


Abstract
Objective: To determine the efficacy and long-term prognosis for operative versus nonoperative treatment of small-bowel obstruction (SBO) secondary to malignant disease.
Design: A chart review.
Setting: A university-affiliated teaching hospital.
Patients: The medical records of all patients with malignant disease as the established etiology of their obstruction who presented to the Sir Mortimer B. Davis-Jewish General Hospital, Montreal, between 1986 and 1996 were reviewed. There were 32 patients accounting for 74 admissions.
Interventions: Selective nonoperative management and exploratory laparotomy, immediate or delayed.
Main outcome measures: The value of nonoperative management and need for operation.
Results: Colorectal and ovarian neoplasms were the principal primary malignant diseases that led to SBO. The median time between diagnosis of the malignant disease and SBO was 1.1 years. At their initial presentation, 80% of patients were treated by operation, but 47% of these patients had an initial trial of nonoperative treatment. Reobstruction occurred in 57% of patients who were operated on compared with 72% of patients who were not. The median time to reobstruction was 17 months for patients who underwent operation compared with 2.5 months for patients who did not. Also, 71% of patients were alive and symptom free 30 days after discharge from operative treatment compared with 52% after nonoperative treatment. Postoperative morbidity was 67%. Mortality was 13%, and 94% of patients eventually died from complications of their primary disease.
Conclusions: SBO secondary to malignant disease usually indicates a grim prognosis. Operative treatment has better outcome than nonoperative management in terms of symptom free interval and reobstruction rates. However, it is marked by high postoperative morbidity. We recommend that, after short trial of nasogastric decompression, patients with obstruction secondary to malignant disease be operated on if clinical factors indicate they they will survive the operation.
Small-bowel obstruction (SBO) secondary to malignant disease is often a sign of end-stage disease. It is almost invariably associated with very poor survival.1 Treatment of such patients presents a dilemma for the surgeon. Operative attempts to relieve the obstruction result in significant morbidity and mortality and have limited success in relieving symptoms.2 On the other hand, nonoperative management is often ineffective and, when relief is obtained, early reobstruction often occurs.1–7 This retrospective study looks at a cohort of patients who presented with SBO secondary to malignant disease (not just patients with a history of malignant disease) over the past 10 years and examines the nature and outcome of their treatment as well as their patterns of recurrence. The goal of the study was to examine the efficacy of operative versus nonoperative management of such obstruction and to suggest management strategies for these patients.
Patients and methods
The medical records of all patients hospitalized at The Sir Mortimer B. Davis-Jewish General Hospital in Montreal between January 1986 and December 1996 with a discharge diagnosis of bowel obstruction were reviewed. Patients with the particular diagnosis of SBO were selected from this group. No distinction was made between complete and partial obstruction. All patients whose records indicated a previous admission to another hospital because of SBO were excluded from the study. Our cohort included 552 patients accounting for 1001 admissions for SBO. The etiology of SBO was determined from the clinical presentation and context, operative findings, radiologic findings and the reports of consultants. Patterns of recurrence of SBO as well as the nature and outcome of treatment were documented. The medical records of patients whose obstruction was secondary to malignant disease were re-audited. Information was collected onto forms and than transferred to Microsoft Excel software creating a computerized database from which results were analysed. To assess the merits of operative (group 1) versus nonoperative (group 2) treatment we compared the recurrence rates for each group, length of stay for patients in each group and the postoperative complication rate. To assess patient quality of life after treatment for SBO, we looked at the percentage of patients who were symptom free 30 days after treatment. Our small study population precluded statistical analysis.
Findings
In the overall audit, 5.8% (32) of all patients and 7.4% (74) of all admissions for SBO were the result of malignant disease. This included patients with obstruction due to the primary disease, local recurrence and peritoneal carcinomatosis. Table I shows the various primary malignant conditions that led to obstruction. The median number of admissions per patient was 2.0 (mean 2.3, range from 1 to 6). In 28% of patients with an obstructing carcinoma, intra-abdominal adhesions also partially contributed to obstruction. Patients having associated adhesions did not differ in median number of recurrences from patients who had malignant disease as the sole cause of obstruction. Also, 19% of patients had large-bowel obstruction in addition to their primary SBO. The median age of patients at initial presentation was 63 (mean 62.2, range from 28 to 93) years. Sixty-nine percent of patients were female because of the large cohort having ovarian carcinomas.
Type of Malignant Disease Leading to Small-Bowel Obstruction in 32 Patients
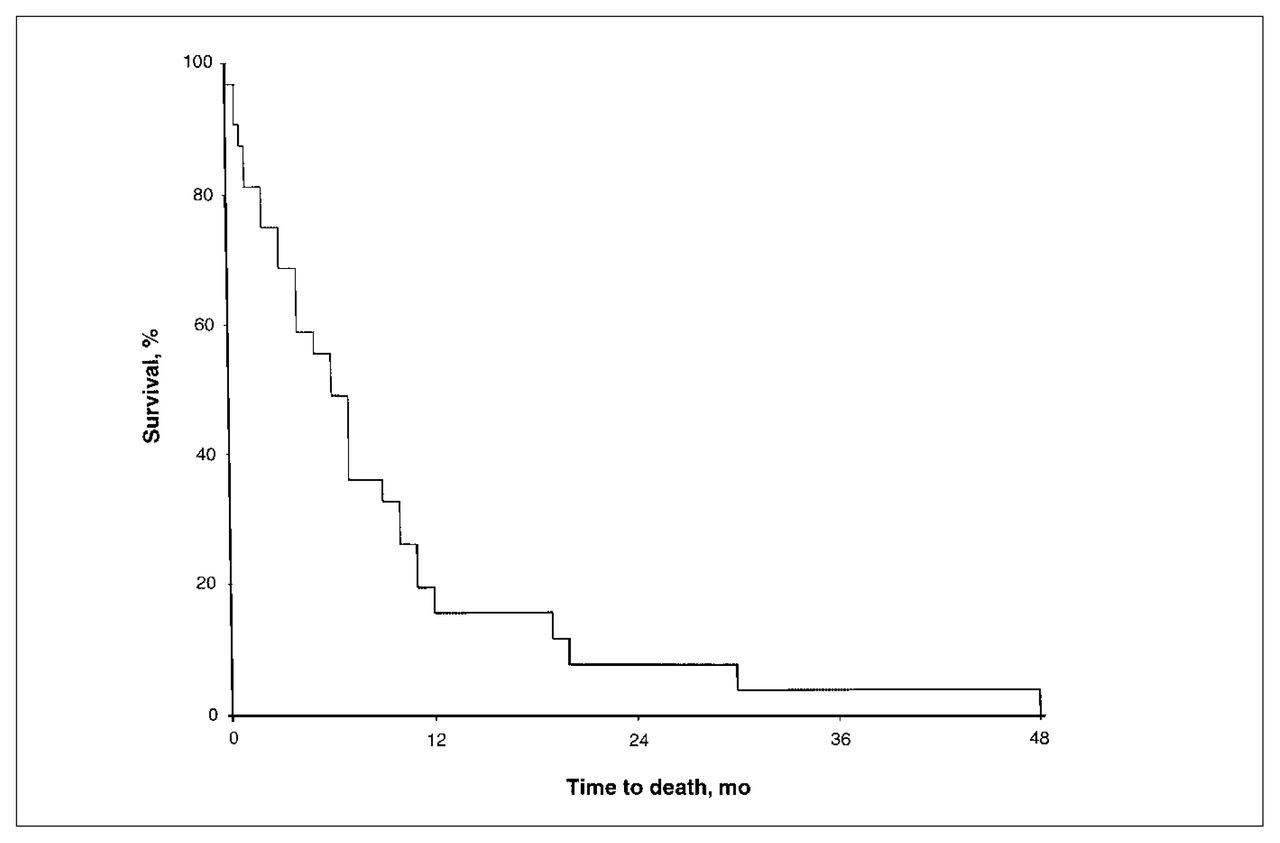
The median time interval from the diagnosis of malignant disease to the development of SBO was 1.1 years (mean 2.6 years). Four patients had SBO as the presenting complaint at the time of diagnosis. These patients had malignant disease of the ovary and colon, retroperitoneal lymphoma and jejunal leiomyosarcoma respectively. The longest interval between diagnosis and SBO was 21 years. Ninety-four percent of patients died from complications related to the primary carcinoma. The 2 patients who survived had a small-bowel lymphoma (11-year follow-up) and jejunal leiomyosarcoma (3-year follow-up). The median interval between the development of SBO and death was 6 months (mean 8.5 months, range from 3 weeks to 4 years). Fig. 1 shows the survival time from initial admission for SBO to death. Nine of the 32 patients died in hospital during an admission for SBO. One patient died early at the first admission, so follow-up data in Figs. 1 and 2 relate to 31 patients.

Five-year survival curve (all-cause mortality) after initial admission for small-bowel obstruction secondary to malignant disease (n = 31).

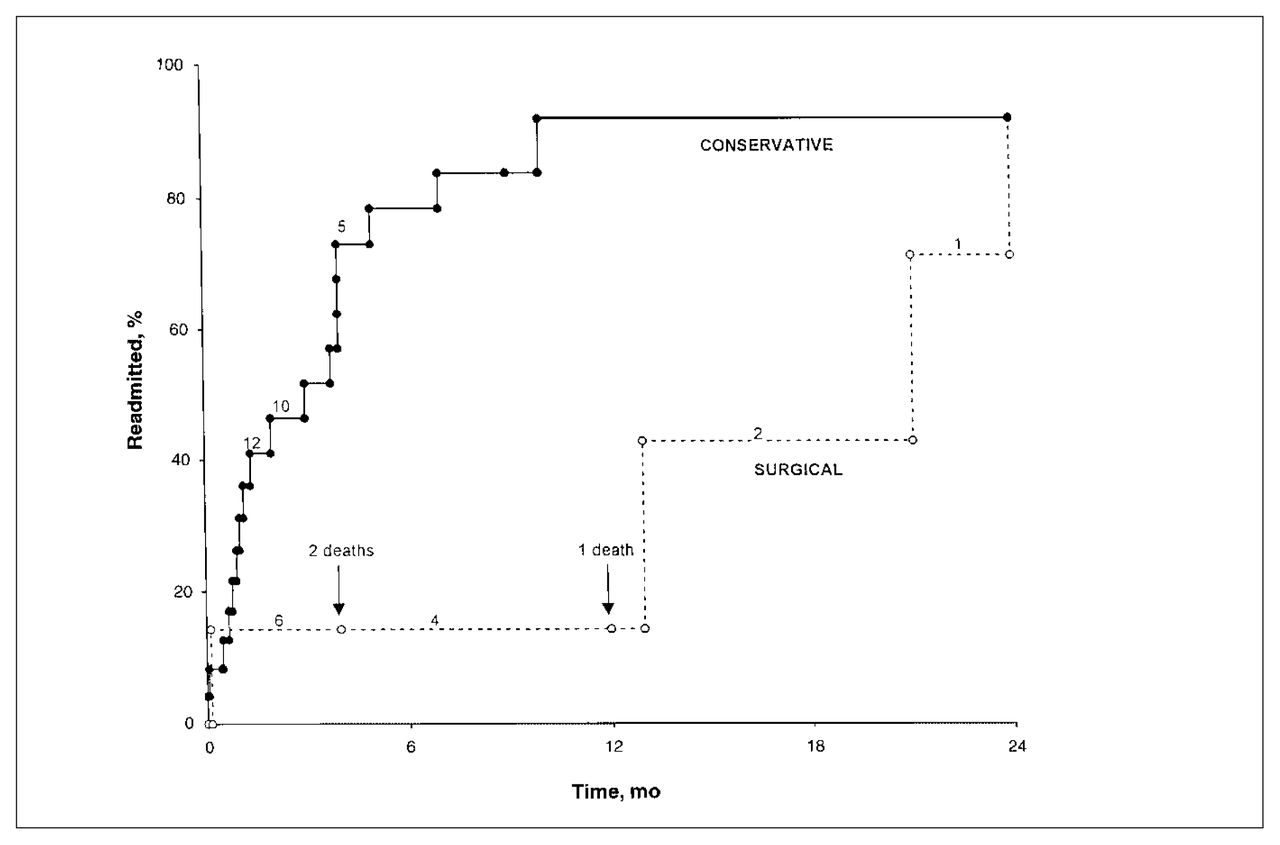
Cumulative frequency of conservatively (n = 24) and surgically (n = 7) treated patients readmitted for bowel obstruction secondary to carcinoma. Patients who were lost to follow-up or died are right censored for the analysis. The numbers above the respective curves represent the number of patients at risk at that particular time. There was a trend for conservatively treated patients to be readmitted sooner.
Fifteen patients (20% of all cases) were treated operatively (Table II). Seven of these 15 were operated on at the time of initial admission (22% of the initial admissions). Seven patients had an initial trial of nonoperative treatment before their operation. The median length of this trial was 4 days (mean 10.3 days).
Type of Procedure Performed in 15 Patients Having Small-Bowel Obstruction
Recurrence rates
To assess the merits of operative versus nonoperative treatment we compared the recurrence rates. Overall, 4 (57%) of operatively treated patients at initial admission required another admission for obstruction compared with 18 (72%) nonoperatively treated patients. The median time to readmission was 17.0 months for patients treated by operation and 2.5 months for patients treated conservatively. Fig. 2 compares the cumulative recurrence frequency of the 2 groups.
Quality of life
With respect to patient quality of life after treatment for SBO, as determined by the percentage of patients who were symptom free 30 days after treatment, 5 (71%) patients treated operatively at initial admission were symptom free and alive 30 days after discharge compared with 13 (52%) nonoperatively treated patients. One (14%) of the 7 patients treated operatively at initial admission required a later operation for obstruction compared with 7 (28%) patients treated nonoperatively. Looking at all admissions, not just the initial episode, the median symptom-free interval after discharge was 6.4 months (mean 7.6 months) after operation compared with 1.1 months (mean 5.3 months) after conservative treatment.
Length of hospital stay and postoperative complications
To further assess the benefits of operative versus conservative treatment for SBO secondary to malignant disease we examined the length of stay for patients in each group and the postoperative complication rate. The median length of a hospitalization was 24 days (mean 30.1 days) for patients treated operatively and 8 days (mean 16.2 days) for those treated nonoperatively. The postoperative complication rate was 67%. Table III lists the frequency of the complications encountered. The median age of patients who experienced complications (68.5 years) was nearly 3 years more than that of patients who were free of postoperative complications. The postoperative death rate was 13%. Causes of death were pneumonia coupled with renal failure and deterioration from the primary carcinoma. Postoperative complications increased the duration of hospitalization by a median of 8 days (mean 10.6 days).
Postoperative Morbidity in Patients Having Small-Bowel Obstruction Secondary to Malignant Disease
Discussion
The management of patients presenting with bowel obstruction after treatment of primary carcinoma when the feared cause is metastatic disease challenges the clinical judgement of even the most experienced surgeon. Inappropriate operation does not improve outcome. Nonoperative treatment is often ineffective in restoring bowel function.3–6 Such patients are often too weak to survive definitive operative decompression.1–4 Stellato and Shenk8 concluded that these patients should be treated as any other patient manifesting intestinal obstruction, the rationale being that 26% to 38% of the bowel obstructions in patients with a history of malignant disease are not secondary to recurrent or metastatic disease and that operative death rates for patients with carcinoma are comparable (9% to 15%) to those of patients presenting with obstruction without a history of carcinoma. The desire to avoid an operation in a patient with a history of malignant disease is tempered by the fact that in 18%4 to 39%4,7,9 a benign correctable condition, such as adhesions or radiation enteritis might be causing the bowel obstruction. Differentiation among these conditions is essential because of the dramatically differing long-term outcomes.4 Even with peritoneal carcinomatosis, Annest and Jolly5 reported that operative decompresion is usually possible and death is usually not caused by reobstruction. In our series, as well as those of others,3,5,6 colorectal and ovarian carcinoma account for most primary malignant neoplasms that lead to obstruction. Colorectal carcinoma is associated with the lowest operative death rate of 13%, with a median patient survival of 10 months.1
At initial admission, nasogastric decompression was successful in only 20% of our cases. Although 10% to 30% of patients obtain relief of obstruction by nasogastric decompression (two-thirds within 3 days), 40% require operation. More than 35% of those with obstruction due to recurrent carcinoma obtain relief of their symptoms with operation. Osteen and colleagues3 recommend a maximum 3-day trial of conservative treatment before operation becomes essential. Tang and colleagues7 reported a greater success rate for nonoperative treatment in patients having partial obstruction (45%) than in those having complete obstruction (3.8%). However, since the distinction between complete and partial obstruction is difficult in a retrospective study because clinical and radiologic features depend on the time course and degree of obstruction,10 we did not distinguish between complete and partial obstruction. Also, in 2 recent large series of SBO,11,12 the authors did not find a significant difference in outcome or recurrence between complete and partial obstruction.
Although the overall prognosis is poor with obstruction secondary to malignant disease (median survival 1.1 years), the outcome for our 7 patients treated operatively at the initial admission was better than for those treated nonoperatively (25). The reobstruction rate was 15% higher for the nonoperative group, the time to reobstruction was 63 weeks earlier (nonoperative group 10 weeks versus operative group 68 weeks), the reoperation rate was twice than that for patients operated on at first admission, and the 30-day obstruction-free rate was 19% lower for patients treated nonoperatively. Other reports6,7 also found longer obstruction-free survival and lower recurrence rates for patients treated nonoperatively. Although the outcome in terms of reobstruction and disease free interval appears to be better with operative treatment, our high (67%) postoperative morbidity makes operation a serious venture. Our death rate of 13% was similar to rates reported in other series (12% to 28%).13 Predictors of poor outcome include the presence of shock, ascites or an abdominal mass, which are associated with death rates of 100%, 70% and 54% respectively.8 Known carcinomatosis has a 40% 30-day death rate. van Ooijen and colleagues13 reviewed the management of 59 patients with intestinal obstruction (38 patients with advanced carcinoma of the ovary and 21 patients with peritoneal carcinomatosis of other organs). They concluded that operation for the relief of intestinal obstruction should only be considered in patients who do not present with ascites or palpable masses and in patients with carcinoma of the ovary for whom effective chemotherapy is available. The rationale is simply that patients with masses or ascites had a median postoperative survival of only 36 days. Percutaneous gastrostomy should be the method of choice for other patients.
Although the overall prognosis is poor in patients with malignant obstruction (median survival 6 months), operation still offers the best hope for palliation.8 Lau and Lorentz14 believe that a more aggressive approach is appropriate. In a review of 30 patients with unresectable intra-abdominal disease, 63% had bowel function restored. Obstruction recurred after a mean symptom-free interval of 120 days in 8 of 19 patients initially relieved. Another operation was performed on 3 of these patients. The authors believe that their results, with a median survival of 192 days for those who benefited from operation, justify a more positive approach to this problem and when conservatism fails, laparotomy should be undertaken in patients who are not terminally ill.
Butler and associates2 also advocate an aggressive approach. They reviewed 54 patients with SBO who had a previous diagnosis of carcinoma. Forty patients were initially treated nonoperatively, and in 28% of those the obstruction resolved after a mean 7 days of nasogastric suction. Five had recurrent SBO. Thirty-seven patients underwent laparotomy, at which time 68% were found to have obstruction due to recurrent carcinoma, which was associated with a mean survival of 5 months. Major postoperative complications occurred in 48% of patients, the most common being failure of the obstruction to resolve. The 30-day and in-hospital death rates of 25 surgically treated patients were 24% and 28% respectively. The authors concluded that (1) patients should be given an initial trial of nonoperative therapy, (2) patients with no known recurrence or a long interval to development of small-bowel obstruction should be treated aggressively with early operation if nonoperative treatment fails, and (3) for patients with known abdominal recurrence in whom nonoperative therapy fails, the results of operative palliation are poor.
August and associates15 reported on the use of home parenteral nutrition in patients with inoperable bowel obstruction secondary to malignant disease. In a review of 17 patients so treated, most patients and families (82%) regarded the therapy as beneficial, with a median survival of 90 days. Also, at times, because of diffuse involvement of the intestine by carcinomatosis, a percutaneous endoscopic gastroscopy (PEG) may avoid the need for celiotomy. When used selectively, PEG can improve the quality of life of the patient by relieving intractable vomiting and by providing an avenue for nutrition in a partially functioning gastrointestinal tract.
Recently, Parker and Baines1 questioned the philosophy of the compulsion to operate on the assumption that obstruction always demands operative intervention. The authors point out a death rate of 13% (identical to our operative mortality) with a median survival of 10 months, but in malnourished patients the death rate can climb to 72%. Emergency operation increases the death rate threefold and, although survival may be increased by a few months, the relief of symptoms lasts only 2 months overall. To counteract these depressing data, good prognostic factors include an early stage or low-grade initial lesion, a long interval from first operation, a wellnourished patient and the fact that in one-third of patients with previous carcinoma, the obstruction is caused by benign disease.
Conclusions
Operation on a patient with obstruction secondary to carcinoma has benefits in terms of survival and quality of life. However, because of the risks of operation in this patient population and the high complication rate, an initial trial of nonoperative decompression is appropriate,16 especially in patients who are at poor risk for survival. Poor-risk patients include those with shock, ascites and an abdominal mass, and those who are terminally ill. On the basis of this review, definitive guidelines are difficult to propose. A suggested algorithm is provided in Fig. 3. In the final analysis meticulous patient selection and mature caring surgical judgement are key factors in the decision to operate.

Suggested algorithm for the management of patients with small-bowel obstruction secondary to carcinoma. PEG = percutaneous endoscopic gastroscopy.
Footnotes
Presented at the annual meeting of the Canadian Association of General Surgeons, Montreal, Que., Sept. 24, 1999.
- Accepted January 24, 2000.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.