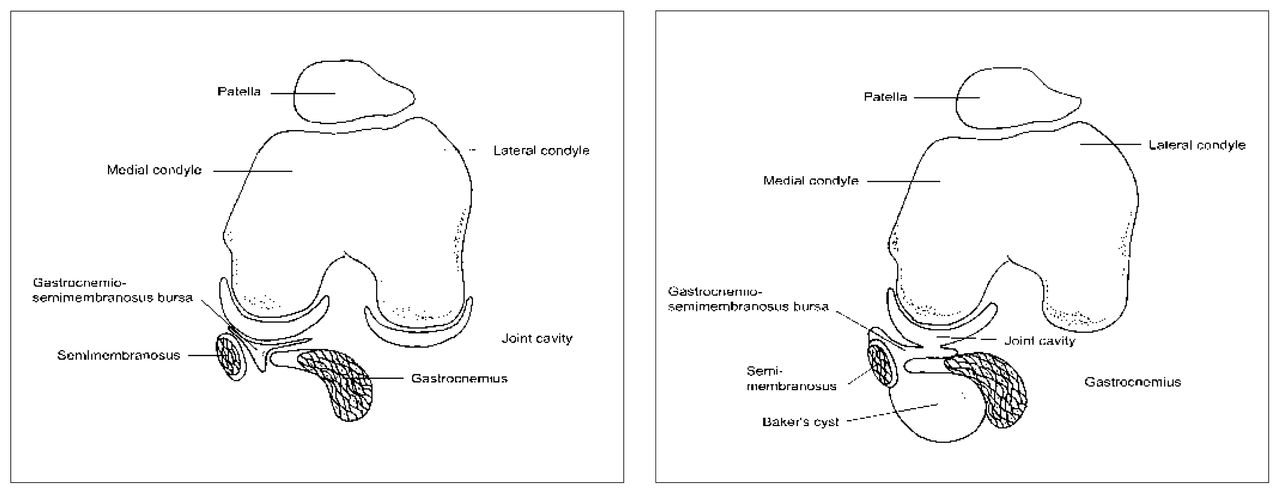
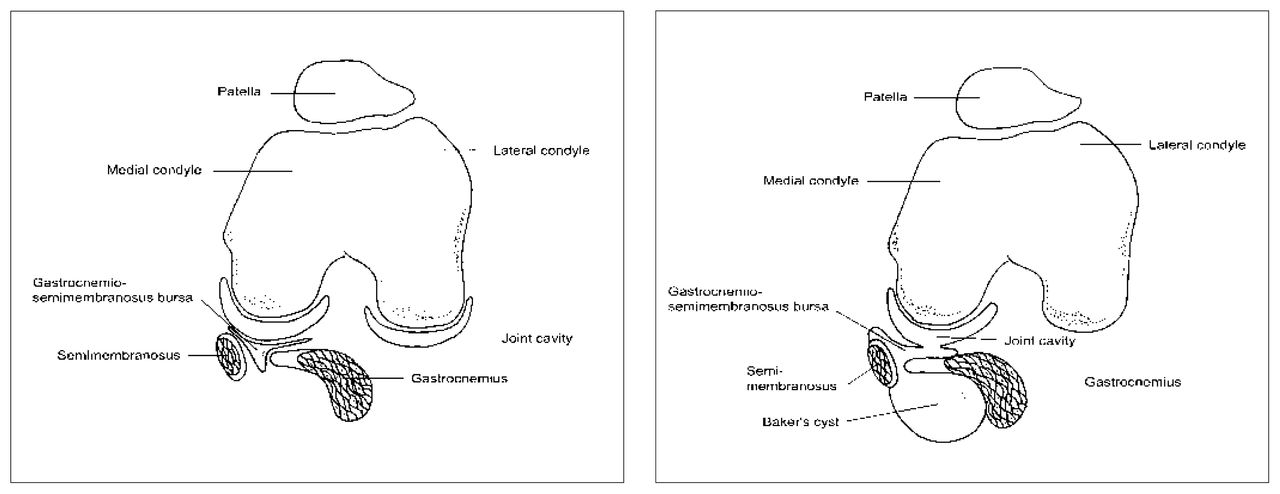
Popliteal cysts (also commonly called Baker cysts) are a frequently encountered synovial lesion. They are often an incidental finding on cross-sectional imaging. Typically, they are encountered in patients who have chronic knee disorders, particularly those producing effusions such as inflammatory and degenerative arthropathies. The elicited effusions result in increased pressure within the joint that forces fluid through a weakened postereomedial joint capsule into a potential space between the medial gastrocnemius and semimembranosus muscles.1,2 A small bursa known as the gastrocnemio-semimembranosus bursa that normally exists at this site (Fig. 2, left) then establishes communication with the knee joint (Fig. 2, right). This bursa gradually increases in size and may eventually dissect into surrounding tissue planes. The dissection occurs posteromedially in most instances, with the cyst emerging at the superficial aspect of the gastrocnemius muscle, tracking along the fascia. Dissection, however, may occur anteromedially or laterally, and occasionally cranially into the thigh.
Baker’s cysts may be mistaken for soft-tissue masses. Ultrasonography is often helpful in their evaluation because this investigation demonstrates that the lesion is cystic, although considerable debris may be present. Sequestered loose bodies from within the joint may be encountered.
The cyst may rupture, allowing the extravasation of synovial fluid and degraded blood products into the soft tissues, eliciting an inflammatory response. 3 Clinically, this may resemble thrombophlebitis, and this is well recognized as the pseudothrombophlebitis syndrome. Injection of contrast medium within the joint has been the traditional method for demonstrating Baker’s cysts. In this case extravasation can also be observed. Ultrasonography is another widely used modality. It is currently in favour because it demonstrates the cystic nature of the bursa and its relation to the joint. The inflammatory reaction in the soft tissues is particularly well demonstrated by magnetic resonance imaging (MRI), which is sensitive to the presence of edema within soft tissues. A series of 3 axial fat-suppressed inversion recovery images (repetition time 2300 ms, inversion time 150 ms, echo time 14 ms) is shown in Fig. 3. Fig. 3, left, demonstrates the cranial aspect of the cyst between the gastrocnemius (curved arrow) and semimembranosus (straight arrow) tendons. Going inferiorly, the cyst can be seen tracking more superficially over the gastrocnemius muscle and inflammatory reaction is noted at the fascial interface with the subcutaneous fat (Fig. 3, centre, hollow arrow). In Fig. 3, right, spreading of the edematous changes associated with the inflammatory reaction become more evident as they progress further inferiorly (arrows).

The use of MRI is not necessarily required for the diagnosis of a leaking cyst as this diagnosis may sometimes by made by ultrasonography. However, in some cases ultrasonography may not be definitive, in which case MRI may prove useful.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.