


Abstract
During adolescence the spine undergoes rapid growth and changes in anatomy and biomechanical properties. Fractures of the adolescent spine are relatively uncommon but may give rise to serious problems. This review describes thoracolumbar fractures in adolescents with respect to epidemiology, anatomy, mechanisms of injury, clinical and radiologic assessment, and nonoperative and operative treatment. The treatment of these injuries follows many of the same principles as spinal fractures in adults but nonoperative treatment is used more frequently because there is less spinal instability and better tolerance of bed rest and spinal immobilization in this young population.
Injuries to the spine are rare in young children but increase significantly in adolescence. From 12 to 17 years of age, the child’s spine undergoes rapid growth and change in its anatomic, radiographic and biomechanical properties as it approaches skeletal maturity. The purpose of this article is to describe the epidemiologic characteristics of spinal injuries in adolescents, their unique anatomic and radiographic characteristics, the mechanisms of injury, and the clinical and radiographic evaluation of these injuries. The principles of nonoperative and operative management of injuries to the adolescent thoracic and lumbar spine will be outlined.
Epidemiologic features
Pediatric spinal fractures represent between 2% and 5% of all acute spinal injuries. The majority of thoracolumbar spine fractures in the pediatric population occur in children aged 14 to 16 years of age.1 The most frequently injured area of the spine is T4 to T12, followed by T12 to L2.2,3 McPhee3 found that in children under 15 years of age, the majority of spinal trauma occurred in those over 12 years of age, usually secondary to falls from a height and to motor vehicle accidents. Neurologic injury occurred in 14% with multiple-level vertebral fractures noted in 35%. Hadley and associates2 found that motor vehicle accidents were the most common cause of spinal fractures in children aged 10 to 16 years, followed by falls and sports injuries.
The following injury data were obtained from the database of the Canadian Hospitals Injury Reporting and Prevention Program (CHIRPP), Health Canada, from 10 pediatric and 6 general hospitals from across the country. Data collection began in April 1990. In April 1999 (the most current data available on adolescent spinal injuries), the entire CHIRPP database was searched for records of spine and spinal cord injuries suffered by youths aged 12 to 17 years. Six-hundred and ten cases were identified. There were no distinguishable patterns of injury by the time of day, day of the week, month or year of the injury. Injuries were most prevalent in those aged 14 to 16 years, and the majority occurred in boys (63%) (Table 1). Most injuries occurred during recreational or sport activities (53%) followed by motor vehicle accidents (26%). Falls from heights were involved in 13%. Fourteen percent of all spinal injuries occurred at home. Hospitalization was required in 60% of cases. Fractures were documented in 67%, and 26% had an associated neurologic injury. Multiple injuries were sustained in 34% of patients seen in emergency departments and in 43% of those who were admitted to hospital.
Age and Sex Distribution of Injuries
Anatomy
The spine in the adolescent differs from that of an adult in numerous respects. Children mature at variable rates and a wide variety of skeletal maturity is possible across the adolescent age group. The spine of a 12-year-old boy at a Risser stage of 0 differs greatly from that of a 13-year-old girl of Risser stage 4 to 5 who may be in the same school class. At a Risser stage 1, the iliac apophysis has not yet formed and the spine is immature. At a Risser stage 4 the entire apophysis has formed but has not united with the pelvis (Fig. 1). This stage corresponds to the end of spinal growth. Each vertebra has 3 ossification centres, a centrum and 2 neural arches which normally fuse between the ages of 2 and 6 years. If this fails to occur a spina bifida occulta is seen. In the immature spine the facet joints are more horizontal and incompletely ossified, which results in more spinal mobility. They achieve a mature configuration by 8 years of age, but the full, more oblique adult pattern is not seen until 15 years of age. The vertebral bodies may appear slightly wedged, particularly in the thoracic spine because of incomplete enchondral calcification at the end plates. The epidural sac ascends to its normal level opposite L1 in the spinal canal by 1 year of age and the spinal canal attains adult volume by 6 years of age.1

Risser stages of skeletal maturity. Risser stage I is illustrated on the left and stage 4 on the right.
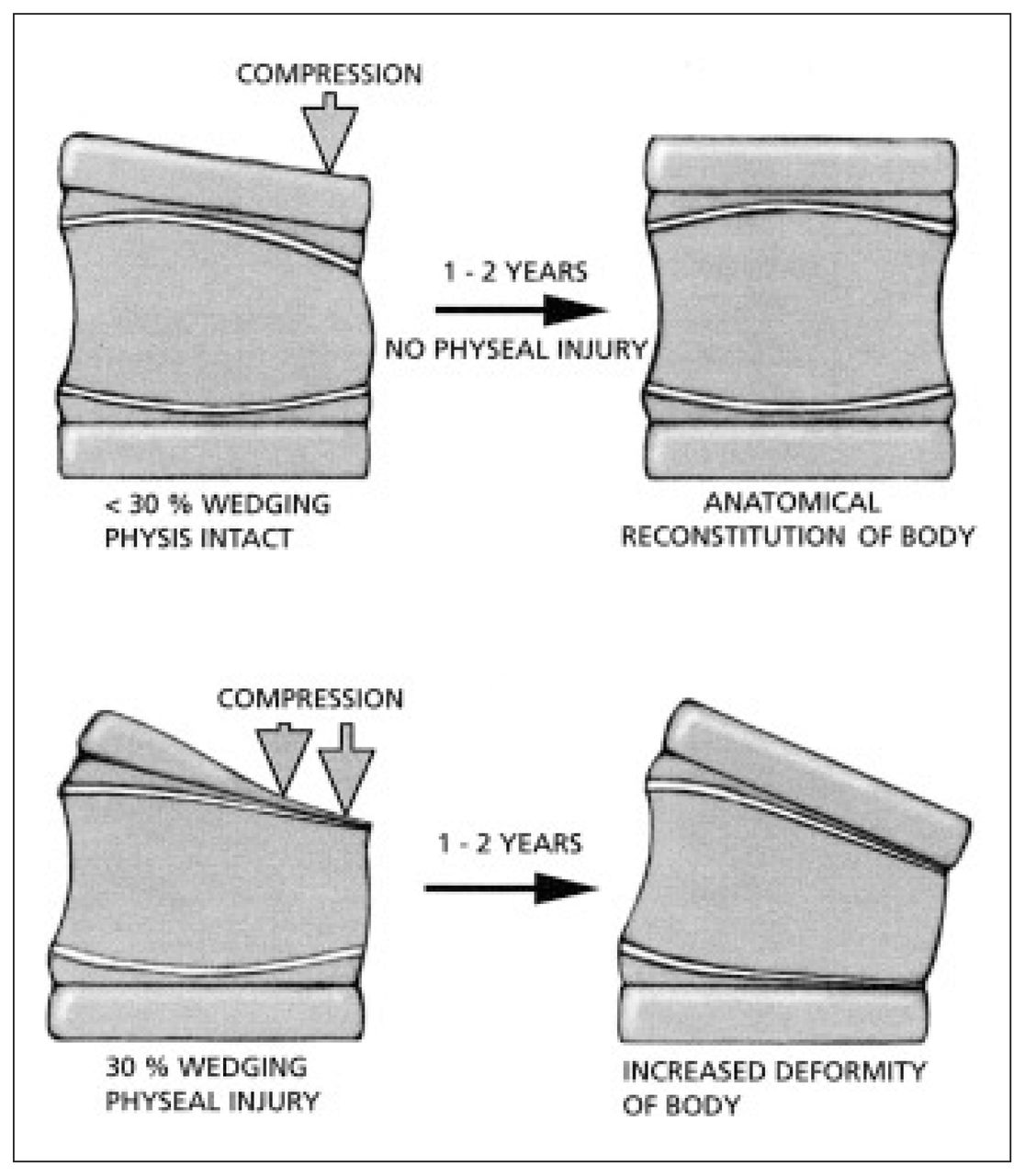
The immature spine is growing and has physes that are part of the superior and inferior end plates. The end plate is composed of hyaline cartilage adjacent to the nucleus and physeal cartilage adjacent to the bony vertebral body. The physes appear radiographically between 8 and 12 years of age when the vertebral apophyseal ossification begins to develop in the periphery of the cartilaginous end plates (Fig. 2). Early in their development they appear as rings because they are thicker at the periphery than at the centre. The ring apophysis contributes to vertebral body breadth and the physeal portion contributes to the vertical height. The end plates begin to fuse when the child is 14 to 15 years of age and may be confused with fractures until fusion occurs at 21 to 25 years of age (Fig. 3). Following a vertebral fracture in children under 12 years of age, stimulation of vertebral growth with overgrowth and complete reconstitution of normal shape can occur. The amount of wedging that will remodel is limited to less than 20° το 30°. If the end plate is damaged or changed, or partially fused, an increase in deformity may occur, especially during the rapid adolescent growth spurt (Fig. 4). Anatomic studies by Aufdermaur4 demonstrated that fractures of the immature spine traverse the growth zone of the physis similar to long bone physeal fractures. In flexion– distraction type injuries of the spine a Salter–Harris type 1 injury may occur through the weaker physis.1 However, because it occurs through a physis, healing potential is excellent, unlike a similar injury in the adult spine.
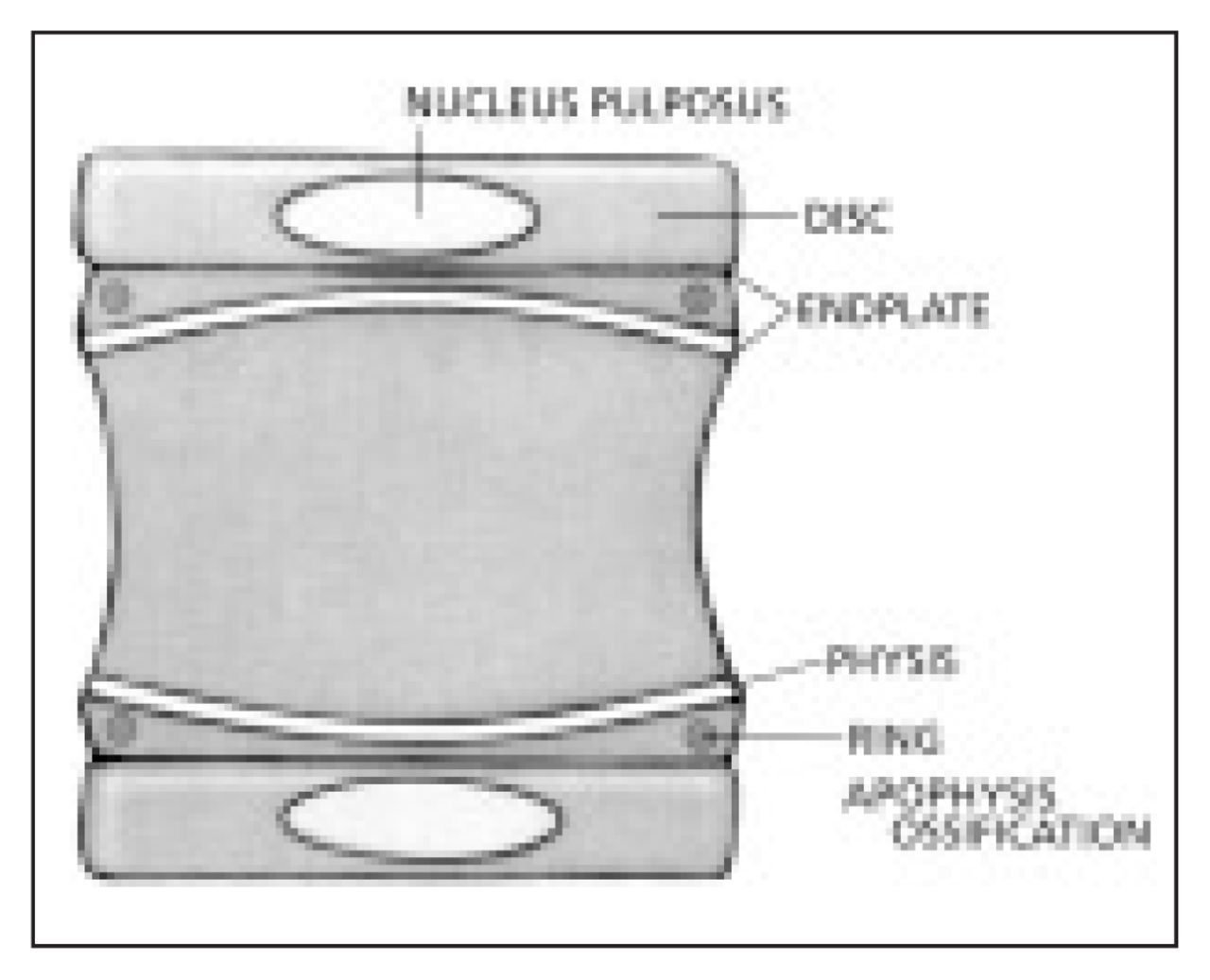
Anatomy of the adolescent vertebra.

The spine of a 13-year-old boy, illustrating the ring apophysis ossification (arrows).

Effects of vertebral physeal arrest on further physeal growth. Top: with less than 30% wedging physeal injury is uncommon. Bottom: with over 30% of wedging, physeal injury frequently occurs.
Fractures of the lumbar vertebral apophysis also occur and can herniate into the spinal canal and present with low back pain and neurologic findings similar to a disc protrusion seen in adults.5,6 Slipping of the vertebral apophysis occurs in the same age range as slipping of the capital femoral epiphysis, when these physes are thicker and weaker due to rapid growth, and may also be associated with anterior lumbar end-plate compression or Scheuermann’s disease of the lumbar spine in 38%.7 After physeal closure and cessation of spinal growth a weak zone no longer exists in the spine, and failure occurs through the bony vertebral body or the anulus fibrosus and the disc space.
The anulus does not fail in the immature spine. The immature intervertebral disc is more hydrophilic than the mature disc, allowing it to be a more effective shock absorber between the vertebral bodies. In children the disc is a very firm structure and much more resistant to injury than the vertebral body. The vertebral body with its cancellous and vascular centrum also acts as a shock absorber before compressing or bursting. Roaf8 in 1960 demonstrated that the cartilaginous end plate often fails first, allowing herniation of the nucleus into the vertebral body creating Schmorl’s nodes rather than herniating into the spinal canal as in adults (Fig. 5). In older adolescents, compression force is transmitted through the anulus so diffuse collapse or bursting of the body may be seen. The more elastic disc also allows compression force to be transmitted as a wave over multiple levels such that multiple compression fractures are more common in children and adolescents than adults.2,9–11 (Fig. 6) In spite of some differences, by the age of 10 to 11 years the mechanical and anatomical characteristics of the child’s thoracolumbar spine approach that of an adult, and fracture patterns are the same. The 3-column theory of Denis12 is therefore applicable to the adolescent age group.
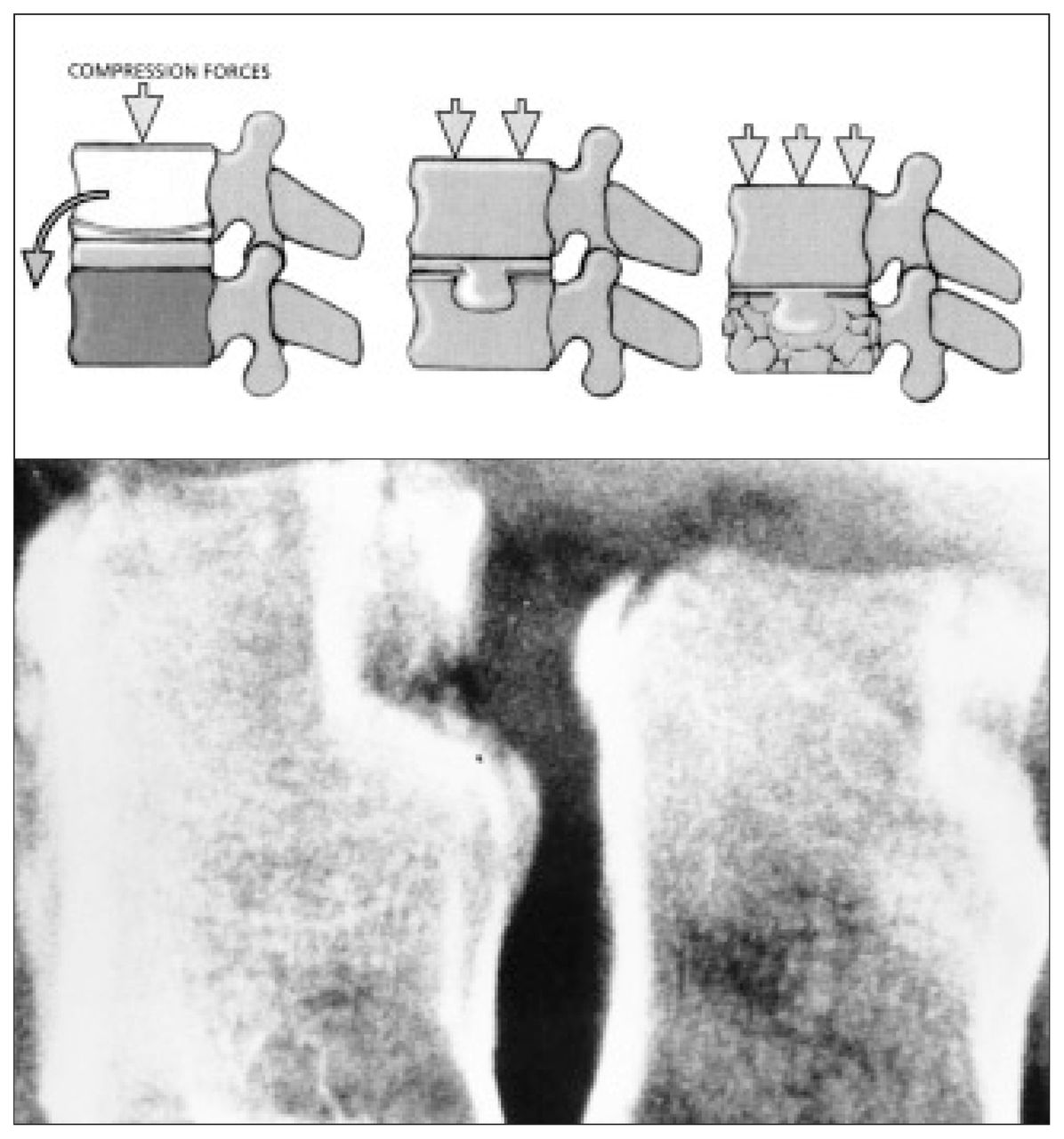
Biomechanical response of the vertebra to excessive axial loading. Top left: asymmetric loading may result in collapse of a portion of vertebra — usually anteriorly. Top centre and bottom left: compression may result in the nucleus pulposus being forced into the body — a so-called Schmorl’s node. Top right and bottom right: severe compression may result in a more typical burst fracture of the vertebral body.

Lateral view of the lumbar spine of a 15-year-old boy, showing fractures at multiple levels.
According to Denis,12 the anterior longitudinal ligament, the anterior anulus fibrosus and the anterior part of the vertebral body form the anterior column. The posterior longitudinal ligament, the posterior anulus fibrosus and the posterior wall of the vertebral body form the middle column. The posterior column is formed by the posterior elements of the spinous and transverse processes, the lamina, facet joints and pedicles alternating with the posterior ligamentous complex, consisting of the supraspinous ligament, interspinous ligament, capsule and ligamentum flavum.
Mechanisms of spinal injury
There are 3 main mechanisms of spinal injury seen in children: flexion, with or without compression; distraction; and shear.10 Hyperflexion injuries are most common. Hyperflexion results in a compression failure of the anterior column, leaving the middle column intact. The posterior column may be intact but becomes distracted with greater degrees of flexion. In Denis’s study12 the largest number of fractures occurred at L1. Radiographically, there is no loss in height of the posterior aspect of the vertebral body. When vertically loaded, the end plate distorts first, blood is forced out of the highly vascular cancellous bone, normally a shock-absorbing mechanism. With increasing force the nucleus is forced through the end plate and a radiographic appearance of narrowing of the disc space is seen. In older adolescents, the forces are transmitted to the anulus and bursting or collapse of the vertebral body occurs. Scheuermann’s kyphosis, with anterior wedging of 3 consecutive vertebral bodies greater than 5° and the presence of Schmorl’s nodes should not be misinterpreted as acute trauma.
In burst fractures the anterior and middle columns both fail under axial load and compress. Radiographically there is fracturing of the posterior wall cortex with retropulsed fragments into the spinal canal from either or both end plates. There is an increase in the interpedicular distance as well as a vertical laminar fracture and splaying of the posterior joints. Denis12 has described 5 subtypes (Table 2).
Classification of Burst Fractures (Denis12)
In adolescents, pure compression may cause slipping of the apophysis. Three types have been described.6 In 11- to 13-year-old children, a cartilaginous ring is extruded posteriorly into the spinal canal and is seen as a fine crescent on CT. In 13- to 18- year-old children, an avulsion fracture of the posterior rim of the vertebral body and anulus is seen. Small, localized fractures are seen in those over 18 years of age (Fig. 7).

Fractures of the ring apophysis.
Seat-belt fractures result from distraction of the posterior and middle columns as hyperflexion occurs over a lap belt during rapid deceleration when the belt is applied over the abdomen. Failure may occur through bone, soft tissue or the apophysis. The anterior column may or may not be intact depending upon the distance of the fulcrum from the anterior aspect of the vertebra11,13,14 (Fig. 8).

Seat-belt fracture, a flexion–distraction injury. A: in a child with a thin abdominal wall, the fulcrum (arrow) is virtually at the body of the spine. Fracture may occur through the end plate and the posterior ligamentous complex. B: in an adult with a thicker abdominal wall, the fulcrum may be 12 to 20 cm anterior to the spinal column. The classic Chance fracture occurs through the vertebral body and posterior spinous process.
Acute fractures of the pars interarticularis are usually the result of repetitive hyperextension stresses in gymnastics, weight lifting and football but may occur after relatively minor trauma in a previously weakened area. Once this spondylolysis has occurred, forward translation of the above spinal segments may occur. This spondylolisthesis, seen at the L5 to S1 level most commonly (97%), should not be misinterpreted as an acute fracture–dislocation.15 In shear injuries there is typically fracture through the end-plate apophysis before it fuses. These result in fracture–dislocations with failure of all 3 columns described by Denis,12 frequently associated with spinal cord injury.
Clinical evaluation
With respect to clinical assessment of spinal fractures in adolescents, several important points should be considered. First, pediatric Advanced Trauma Life Support (ATLS) protocols and evaluation must be adhered to because of the high incidence of associated injuries with these fractures, particularly if they are related to the use of seat belts. A complete history must be obtained. Most adolescents with a fracture of the thoracolumbar spine will complain of significant back pain and should be able to localize it.
It is important to know:
What is the age and spinal maturity of the patient?
What were the circumstances of the injury and what was the amount of energy involved. (i.e., a fall on ice versus a 10-m fall off a cliff on a snowboard) and the length of time since the injury ?
Are there any symptoms of pain, tingling, numbness or loss of sensation and weakness in the extremities and, if these were transient, how long did they last?
Did the patient get up or walk after the injury and how was the patient transported to the hospital?
Has the patient voided urine, and if a catheter was placed could the patient feel it being placed?
Is there any abdominal, chest or extremity pain?
Any allergies, immunizations, medical problems especially bleeding disorders, asthma, diabetes or seizures, the dates of any previous surgical procedures or fractures and any complications should be noted to complete the history.
The physical examination should follow the ABCDs of the ATLS protocol to avoid missing associated injuries. In the polytraumatized adolescent, a spinal fracture may be overlooked or detected late. Fractures of the transverse process are associated with serious abdominal injury in 20% of cases as are lap-belt injuries in 50% to 90%, including small-bowel rupture and traumatic pancreatitis.16 Abdominal seat-belt abrasions should be carefully noted especially if they are in a lap-belt distribution. During initial screening for neurologic deficits, test light touch with a wisp of cotton in all 4 extremities in addition to asking the patient to move all fingers and toes. This should be followed by: (a) formal testing of pain sensation with a sharp broken wooden tongue depressor in a dermatomal fashion; (b) reflex testing of the upper and lower extremities; and (c) strength testing in a myotomal fashion. Reflexes should be graded as absent, present, brisk or exhibiting clonus. Strength is graded out of 5 points (Table 3) to evaluate nerve root function. Great toe and foot plantar flexion corresponds to S1, great toe dorsiflexion L5, ankle dorsiflexion L4, knee extension L3 and hip flexion L2. A score out of 50 can be obtained by adding up the scores for both lower extremities.
Motor Power Grading
The patient must be log rolled, inspecting the entire posterior spine for marks, bruising or swelling. The entire spine is palpated for tenderness and widening or steps between spinous processes. The examiner must watch for injuries at multiple levels. A rectal examination is then performed and the bulbocavernosus reflex is checked by applying gentle traction to the Foley catheter or squeezing the glans of the penis in males and feeling for contraction of the anal sphincter. Absence of this reflex indicates the presence of spinal shock. Sensation in the anal region must always be tested to identify sacral nerve-root sparing. If a neurologic deficit is identified the patient should be started on intravenous methylprednisolone immediately to minimize cord edema.17 This should be given as a 30 mg/kg bolus over 15 minutes followed by a 23-hour infusion at an hourly rate of 5.4 mg/kg. Patients treated with methylprednisolone within 8 hours of injury have significantly improved neurologic function over patients treated with a placebo in controlled clinical trials at 6 weeks, 6 months and 1 year after the injury.17 If a neurologic deficit is noted, the Frankel classification (Table 4) may also be used to grade the degree of paraplegia. All examinations must be recorded, preferably on a spinal injury examination protocol sheet, so that serial examinations of the patient can be monitored and compared.
Frankel Classification of Degree of Paraplegia
Radiographic evaluation
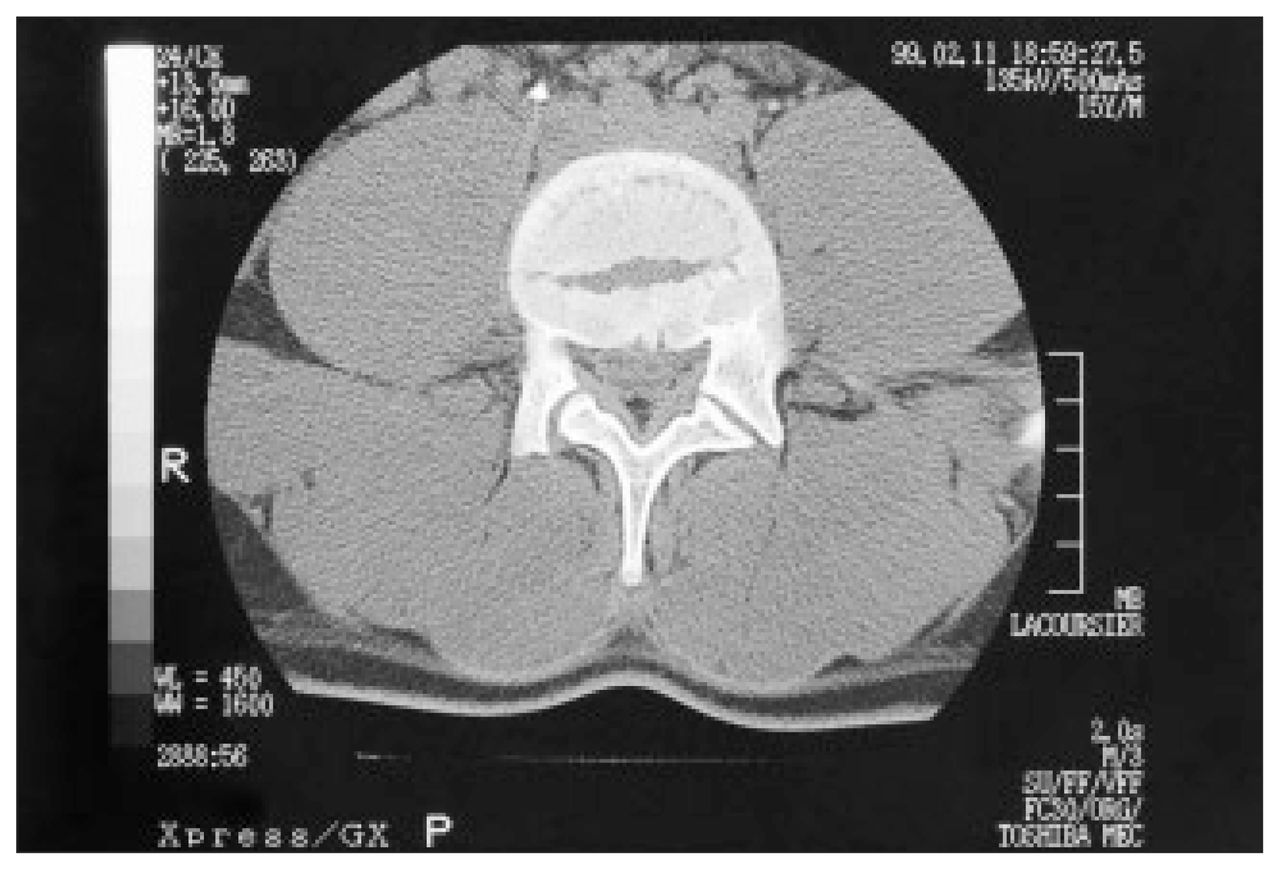
Most spinal fractures in adolescents are demonstrable on plain radiographs. Once identified, the level of the injury should be investigated further by CT in most cases (Fig. 9). The definition available on CT is often necessary to determine the status of the middle column. In burst fractures and those associated with a neurologic deficit, the degree of canal compromise is determined by comparing the amount of retropulsed bone in the canal to the canal width of the levels above and below the fracture.

A CT scan often will delineate the vertebral fracture more clearly than a plain radiograph as shown here.
If a neurologic injury has been sustained MRI should be done to assess the extent of injury to the spinal cord and the soft tissues. Three patterns are seen on T2-weighted images: decreased signal associated with acute hemorrhage, a bright signal indicating cord edema (Fig. 10) and a mixed signal consistent with contusion. Transection of the cord is readily seen as well as compression by hematoma, the ligamentum flavum or disc material in older adolescents. Because of the flexibility of the immature spine a spinal cord injury may be sustained without any radiologic signs of injury. This occurs in about 20% of pediatric spine injuries13,18,19 but drops to 0.2% in adults.20 As the adolescent spine matures and behaves more like the adult spine, the incidence of cord injury without radiologic signs falls to adult levels.

Spinal cord injury is best identified with MRI, which will identify the extent of cord edema and hemorrhage as shown here.
Radiographic evaluation is also used to determine the stability of the injury. If the patient is neurologically intact and has sat up and walked since the injury, the fracture is likely to be stable. An unstable injury is one that may angulate with time into an unacceptable position or result in neurologic compromise. By definition, if there is a neurologic injury, the spine is considered unstable. Denis’s 3-column theory12 provides guidelines to stability. To be unstable 2 or more columns must be disrupted. In general a fracture will be stable if the middle column is intact and unstable if it is disrupted, with the following exceptions: in fractures of the thoracic spine involving the middle column above T8, if the sternum and ribs are intact the injury is splinted and tends to be stable; at L4 and L5, if the posterior elements are intact or have only longitudinal fractures the injury will be stable if normal lumbar lordosis can be maintained; distraction injuries will behave as stable injuries in adolescents after initial soft-tissue healing, or healing of the growth plate. Fractures through bone at this level are usually very stable because of inter-digitation of the fracture surfaces.
Mechanical instability also applies to injuries in which the neural elements are not threatened but progression of deformity may occur. These fractures include severe compression fractures and seat-belt fractures in which the posterior ligamentous structures are disrupted. This includes any fracture with loss of more than 50% of the height of the anterior column but an intact middle column. More than 20° of flexion of L1 on L2 indicates complete disruption of all posterior ligaments and instability. Neurologically unstable fractures are those in which the middle column has ruptured under an axial load. Most neurologic injuries result from the initial trauma, but ongoing compression of neurologic elements may occur with fragments in the spinal canal. Any fracture in which there is disruption of the middle column and all burst type fractures are at risk of further neurologic injury if axial load is applied before the fracture is healed, even if the patient is initially neurologically intact. Mechanical and neurologic instability is represented by fracture–dislocations and severe burst fractures by neurologic deficit. These are usually fractures with more than 15° of kyphosis, more than 40% loss of vertebral height and more than 40% compromise of the canal.
There are 5 specific radiographic findings that imply instability21 applicable to the adolescent spine: vertebral body collapse with widening of the pedicles; greater than 33% canal compromise by fragments of the lamina or the middle column on CT; translation of more than 2.5 mm between vertebral bodies in any plane; bilateral facet dislocation; and abnormal widening between the spinous processes or lamina combined with more than 50% anterior collapse of the vertebral body. The risk of neurologic injury increases with more than 35% canal narrowing at T11 to T12, 45% at L1 and 55% at L2 and below.
White and Punjabi21 developed a checklist to diagnose instability of the thoracolumbar spine. It includes 7 different elements (Table 5). If the score totals more than 5 points, the spine is considered unstable until healed or surgically stabilized.
Checklist for Instability of the Thoracolumbar Spine
Nonoperative treatment
Clinically stable fractures of the spine in adolescents can be safely treated nonoperatively. This applies to minor spinous process and transverse process fractures, wedge compression fractures and flexion-hyperextension (Chance) fractures in which more than 50% of the fracture passes through cancellous bone. Nonoperative treatment comprises short-term bed rest, analgesics and benzodiazepines for muscle spasms. A nasogastric tube is often required should an ileus be present. Once the adolescent patient is tolerating food and is comfortable, mobilization with a thoracolumbosacral orthosis (TLSO) to lessen pain can be started. This is worn for the first 6 weeks after the injury. A Chance fracture requires hyperextension casting and bracing for 8 to 12 weeks to facilitate healing.
Most burst fractures and potentially unstable injuries can also be treated nonoperatively with bed rest. If neurologically intact, canal decompression is not required because the fragments are resorbed.22 A stable burst fracture may be treated by early mobilization in a cast or orthosis. Hyperlordosis pulls the cord away from the fragments. A Jewett brace is inadequate for initial treatment of fractures below the thoracolumbar junction. Fractures of the upper lumbar spine require a TLSO. Fractures of L4 and L5 require a TLSO with thigh extension to prevent kyphosis. An unstable burst fracture treated nonoperatively requires a minimum of 6 to 10 weeks’ bed rest, after which the patient is mobilized in a TLSO for the same length of time so long as the fracture is unchanged in its position as demonstrated on a radiograph through the brace in the standing position.
Nonoperative treatment is contraindicated in several situations. In the adolescent with a complete neurologic injury, stabilization is indicated to prevent progression of deformity with growth and to facilitate nursing care and the early rehabilitation of the patient to life as a paraplegic.23
Operative treatment
In cases of unreduced dislocation or those with partial neurologic impairment immediate surgical stabilization and decompression is indicated to relieve pressure on affected neural elements and to prevent further neurologic deterioration. However, a discussion of all aspects of the operative treatment is beyond the length and scope of this paper. Several principles and controversies of the adolescent spinal injury do warrant discussion. The purpose of operative treatment in the unstable spine is fivefold: to restore anatomic alignment and prevent progressive deformity; to provide early decompression of neural elements in patients with partial deficits; to provide early pain control; to facilitate skin and pulmonary care in the multiply injured youth; and to permit early discharge from hospital. It must be emphasized that 97% to 100% of adolescents with spinal cord injury incurred before the growth spurt develop a scoliosis or kyphosis. Ninety-six percent of the curves progress with scoliosis in 92% and kyphosis in 64% of these. Children injured after the onset of the adolescent growth spurt have a 52% incidence of such deformities.23
The ideal time for surgery is in the first 12 to 48 hours after the injury. The indirect reduction of retropulsed fragments is best achieved before clot formation at 48 hours. Edwards and Levine22 found a 32% improvement in canal area for burst fractures treated within 2 days of injury compared with 23% for those treated between 2 and 10 days and 1% for those treated after more than 2 weeks. The instrumentation chosen should provide the corrective forces necessary with the minimum amount of surgery and the shortest length of instrumentation. This can be achieved with hook and rod constructs or pedicle screws to one vertebra above and one below the fractured level. Anterior plating and strut grafting can be used anteriorly, although access below L4 is difficult due to the proximity of the great vessels. Indirect decompression is possible because the retropulsed fragments are firmly attached to the anulus and posterior longitudinal ligament, particularly in the immature spine, and can be pulled back into position by distraction. Indirect decompression of the spinal canal is accomplished by restoring the anatomic alignment through distraction across the vertebral body followed by hyperlordosis of the injured segment. Approximately 50% of the canal width can be improved in this manner. If canal compromise is greater than 50%, then residual canal narrowing will remain postoperatively. If the posterior longitudinal ligament is completely disrupted, further displacement will result with possibly a worse neurologic injury. Therefore the integrity of the ligament must be determined preoperatively with MRI. A flexion–hyperextension injury (Chance fracture) when stabilized operatively requires compression and not distraction. In the case of Chance fractures in which less than 50% of the fracture passes through bone, posterior compression instrumentation is necessary to facilitate healing of the torn ligamentous structures and prevent late deformity. 22,24–26
Currently, it is believed that severe burst fractures likely require instrumented fusion through an anterior approach if there is 40% or more canal compromise, 40% or greater loss of canal height or kyphosis of 15° or more.27 There is also concern that distraction leaves a large void in the cancellous bone similar to the compression of bone in tibial plateau fractures in adults. Just as bone grafting is required in the knee, so it may be required to fill the void in the distracted vertebrae to prevent late collapse. The technical aspects of the operative approaches and instrumentation are well covered in standard texts and the technique manuals of the particular hardware being used. Because of the variability in size of the patient in the adolescent age group, flexibility in the hardware size is a requirement, although most in this age group can be treated with standard adult spinal instrumentation.
- Accepted May 12, 2000.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.