


1. ARTIFICIAL BOWEL SPHINCTER IMPLANTATION IN THE MANAGEMENT OF SEVERE FECAL INCONTINENCE — EXPERIENCE FROM A SINGLE INSTITUTION
The purpose of this study was to evaluate the safety and efficacy of artificial bowel sphincter (ABS) implantation in the management of severe fecal incontinence (FI).
Ten patients (6 males), with a mean age of 40.6 years, underwent ABS implantation between April 1998 and November 1999. The etiology of FI was imperforate anus (6), obstetrical trauma (3) and trauma (1). All patients failed previous operative and/or nonoperative therapy. One patient had a stoma at the time of ABS implantation. Preoperative evaluation included calculation of the Fecal Incontinence Severity Score (FISS) and anal manometry. Manometry was repeated at activation of the ABS, and both manometry and FISS were performed at 6- and 12-month follow-up visits. Differences in the measures were tested with the repeated measures ANOVA to determine if a difference existed over time, and if ANOVA was significant, further paired comparisons were conducted using a Student’s t-test.
Mean operating time was 2 hours 22 minutes (range: 1 h 30 min–2 hr 50 min), and mean length of stay was 7 days (range 5–13). Two patients have required explantation at 5 and 8 months, because of erosion of the device, and reopening of a rectourethral fistula, respectively. The remaining 8 patients had significant improvement in manometry and FISS. Mean preoperative resting anal pressure (RAP) was 20 mm Hg; mean RAP was 56.6 mm Hg at activation (p < 0.001), 50.7 mm Hg at 6 months (p < 0.001) and 55.3 mm Hg at 12 months (p = 0.001). Mean preoperative FISS was 102.4; mean FISS was 53.4 at 6 months (p = 0.011) and 55.3 at 12 months (p = 0.002).
ABS implantation results in a significant increase in RAP and a significant decrease in FISS. Serious complications leading to explantation were seen in 2 of our 10 patients. ABS implantation is an effective tool in the management of severe FI.
2. COMPARISON OF DELORME AND ALTEMEIER PROCEDURES FOR RECTAL PROLAPSE
We wish to compare the outcomes of 2 perineal operations for rectal prolapse: rectal mucosectomy (Delorme’s operation) and perineal rectosigmoidectomy (Altemeier’s operation).
We reviewed all 34 patients who had a perineal repair of rectal prolapse at our hospital from July 1997 to June 2000. Ten patients had the Delorme operation and 24 patients had the Altemeier operation. Mean age was 44.7 years (22–77) for Delorme and 67.1 years (23–87) for Altemeier operations. Follow-up telephone interviews were conducted for 25 patients (8 Delorme; 17 Altemeier) at a mean of 12.8 and 19.3 months, respectively.
Recurrence of prolapse occurred in 50% patients who had the Delorme (2 full-thickness, 2 mucosal) versus 0% for the Altemeier operation, p = 0.006. Incontinence to solid stool changed from 30% to 38%, preop. to postop., for the Delorme compared with a change of 65% to 29% for the Altemeier operation, p = 0.2. Incontinence scores (Jorge and Wexner, 1993) changed from 7.9 ± 7.0 to 6.7 ± 7.7, p = 0.45, for the Delorme, and 14.7 ± 6.4 to 10.8 ± 8.0, p = 0.01, for the Altemeier operation.
Complications occurred in 2 Delorme versus 6 Altemeier patients with 1 anastomotic stricture in each group, p = 0.68. Hospital stay was 3.0 ± 0 days for Delorme versus 4.6 ± 2.0 days for the Altemeier operation, p = 0.01. Patient satisfaction was rated as excellent or good by 50% of Delorme and 64% of Altemeier patients, p = 0.3.
We conclude that perineal rectosigmoidectomy had fewer recurrences and improved incontinence scores compared with rectal mucosectomy for the treatment of rectal prolapse.
3. ANAL ADVANCEMENT FLAP FOR CHRONIC ANAL FISSURE: A RETROSPECTIVE REVIEW
The aim of this study was to evaluate anal advancement flap (AAF) for the treatment of chronic anal fissure (CAF).
A retrospective chart review from December 1993 to November 2000 identified 21 patients (11 female, 10 male; age 19–72) who underwent AAF for CAF.
Twelve flaps were lateral and 9 were midline covering the fissure. Indications for AAF repair of the fissure included patient preference (8), poor sphincter function (previous surgery [4], trauma [3], idiopathic [4]), and associated anal stenosis (2). There was no mortality. Morbidity included perianal sepsis (1) and flap tip necrosis (1). Two patients required overnight readmission for pain control. One patient with anal stenosis had constipation, which resolved conservatively. Following primary AAF, 20 patients were healed, while 1 required a second AAF for cure. No patient reported incontinence.
Anal advancement flap for chronic anal fissure is a viable surgical alternative to lateral internal sphincterotomy for selected patients, especially those at high risk for postoperative incontinence.
4. FACTORS AFFECTING OUTCOMES FOR THE PELVIC POUCH PROCEDURE IN ONTARIO
The objective of this study was to determine what clinical variables are predictive of length of hospital stay (LOS) and 30-day readmission, reoperation and excision rates following pelvic pouch procedure (PPP) using population based data.
Two population based, administrative databases were used to obtain all demographic, surgical and hospital data for patients undergoing the PPP in Ontario between 1992 and 1998. Logistic regression was used to determine if age, gender, PPP staging (1, 2 or 3 stage), year of PPP or hospital volume (high [HV] >100 PPP; medium [MV] 11–100 PPP; low [LV] ≤10 PPP) were predictive of LOS, 30-day readmission, reoperation and excision rates.
Overall, 1285 PPP were performed. Mean LOS for all stages of the PPP decreased from 21.0 to 18.5 days (p = 0.002) while 30-day readmission rate decreased from 12.8% to 9.9% (p = 0.5). One- and 2-stage PPP had shorter LOS than 3-stage; however, lower stage was also associated with a slight but insignificant increase in 30-day readmission rate. Hospital volume was the strongest predictor of reoperation following PPP. Patients at MV and LV hospitals were 1.66 (95% CI 1.29–2.14) and 3.55 (95% CI 2.17–5.80) times more likely to require reoperation compared to HV hospitals. Age and hospital volume were the strongest predictors of excision following PPP. Patients ≥40 years were 2.19 (95% CI 1.25–3.82) times more likely and those at MV and LV hospitals were 3.35 (95% CI 1.79–6.26) and 3.01 (95% CI 1.16–7.78) times more likely than those at HV hospitals to require excision.
There were decreases in both LOS and 30-day readmission rates following the PPP in Ontario between 1992 and 1998. Patients having surgery at HV hospitals had better outcomes following the PPP compared with those at MV and LV hospitals.
5. HOME TPN — AN ALTERNATIVE TO EARLY SURGERY IN PATIENTS WITH COMPLICATED IBD
A small number of patients undergoing surgery for inflammatory bowel disease require short-term parenteral nutrition either pre- or postoperatively. Some of these patients will require definitive surgery to correct the underlying cause of intestinal failure. Delaying surgery may make a difficult procedure easier, and sometimes surgery may even be avoided. Traditionally patients remain in hospital while they receive this nutritional support. This paper examines the safety and feasibility of providing short-term, home TPN for IBD patients for whom the alternative is prolonged hospitilization or early surgery. A review of all IBD patients receiving temporary home parenteral nutrition from our hospital pharmacy from June 1996 to July 2000 was performed. A quality-of-life phone questionnaire was conducted at the time of review. Fifteen patients (11 males, 4 females) were identified, average age 35 years. The underlying diagnosis was Crohn’s disease in 10 and ulcerative colitis in 5. Indications for TPN varied. Two patients received preoperative home TPN for complex internal fistulae and resolving sepsis. Twelve patients received home TPN after undergoing surgery during that admission. Five developed septic complications (anastomotic leak/enterocutaneous fistula), 4 had high-output proximal stomas and 3 had prolonged ileus/partial obstruction. One patient received home TPN for a spontaneous enterocutaneous fistula to an old surgical wound. TPN was given to 7 patients with the intention of performing delayed surgery. Five patients were given a trial of nonoperative management, with a plan to perform surgery for non-healing fistulas. The average duration of TPN prior to discharge was 19.6 days and for home TPN was 75 days (range 7–240). Two (13%) patients failed home TPN (1 with uncontrolled sepsis; 1 with dehydration) and were readmitted to hospital. Home TPN was stopped in 1 patient whose enterocutaneous fistula failed to heal with nonoperative treatment. Home TPN was successful in 12 (80%) patients, 8 (53%) who underwent planned definitive surgery and in 4 (27%) patients who settled without requiring surgery. No patient developed deterioration in any of the nutritional indices (weight, hemoglobin, transferrin, albumin, lymphocyte count) used to monitor therapy. Complications of home TPN were line sepsis and pulmonary aspergillosis in 1 patient. All patients preferred home TPN to further hospitalization and reported good or excellent quality of life at home. Home TPN is a safe alternative to prolonged hospitalization or early surgery in patients with complicated IBD.
6. IMPROVED OUTCOME AFTER COMBINED STOMA REVISION AND ABDOMINOPLASTY
Despite preoperative siting and maturation of stomas, some patients may have poor stoma function because of redundant pannus, scars, creases and parastomal hernias. In these patients, a combined abdominoplasty and stoma revision may be helpful. The object of this paper is to report our preliminary results. Seven patients (mean age 46, female:male 6:1) undergoing this procedure are reported. Five patients had IBD and 2 had malignancies. Patients were contacted at 2 months–2 years follow-up to assess functional outcome and satisfaction with the procedure. Indications for surgery were difficulty maintaining an appliance (n = 7), stool leakage (n = 5) and skin irritation (n = 4). Multiple surgeries (n = 3), skin creases (n = 2), scarring (n = 1), large weight loss (n = 4) and hernias (n = 5) were contributing factors. At surgery 5 patients had hernias repaired (3 parastomal, 2 incisional), 3 had stomas resited and 3 underwent resections for Crohn’s disease. One patient developed a seroma postoperatively. At follow-up all patients were able to maintain an appliance for at least 4 days, and none experienced stool leakage. All reported a dramatic improvement in body image. Combined stoma revision and abdominoplasty can be performed safely and leads to improved functional results and outcome.
7. LAPAROSCOPIC VERSUS OPEN RESECTION FOR COLORECTAL ADENOCARCINOMA
Laparoscopic surgery has not gained widespread application in the treatment of colorectal adenocarcinoma. We conducted a retrospective cohort analysis of 618 patients undergoing elective resection for colorectal adenocarcinoma between July 1992 and December 2000 at a university-affiliated hospital. These included 487 open (mean age; 76.1 years old) and 114 laparoscopic (mean age; 69.9 years old) resections. Data from converted cases (n = 17) were included in the laparoscopic group using the intention-to-treat principle.
Results:
Operative time, lymph-node yield and postoperative mortality were similar between laparoscopic and open technique. Laparoscopic patients used less parenteral analgesic, regained bowel function and oral intake earlier, and had decreased hospitalization time postoperatively than open patients. There were fewer minor complications in the laparoscopic group (laparoscopic, 15.2%; open, 26.2%; p < 0.05) but no difference in major complications or perioperative mortality. There were no differences in the disease-free survival, overall survival or recurrence rate among the 2 groups after a median follow-up of 49 months in the laparoscopic group and 37 months in the open group.
Conclusions:
Laparoscopic resection for colorectal cancer can be performed safely and effectively in tertiary centres. Earlier discharge from hospital, quicker resumption of oral feeds and less postoperative pain are clear advantages. Results of prospective, randomized trials, currently underway, are needed before laparoscopic resection for colorectal cancer becomes the standard of practice.
| Characteristic | Laparoscopic n = 131 | Open n = 487 | p |
|---|---|---|---|
| Operative time, min | 143.824 (54.575) | 140.787 (88.304) | 0.1318 |
| Lymph nodes harvested | 6.484 (4.987) | 6.521 (4.945) | 0.9473 |
| Parenteral analgesic use | 3.031 (3.410) | 4.262 (14.266) | <0.0001 |
| Flatus, d | 2.968 (1.591) | 4.167 (2.033) | <0.0001 |
| Bowel movement | 3.615 (1.924) | 5.056 (2.467) | <0.0001 |
| Soft diet | 2.220 (1.873) | 4.157 (2.240) | <0.0001 |
| Length of stay | 8.838 (9.063) | 13.311 (13.443) | <0.0001 |
Presented as mean (SD)
8. APPROPRIATENESS OF RECTAL CANCER MANAGEMENT IN BRITISH COLUMBIA
We report outcomes for all rectal cancers in BC in 1996. We relate outcomes to use of adjuvant radiation and chemotherapy, types of surgical procedures and staging investigations.
There were 495 adenocarcinomas of the rectum. Disease-specific survival at 4 years was: in situ — 100% (33 cases), stage 1 — 92% (135 cases), stage 2 — 78% (109 cases), stage 3 — 72% (89 cases), stage 4 — 17% (84 cases). Local recurrence rates at 4 years were: in situ — 0%, stage 1 — 6%, stage 2 — 16%, stage 3 — 27%.
Adjuvant radiation was given in 63% of stage 2 and 3 tumours less than 15 cm (143 cases) from the anus; preop. 7%, postop. 56%. Adjuvant chemotherapy was given in 59% of stage 2 and 3 tumours.
Local excision was performed in 4.4% of cancers with in situ — 27%, T-stage 1 — 11%, T-stage 2 — 1%, T-stage 3 — 0%. Twenty-nine percent of tumours with distance 5 to 10 cm from the anus were resected by abdominoperineal resection. Use of total mesorectal excision could not be reliably determined.
Investigations performed within 3 months of diagnosis were: chest x-ray — 65%, barium enema or colonoscopy — 74%, CT scan — 21%, ultrasound — 42%, endorectal ultrasound — 3%.
We conclude that: (1) BC survival rates are comparable to other centres. However, local recurrence rates are higher than current standards. (2) Adjuvant radiation and chemotherapy are used suboptimally in BC. (3) Local excision is used appropriately for in situ, T1 and T2 cancers. Rate of abdominoperineal resection for tumours 5 to 10 cm from the anus is high in consideration of current techniques for TME and coloanal reconstruction. (4) Total mesorectal excision as a standard of care could not be determined. (5) Staging investigations are used suboptimally. Access to CT and endorectal ultrasound scans is resource limited.
9. SURGICAL MANAGEMENT OF RECTAL CANCER: INFORMATION FROM THE OPERATIVE REPORT AND DISCHARGE SUMMARY
Population-based studies of rectal cancer management are dependent on accurate information about the tumour and the surgical intervention. Cancer-specific outcomes are affected by the technical quality of resection, as well as by the appropriate delivery of adjuvant treatment, which requires knowledge of the tumour’s extent and exact location. We hypothesized that this information would be difficult to obtain retrospectively. This study evaluated information contained within the operative report and discharge summary to determine their usefulness for epidemiologic studies and for medical and radiation oncologists in decision-making about adjuvant therapy. As part of the Patterns of Rectal Cancer Care in Ontario project, a sample of operative reports and discharge summaries was collected for patients diagnosed with primary rectal cancer in Ontario in 1996 to 1997. A multidisciplinary panel determined surgical factors important for cancer-specific outcome assessment. The records of 520 patients were examined. It was possible to determine that 62% (322/520) had an intentionally curative rectal cancer resection, while the remainder did not. The surgeon provided at least limited background information on 76% (245/322) of patients. A metastatic search at laparotomy was documented in 89% (287/322) of cases; in 83% (267/322), liver inspection was specifically mentioned. The operative procedure was always stated; 32% (103/322) had an abdominoperineal resection. The tumour’s relation to the peritoneal reflection was documented in 69% (222/322) of reports, and the distance from the anal verge in 47% (151/322). A sharp mesorectal resection was described or implied in 15% (48/322). The operative report and discharge summary were useful to provide information about the intent and type of procedure and the metastatic status, but were less useful about precise tumour location and technical aspects of the resection. Improving documentation of the latter factors is important since these are major determinants of outcome.
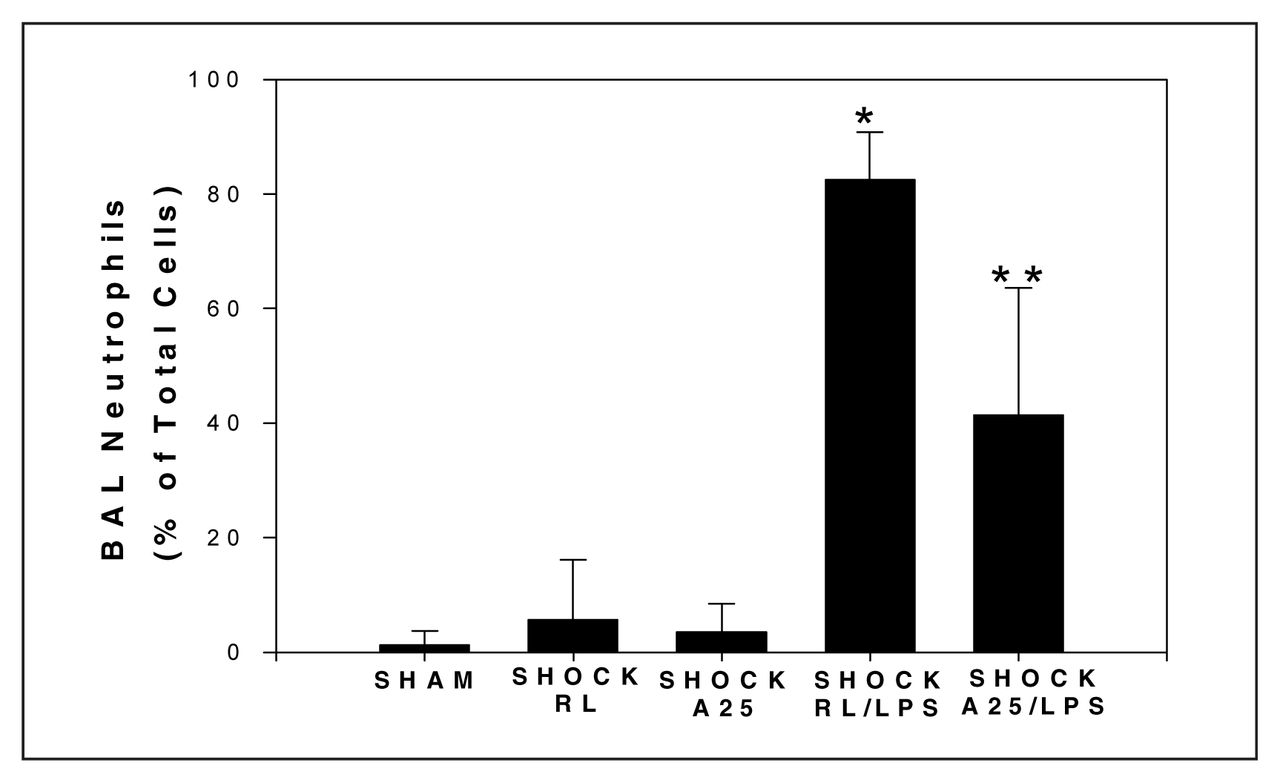
10. 25% ALBUMIN PREVENTS LUNG INJURY IN A RESUSCITATED SHOCK ANIMAL MODEL
We previously showed that antecedent shock/resuscitation in rodents enhanced LPS-induced lung injury and that the antioxidant N-acetyl-cysteine prevented this priming effect. We hypothesized that 25% albumin (A25), due to its antioxidant activity, might be both an effective resuscitation fluid as well as an immunomodulatory agent.
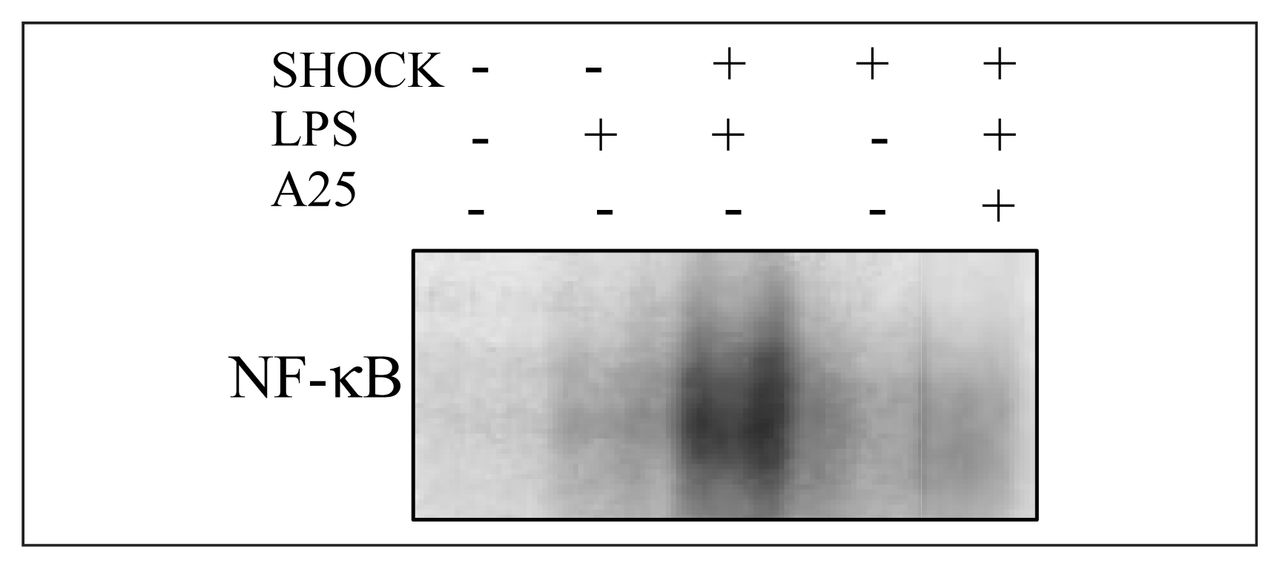
Sprague–Dawley rats were bled to a mean arterial pressure of 40 mm Hg, and maintained in a shock phase for 1 hour, then resuscitated with either shed blood and an equal volume of Ringer’s lactate (RL) or with shed blood plus one-fourth of their shed blood volume of A25. MAP was monitored continuously. One hour after resuscitation, LPS (30 μg/kg) or saline (SAL) was given intratracheally. Lung permeability index (LPI) was determined by intravenously injecting 1 μCi of [125I]fibrinogen, just prior to LPS or SAL, and analyzing counts in blood and bronchoalveolar lavage fluid (BALF) at t = 6 h. BAL was also performed at t = 4 h for determination of lung total cell counts (TCC) and differential cell counts. Lungs were harvested at 4 hours after LPS or SAL treatment and NF-κB nuclear translocation was detected by an electrophoretic mobility shift assay (EMSA) on whole lung tissue.
Animal survival in both groups exceeded 90%. Animals resuscitated with RL had a significant rise in LPI compared with sham animals (n = 4 per group,*p < 0.05). However, the use of A25 prevented this increase (n = 4,**p < 0.05, Fig. 1). Resuscitation with A25 caused a significant decrease in the percent neutrophils in BALF compared with RL (n ≥ 4 per group, *p < 0.01, Fig. 2). LPS-induced NF-κB nuclear translocation was augmented by antecedent shock, however A25 resuscitation reversed this process (Fig. 3).
Resuscitation with albumin decreases the LPS-induced increase in lung permeability, pulmonary neutrophil sequestration and NF-κB activation. These findings suggest a novel immunomodulatory role for albumin resuscitation.

11. STRICT ADHERENCE TO THE DAMAGE CONTROL SURGERY CRITERIA SIGNIFICANTLY INCREASES THE LIKELIHOOD OF SURVIVAL
The purpose of this study was to identify, 1) trauma patients who met the criteria for damage control surgery (DCS), 2) the subcategory that, in fact, underwent DCS, and 3) any survival advantages by adhering to these criteria. A retrospective chart review was performed on trauma patients who were admitted to the Montreal General Hospital from 1994 to 1999 and met the following selection criteria; 1) had documented intra-abdominal injury, 2) were operated on by the trauma service in the first 24 hours of admission, 3) were admitted to the surgical intensive care unit immediately postoperatively and 4) were reoperated or pronounced dead during the first 72 hours of admission. Comparisons were made based on the 72-hour survivals. One hundred and eighty-six patients were identified, of whom 34 met the selection criteria. The 72 hours mortality rate was 41%. The nonsurvivors were significantly more acidotic, hypothermic and coagulopathic than survivors. Overall, 27 patients met the DCS criteria, and DCS was adequately performed in 59% of them. Our selection criteria resulted in close to 80% accuracy in identifying patients to whom DCS could have been offered. Patients who met the DCS criteria had an associated 72-hour mortality rate of 50%. pH less than 7 and PTT greater than 120 in a patient whose temperature is less than 32.5 °C was associated with a mortality rate of 100%. Therefore, any form of non-essential surgical procedure that would delay the nonoperative resuscitation of a patient whose pH <7.2, T <35 °C and has PT >55, the DCS criteria, appears to be associated with increase in mortality rate from 50% to virtually 100%.
12. OUTPATIENT HERNIA REPAIR IN A MINOR PROCEDURE ROOM UNDER LOCAL ANESTHESIA
Methods:
Retrospectively, the charts of patients with groin hernias managed in this fashion from January 1994 to September 2000 were reviewed.
Results:
During this period, 600 groin hernias were repaired in this fashion including 67 recurrent hernias. Age range was 17 to 92 years; 552 were males (92%) and 48 females (8%). Three hundred and thirty right side (55%), 265 left side (44%), and bilateral (1%) groin hernias were repaired. There have been 13 (2%) recurrences, 3 (0.5%) minor infections and a single case of urinary retention. Patient satisfaction with the procedure is excellent.
Conclusion:
We conclude that repair of groin hernia can be carried out on an outpatient basis under local anesthesia in a minor procedure room with acceptable results without the need for additional nursing and recovery room facilities.
13. ESOPHAGEAL CANCER: A LAPAROSCOPIC APPROACH
The purpose of this report is to describe the surgical management of patients with esophageal carcinoma using minimally invasive techniques and report on early outcomes of patients following laparoscopic esophagectomy.
Data was obtained from a prospectively collected computer database of 32 consecutive patients referred for surgery with a diagnosis of esophageal carcinoma. Staging laparoscopy was performed in all patients. If curable disease was found, a laparoscopic esophagectomy was attempted. Follow-up data was obtained from the patient’s office chart and, if incomplete, from patients, their family or the family physician.
Thirteen patients (40.6%) had incurable disease based on staging laparoscopy (6 had tumour invading local structures, 6 had bulky tumour involvement of celiac nodes, and 1 had diffuse peritoneal carcinomatosis). Laparoscopic esophagectomy was attempted in 19 patients (12 males and 7 females). Median operative time was 380 minutes (range of 230–445) and median operative blood loss was 400 cc (range of 100–1000). Two cases were converted. Median hospital stay was 12 days (range of 8–39) and median ICU stay was 2 days (range of 1–39). Four patients (21.1%) suffered major postoperative complications and 12 patients (63.1%) suffered minor complications that did not affect length of stay. There was 1 in-hospital death (5.3%). Delayed complications occurred in 5 patients (26.3%). Proximal and distal resection margins were tumour free in all cases. Average number of lymph nodes excised was 10 (range of 2–30). There was 1 stage 0, 3 stage 1, 4 stage 2A, 5 stage 2B, and 6 stage 3 tumours. Overall survival was 68.4% with a median follow-up of 18 months.
Staging laparoscopy can spare some patients with esophageal cancer unnecessary surgery. Laparoscopic esophagectomy is safe, feasible and can be done with acceptable morbidity and mortality.
14. IN ADVANCED CANCER IS GASTRECTOMY PALLIATIVE?
While much is published on the extent of surgery required to achieve cure in gastric cancer, the reality is that the majority of patients present with advanced incurable disease. Traditional teaching is that gastrectomy is the best form of palliation. Given the propensity for submucosal spread in advanced disease, removal of the primary may not be possible with negative margins.
This study compares survival curves in non- and gastrectomized gastric adenocarcinoma.
Prospectively collected Provincial Registry data from Northern Alberta between 1991 and 1995 were examined. There were 411 patients (70 ± 13 yr) (60%) male, stage I 11%, II 8%, III 25%, IV 43%, unstageable 12%. To date 89% have died. Surgery (major resection 54%, minor [bypass] 14%) was carried out on 68% (278 of 411). There were positive margins in 39 of 222 major resections (18%).
The overall 5-year survival was 13% (median 7 mo). For those undergoing major resection with negative margins 5-year survival was 28% (median 19 mo), but with positive margins was 5% (median 9 mo) p < 0.00005. Survival for bypass (median 3 mo) and no surgery (median 2 mo) was not different (p < 0.66). In stage III disease the survival difference for negative margins (median 15 mo) and positive margins (median 8 mo) was significant (p = 0.0016) but not for stage IV disease (p = 0.58) with medians of 6 and 9 months respectively.
We conclude that palliative gastrectomy even with positive margins achieves longer survival than bypass or laparotomy or no surgery. This supports the long held dogma that palliative gastrectomy should be attempted where possible except when stage IV disease is present.
15. SYSTEMATIC OUTCOMES EVALUATION IN ELECTIVE SURGERY
There is currently wide variation in the rates of elective surgery and a lack of systematic measurement of outcomes, leading to inevitable questions about the appropriateness of some procedures. This study was designed to assess the feasibility and perceived value of routinely assessing surgical indications and measuring patient self-reported health-related quality-of-life (HRQOL) outcomes.
The study included 138 surgeons and 6274 elective surgical procedures in the entire Vancouver/Richmond Health Region. Information on the indications for surgery provided by the surgeon was matched against the InterQual™ guidelines and all patients were sent both generic and disease-specific HRQOL questionnaires before and at appropriate intervals after surgery.
Sufficient data to evaluate the surgical indications were obtained from surgeons on 60% of patients, and of these the proportion matching the guidelines ranged from 48% to 100% for individual surgeons. HRQOL surveys were completed by 58% of patients and the results showed marked and significant improvement overall, but with considerable variation by procedure and by individual. As expected, there was a highly significant relationship between the preoperative level of symptoms/disability and the extent of improvement after surgery. Many of the patients reporting minimal symptoms and disability preoperatively derived little benefit from the procedure, and some reported deterioration. Opinion among the participating surgeons was mixed in terms of the usefulness of this patient self-reported information on outcomes.
Improved HRQOL is ultimately the most important objective of most elective surgical procedures, but surgeons in general have as yet little understanding of or interest in this rapidly expanding field of outcomes research. This study demonstrates that HRQOL outcomes information can be gathered inexpensively and suggests that it could be valuable to surgeons for routine patient follow-up and in the clinical decision-making process to help identify patients less likely to benefit from surgery.
16. LES EFFECTIFS EN CHIRURGIE GÉNÉRALE AU CANADA ET AU QUÉBEC DE 2001 À 2021. CANADA AND QUEBEC, GENERAL SURGERY MANPOWER 2001–2021
Nous voulons démontrer que la chirurgie générale vit actuellement une pénurie d’effectif qui ne fera qu’accroître, au cours des deux prochaines décennies, tant au Canada, qu’au Québec. Des statistiques et des tableaux résultant de recherche sérieuses, incontestables, illustrent sans équivoque la mesure de cette pénurie anticipée. Si, aucun correctif n’est appliqué dans les prochaines années, le ratio chirurgien général/population ira en diminuant, pour atteindre des proportions menaçante, empêchant de dispenser des soins chirurgicaux de base de manière adéquate et uniforme dans un pays développé. Un ensemble multi-factoriel est responsable de cette situation appréhendée, vieillissement des effectifs, féminisation, retraites, mode de vie, manque d’attrait de la chirurgie générale auprès des étudiants en médecine, résidence difficile, mauvaise rémunération de la spécialité.
[We wish to show that general surgery is facing a serious manpower shortage that will grow over the next 2 decades across Canada and Quebec. Without contest, grafts and stats issued from serious research will illustrate the magnitude of that anticipated deficit. If no correction is applied in the next years, the general surgeon/population ratio will drop to a threatening level. Basic surgical care will no longer be available everywhere evenly in a country of the developed world, our country, Canada. Many factors are responsible for this apprehended situation, aging of the surgeons, feminizations, retirement, way of life, lack of attraction toward medical students, difficult residency, bad income of the specialty.]
17. L’EXPLORATION CERVICALE UNILATÉRALE DANS LES ADÉNOMES PARATHYROÏDIENS
L’arrivé de la scintigraphie au sestamibi-Tc99m a considérablement amélioré la localisation préopératoire des glandes parathyroïdes dans l’hyperparathyroïdie primaire. Le but de cette étude est de démontrer son utilité dans l’exploration cervicale unilatérale, ainsi que d’évaluer sa sensibilité dans notre milieu. Revue de 123 cas dans un centre tertiaire, de 1995 à 2000. Des 114 cas d’hyperparathyroïdie primaire identifiés nous avons 93.9% d’adénomes dont 4.6 % étaient doubles, 5.3 % d’hyperplasie et 0.9 % de cancer. Le taux de succès est de 97.4 % (3 échecs). La différence des temps d’anesthésie était statistiquement significative (69 ± 29 minutes p < 0.002). 79.5 % des patients qui ont eu une scintigraphie préalablement (112), sans pathologie thyroïdienne associée, ont bénéficié d’une exploration unilatérale. La sensibilité dans cette série était de 92.6 % avec une valeur positive prédictive de 96.2 %. La scintigraphie au sestamibi-Tc99m est utile dans localisation initiale des adénomes parathyroïdiens en permettant une exploration unilatérale dans presque 80 % des cas, ce qui diminue significativement le temps d’anesthésie. La procédure chirurgicale étant plus limitée, il pourrait y avoir un effet aussi sur le nombre de complications.
[Tc99m-sestamibi scanning has markedly improved preoperative parathyroid gland localization. The aim of this study was to assess its usefulness in unilateral cervical exploration for cases of primary hyperparathyroidism, as well as to evaluate its sensitivity in our centre. A review of 123 cases in a tertiary centre, from 1995 to 2000. From 114 identified cases of primary hyperparathyroidism, there was 93.9% adenomas, of which 4.6% were double, 5.3% hyperplasia and 0.9% cancer. Success rate was 97.4% (3 failures). Statistical difference was achieved for the difference in time of anesthesia between unilateral and bilateral cervical exploration (69 ± 29 min, p < 0.0002). 79.5% of patients who had preoperative scanning (112), and no associated thyroid pathology, had unilateral cervical exploration. In this series, the sensitivity was 92.6% with a positive predictive value of 96.2%. Tc99m-sestamibi scanning is useful for initial localization of parathyroid adenomas, leading to the oportunity of unilateral exploration in almost 80% of cases which reduces significantly anesthesia time. The procedure being more limited, there could be an impact on the number of complication as well.]
18. FAMILIAL MEDULLARY THYROID CARCINOMA IN A LARGE KINDRED WITH V804M MUTATION — CLINICAL AND PATHOLOGICAL CORRELATION WITH RECOMMENDATIONS FOR TIMING OF THYROIDECTOMY
In order to avoid the development of medullary carcinoma, the endocrine surgery literature recommends prophylactic thyroidectomy at the age of 6 or 7 for carriers of mutations in the RET oncogene, in families with multiple endocrine neoplasia (MEN) type 2A, 2B or familial medullary thyroid carcinoma (FMTC). We present the largest RET oncogene mutation-positive kindred known to date. This kindred is composed of over 1150 members followed thus far, of whom 126 have undergone genetic testing. Of these, 42 have been found to be carriers of the RET V804M mutation. To date, 15 have undergone total thyroidectomies at our site. Although 9 were found to have medullary thyroid cancer, only 2 were found to have nodal metastases at the time of surgery. Some family members with the V804M mutation have not undergone thyroidectomy due to advanced age, and have been followed clinically with no evidence of FMTC.
All of our V804M carriers had C-cell hyperplasia noted by our pathologists. Only patients with medullary carcinoma were found to have elevated calcitonin levels preoperatively. Among both who had nodal metastases, the calcitonin levels were elevated for long-standing periods preoperatively. None of the patients with FMTC have died of metastatic disease, and 1 of the patients with nodal metastases has been asymptomatic for over 16 years. The average age of the patients with FMTC at the time of surgery was 53.3 (range 33–65).
Since the advent of genetic screening, an increasing number of patients with RET oncogene mutations are presenting for prophylactic thyroidectomy, including the children of carriers. Mutations that cause FMTC have variable penetrance and expressivity, as can be demonstrated in this family, where there are no cases younger than 33. We recommend that the age for prophylactic thyroidectomy be mutation-specific, retaining the age 5 to 6 for mutations causing MEN 2A, age 1 to 3 for mutations causing MEN 2B and adulthood (over age 19) for mutations causing FMTC.
19. PROGNOSTIC FACTORS IN RESECTED PANCREATIC ADENOCARCINOMA: ANALYSIS OF 5-YEAR SURVIVORS
Discrepancies exist between actuarial and actual 5-year survival rates for pancreatic adenocarcinoma. Our objective was to determine the actual 5-year survival rate of patients with pancreatic adenocarcinoma who underwent a resection with curative intent in 5 hospitals within the University of Toronto. We then sought to determine clinical and histopathologic features of 5-year survivors to determine factors associated with a more favourable prognosis.
A retrospective chart review was performed using surgeon and hospital databases to identify patients who had a surgical resection (Whipple, total or distal pancreatectomy) for pancreatic adenocarcinoma between Jan. 1, 1988, and Dec. 31, 1995.
Using the above search strategy, 112 patients from 7 surgical practices were identified who had a resection and a pathologic diagnosis of pancreatic adenocarcinoma. Mean survival for all patients was 30.3 months.
There were 17 5-year survivors (15.2%) including 4 patients (3.6%) who survived more than 10 years. The survivors included 12 patients with a Whipple resection, 4 with a distal pancreatectomy, and 1 with a total pancreatectomy. Four of the 5-year survivors died of recurrent pancreatic cancer at 60, 62, 79 and 106 months and 3 patients died of other causes. Ten patients are still alive at a mean of 110.8 months after surgery.
Five-year survivors had smaller tumours (mean 2.24 v. 3.20), a lower rate of duodenal (18% v. 52%) and commonbile-duct invasion (18% v. 31%), a higher proportion of well-differentiated tumours (58.3% v. 13.1%) and a lower proportion of node-positive disease (25% v. 51.6%). The 5-year survival rate by tumour size was: T1 tumours 25%, T2 13.5%, and T3 6%.
Univariate proportions were evaluated by Fisher’s exact test. Tumour size, nodal involvement, tumour grade, duodenal invasion and tumour location were all significant (all p < 0.05). Only nodal status (p < 0.001) and tumour grade (p < 0.02) were independently associated with survival differences in a multivariate Cox proportional hazards model.
We conclude that pancreatic adenocarcinoma is occasionally curable if identified in its early stages. These and other similar data should provide further stimulus for the development and evaluation of novel screening strategies, especially for those subjects with inherited predisposition to the disease.
20. GEMCITABINE IN THE TREATMENT OF ADVANCED PANCREATIC CANCER — RELEVANCE IN CLINICAL PRACTICE
This study was done to report our experience with the administration of systemic gemcitabine in the treatment of advanced pancreatic cancer.
From our prospective data bank, we review all the cases of patients with advanced pancreatic cancer treated with gemcitabine between July 1997 and December 1999 (n = 17). Tumours were non-resectable for anatomical reason (T4) in 10 patients and because of metastasis in 7. Eleven patients had a palliative surgery, 3 had a diagnostic laparotomy and 3 had an endoscopic stent. Actuarial survival, disease-free survival, symptom-free survival and time-to-progression were calculated (Kaplan–Meier). Toxicity of treatment was classified according to AJCC criteria.
We administered 440 injections of gemcitabine to 17 patients. Mean survival was 18.5 months. Symptom-free survival was 16.4 months. Time to progression was 15.7 months. Two patients had a complete response and are disease-free at 12 and 30 months. Once doses were adjusted for toxicity, mean dosage of gemcitabine administered was 800 mg/m2 weekly for 3 weeks per month. Dose reductions were planned for any grade 2 toxicity but treatment interruption was never required. Sixty-four injections were delayed for 1 week. Four patients required odansetron to control nausea on a regular basis. Tumour measurements were done every 3 months with helicoidal CT-SCAN and treatment was stopped when progression was noted.
Gemcitabine has a major role in the treatment of advanced pancreatic cancer. It is a well-tolerated treatment and should be started as soon as possible for better response rate.
21. CLINICAL AND PATHOLOGIC CHARACTERISTICS OF A COHORT OF PATIENTS WITH COLITIS-ASSOCIATED NEOPLASIA
Chronic inflammatory bowel disease is associated with an increased risk of colorectal neoplasia. Despite the use of colonoscopic screening, patients continue to present with colorectal malignancies. The purpose of this study was to review the clinical and pathologic features of a cohort of patients undergoing resection for colitis-associated neoplasia (CAN) at our institution.
Patients who had resections between 1989 and 2000 were identified using prospectively obtained information on our IBD database, as well as a review of the hospital’s pathology department database, searching for the combined diagnoses of IBD and colon or rectal cancer. Clinical and pathologic data were obtained from information contained in the database and by review of the patients’ hospital and office charts.
Forty-two patients with 54 colitis-associated neoplasms treated at our institution were identified. There were 37 cancers, 12 dysplasia-associated lesions or masses (DALM), and 5 high-grade dysplasias. Of the cancers, 12 were T1 lesions, 6 were T2, 14 were T3 and 3 were T4. Seven patients had stage 3 disease, while 5 had stage 4. Thirty-nine percent of the neoplasms were right-sided, 28% were left-sided and 33% were rectal. Ten cancers (27%) had mucinous differentiation. The mean age of onset of IBD was 32.5 (±18.1) years, and the mean time from diagnosis of IBD to diagnosis of neoplasia was 16.9 (±10.6) years. However, considering the recommendation of beginning screening only after 8 years of disease, 10 (24%) of our patients presented with neoplasia within 8 years of their diagnosis of IBD. Additionally, 14 (33%) patients had negative endoscopy and the neoplasm was found incidentally in their resected specimen. Eight (19%) had a family history of IBD, while 11 (26%) had a family history of colorectal cancer.
Colitis-associated neoplasia continues to present a challenging problem to the practising clinician. These patients often present with neoplasia at an earlier age, and often seem to have an aggressive course, with relatively frequent unfavourable histology. Despite surveillance, one-third of the patients in this series had their neoplasm missed and only diagnosed on pathologic examination of their resected specimen. A family history of IBD and/or colorectal cancer was frequently present, suggesting possible genetic factors leading to neoplastic development. Further research in this group of patients is warranted.
22. INHIBITION OF NF-κB ACTIVITY WITH NACETYLCYSTEINE NORMALIZES INTESTINAL PERMEABILITY IN SEPSIS
Studies have shown that increased activity of nuclear factor kappa B (NF-κB) is at least partially responsible for the breakdown of gut barrier function seen in sepsis and multiorgan system failure. Work in other areas has demonstrated that NF-κB activity is inhibited by N-acetylcysteine (NAC). We hypothesized that administration of NAC would normalize intestinal permeability by inhibiting NF-κB activity in a rat model of sepsis induced by intraperitoneal (ip) administration of bacterial lipopolysaccharide (LPS).
An experimental study was performed on 20 male Wistar rats, divided into 4 groups. Rats received an ip injection of: (a) saline (controls), (b) NAC alone (300 mg/kg), (c) LPS alone (7 mg/kg), or (d) both LPS and NAC. Intestinal permeability before and after treatment was determined using the inert sugar method, whereby the concentrations of orally administered sugars are measured in the urine. The rats were then sacrificed and mucosal scrapings taken from the small intestine for Western blot analysis of phosphorylated IκB-α levels, an indirect measure of NF-κB activity.
Mean intestinal permeability increased by 130% above baseline in rats treated with LPS alone (p < 0.05). When NAC was given along with LPS, the increase in mean permeability was reduced to 46% (p > 0.05). There was no significant change in permeability in rats treated with ip saline or NAC alone. Western blot analysis of small-bowel mucosa showed a 30% reduction in phosphorylated IκB-α levels in rats given LPS and NAC when compared to rats given LPS alone, indicating a decrease in NF-κB activity.
These preliminary results demonstrate that administration of NAC inhibits NF-κB activity and normalizes intestinal permeability in a rat model of sepsis. Thus, N-acetylcysteine may be a useful therapeutic agent in preventing the progression of sepsis to multiorgan system failure and death.
23. MINIMIZING BLOOD LOSS AND TRANSFUSION REQUIREMENTS IN HEPATIC RESECTION
Significant blood loss and the requirement for blood transfusions remain major considerations for hepatic surgeons. We analyzed the impact of a systematic protocol aimed at reducing intraoperative blood loss and homologous blood (HB) transfusion associated with hepatic resection.
Prospective clinical data was collected from 151 elective liver resections performed during the period of 1980 to 1999. Strategies implemented in 1991 included preoperative autologous blood donation, low central venous pressure anesthesia, aprotinin administration, ultrasonic dissection, hepatic vascular inflow occlusion cell saver. Blood loss and transfusion requirements before and after the implementation of these strategies was studied.
Central venous pressure less than 6 mm Hg during transection and intravenous aprotonin administration were the most significant factors in minimizing intraoperative blood loss. There was no difference in the patient demographics, indications for operation or the scope of resections in the 2 time periods evaluated. Blood-saving strategies resulted in decreased estimated blood loss (4500 mL v. 1000 mL p < 0.001). In addition, the number of patients requiring transfusion decreased (91.8% v. 25.5% respectively, p < 0.001) and the mean number of units of HB transfusion was lower (13.7 v. 2.3, p < 0.001). Morbidity and mortality were also decreased (57.1% v. 25.5%, p < 0.001 and 10.2% and 4.9% p < 0.001 respectively) and no complications directly referable to low CVP anesthesia were identified.
Systematic implementation of strategies designed to control blood loss are effective and may reduce morbidity and mortality associated with hepatic resections.
24. CHOLANGIOGRAPHY IN BILIARY PANCREATITIS
In order to define the role of cholangiography in preventing recurrent pancreatitis the charts of 108 patients admitted with biliary pancreatitis were reviewed. Of these 65 patients (60%) underwent cholangiography. In 47 patients subjected to preoperative ERCP, common duct calculi were found in 16 (34%). Intraoperative cholangiography (IOC) done in 12 of 74 patients who had laparoscopic cholecystectomy was technically adequate in 8 (66%). IOC done in 5 of 15 patients who had open cholecystectomy was adequate in 4 (80%). No stones were found with IOC.
In 8 patients (7.4%) readmitted with pancreatitis, 6 had not undergone cholangiography. One patient died and another developed pancreatic sepsis.
We conclude that adequate cholangiography to permit clearance of the biliary tree is necessary to prevent recurrence of biliary pancreatitis.
25. DECOMPRESSION OF MALIGNANT BILIARY OBSTRUCTION: A PROSPECTIVE TRIAL EXAMINING QUALITY OF LIFE
We tracked changes in the quality of life of patients with malignant biliary obstruction following decompression with a plastic stent.
Data were prospectively recorded at baseline, 7 days and 1 month including: body mass index, weight loss, duration of symptoms, total bilirubin (TB), site of biliary obstruction, pruritus, and the SF-36 Health Survey questionnaire. Statistical analysis was performed using the Student’s t-test, the Kruskal–Wallis one-way analysis of variance, and the Pearson chi-square test where appropriate.
Fifty patients (20 men, 30 female), of mean age 72.6 years (SD: 10.6), and mean body mass index of 23.4 (SD: 4.3), were enrolled. At baseline, 70% of patients had pruritus with average TB of 283 mmol/L (SD: 136). Duration of symptoms ranged from 2 to 120 days (SD: 25). Men reported worse general health (p = 0.029) before decompression. Clinical variables most affecting baseline function were weight loss and the TB value. Baseline TB correlated with patients’ baseline assessment of physical role (p = 0.011), vitality (p = 0.042), and social function (p = 0.005). Weight loss also was significantly associated with patients’ baseline QOL in several domains.
Following biliary drainage, an improvement in TB of at least 33% was documented in 84% of patients. This “successful” drainage was associated with improvements in social function (p = 0.030) and mental health (p = 0.030) at 1 month.
A baseline TB above 250 mmol/L predicted a lack of improvement in social function after 1 month (p = 0.03).
Clinical parameters in patients with malignant biliary obstruction can be correlated with determinants of QOL, and subgroups can be determined which exhibit improvement after “successful” biliary decompression.
26. PROGRESSION OF PERIAMPULLARY ADENOMAS IN FAMILIAL ADENOMATOUS POLYPOSIS
A common cause of cancer death following colectomy in FAP is upper gastrointestinal malignancy. Although endoscopic surveillance is recommended, there is no consensus on the frequency of endoscopies or management. The specific aim of this study was to understand the natural history of duodenal polyps in FAP and to devise an evidence-based protocol for surveillance of upper GI polyps.
One hundred and fifteen FAP patients were followed prospectively using periodic upper GI endoscopies based on a protocol developed in 1990. The majority of these endoscopies were performed by a single surgeon. Polyps were classified according to their size and histologic characteristics into stages 1 to 5, as previously described. Statistical analysis included one-way ANOVA for the age comparisons between stage groups and Kaplan–Meier analysis for the lifetime risks of having a particular stage.
Fifty-four males (47%) and 61 females (53%) were studied. The average age at colectomy was 29.9 years (range 9–62) and at first side-viewing upper endoscopy was 39.1 years (range 16–69). The stages at first endoscopy were higher in older patients. There was a significant difference between the mean age at first endoscopy for stage 1 (37.3 years) and stage 4 (54.0 years) patients (p = 0.02), as well as for stage 2 (37.3) and stage 4 patients (p = 0.03). Of the 115 patients, 87 (76%) had 2 or more endoscopies and were followed for an average of 6.6 years (range 1–15). Of the patients with at least 2 endoscopies, 33 (38%) had a change in stage, in an average time of 3.94 years (range 0–13). The average age at which a change occurred was 40.9 years (range 22–74). There were no significant differences when comparing average time to first stage change across groups categorized by stage at first endoscopy. The stage at first endoscopy did not correlate with the degree of dysplasia in the periampullary polyps. The progression of the periampullary adenomas in patients who had 2 or more upper GI endoscopies was very slow. Close to 90% of patients had periampullary polyps by the age of 75. The risk of having a stage 3 or higher polyp increased exponentially after the age of 40.
The stage of duodenal polyposis increases with age in FAP. The average time for change in stage was 3.9 years. The average age for this change in stage was 41. These values do not seem to be influenced by the initial stage at first endoscopy. The degree of dysplasia did not correlate with initial stage. The risk of having a higher staged polyp is exponentially increased in FAP patients after the age of 40. Progression of periampullary adenomas in FAP appears to be slow. We therefore propose a revised endoscopic surveillance protocol for FAP.
27. VALUE OF FOLLOW-UP IN PATIENTS WITH HIGH-RISK MELANOMAS
Guidelines for the follow-up of patients with diagnosed thick melanomas are not well established. Since melanomas greater than 4 mm have a high incidence of local and distant recurrence, most centres recommend following these patients every 3 months for the first 3 years based on little data. The purpose of this study was to determine the most common method of detecting recurrences and whether the method of detection or intensity of follow-up impacted on survival. A retrospective chart review yielded 80 patients with thick melanomas (Clark level V or Breslow ≥4 mm) diagnosed between November 1979 and April 2000 who were followed for a median of 701 days (range: 76–7112).
The median age at diagnosis was 59.2 years (range: 19.3–88.8); 64 patients had ulcerated lesions and Breslow ranged from 3.5 to 35 mm. Recurrence occurred in 53 patients with a median disease-free survival of 531 days (±99.3). The 24-month overall survival was 62.7%, with a median survival time of 1052 days (±147.2). Of the 53 recurrences, 47% (25) were detected by patient self-examination and 49% (26) by the physician (2 unknown). Method of recurrence detection did not impact on time to recurrence (p = 0.8816) or time to death (p = 0.8966). Survival of patients more intensely followed (30) did not differ significantly (p = 0.5537) from the less intensely followed patients (48). Two patients were not seen in the first 12 months.
These results indicate that intensity of follow-up or method of recurrence detection in patients with high-risk melanomas does not impact on time to recurrence or survival. We conclude that routine follow-up guidelines should be re-examined to provide the most efficient care to melanoma patients.
28. MIS SURGICAL PRACTICE IN ONTARIO: A SURVEY OF GENERAL SURGEONS
The purpose of this study was to assess the state of MIS within the general surgery community in Ontario.
A pre-tested questionnaire was mailed to general surgeons in Ontario. The survey addressed the surgeon’s practice demographics, his/her performance of both basic and advanced MIS procedures, the factors influencing this practice, and the means of obtaining MIS training.
307/390 (78.7%) of general surgeons responded to the survey. Thirty-six respondents were retired and thus excluded from the analysis. The study group averaged 49 years old and consisted of 245/269 (91%) men. 115/269 (43%) had subspecialty training. The average surgeon’s OR time was 1.5 d/wk and wait list was 4 weeks for elective procedures. 255/270 (94%) performed basic laparoscopic procedures, though only 162/267 (61%) performed appendectomy. 133/270 (49%) performed at least 1 advanced laparoscopic procedure in their practice, though 30/133 (23%) only performed inguinal hernia repair. Using a Likert scale, the most important factors influencing the incorporation of advanced laparoscopic procedures into one’s practice were a lack of training opportunities (median = 3.5), OR time (median = 4), OR financial resources (median = 4). 160/250 (64%) of surgeons felt that the present medical environment did not allow them to meet standard of care requirements. General surgeons felt that it was the responsibility of academic surgical departments (212/266 [80%]), CAGS (176/260 [68%]), and the OAGS (140/262 [53%]) to provide CME courses for MIS training.
There are significant concerns raised regarding the ability of practising surgeons to incorporate advanced MIS procedures into their respective practices.
29. HEREDITARY NON-POLYPOSIS COLORECTAL CANCER — REPORT OF 25 YEARS’ EXPERIENCE IN A RURAL CANADIAN SETTING
Hereditary non-polyposis colorectal cancer (HNPCC) is an autosomal dominant condition predisposing to colorectal carcinoma (CRC), endometrial and other cancers in the absence of premonitory stigmata.
We report our experience — beginning in the mid 1970s — with a large HNPCC kindred whose pedigree now spans some 10 generations and for whom, because of geographic isolation, follow-up is virtually complete. Detailed records permit an unrivalled opportunity to document the natural history of this condition and the salutary influence and cost-effectiveness of an intensive surveillance program (2-yearly physical examination, colonoscopy, urine cytology, pelvic examination, pelvic ultrasound, endometrial aspiration biopsy) coupled with genetic counselling and directed by genetic testing.
HNPCC in this kindred has been traced to a deletion in the hMSH2 gene. Thirty-four (34) CRCs have developed in 24 individuals (18 males and 6 females). Seventeen (17) individuals had only 1 CRC, 4 had 2 CRCs and 3 had 3 CRCs. Average age to first CRC was 43.5 years. The following extracolonic malignancies were encountered : transitional cell carcinoma ureter/bladder — 7 lesions in 5 patients; endometrium — 6; stomach — 1; kidney — 1; cutaneous stigmata of Muir-Torre — 4 patients. No individual in this kindred who has complied with the recommended screening protocol has developed an incurable malignancy.
Intensive case documentation and research into pedigrees in the last 5 years has uncovered another 30 families in this region who fulfil the Amsterdam criteria. Several other “worrying” pedigrees have also been discovered. As yet a genetic marker has not been determined for these groups and some 300 individuals are currently participating in a surveillance protocol.
This ongoing work exemplifies the benefits that may derive from collaboration between a rural community hospital and a university teaching centre.
30. LAPAROSCOPIC VERSUS OPEN DONOR NEPHRECTOMY — ONE INSTITUTION’S INITIAL EXPERIENCE
We initiated a laparoscopic donor nephrectomy (LDN) program at our institution in July 2000, with the objective of reducing donor morbidity, while achieving the equivalent graft outcomes as those of open donor nephrectomy (ODN).
Data from 17 laparoscopic donors and recipients was compared with a matched retrospective cohort of 14 contemporaneous open donors and recipients.
Baseline characteristics were similar for all groups. The LDN group had longer operative times (227 ± 67 min v. 138 ± 21 min, p < 0.001), less blood loss (78 ± 40 mL v. 131 ± 84 mL, p = 0.05) and longer warm ischemic times (180 ± 63 s v. 32 ± 7 s, p < 0.001). Serial serum creatinines at 1 day up to 3 months postoperatively were not statistically different between the 2 groups. Narcotic use was similar in both groups (99.4 mg morphine v. 143.1 mg, p = 0.129). There was an earlier return to normal diet (2.5 ± 0.59 v. 3.0 ± 0.67 d, p = 0.015) and a shorter hospital stay (3.0 ± 0.70 v. 4.0 ± 1.04 d, p < 0.001) in the LDN group. There was no difference in serial recipient creatinines up to 3 months (p = 0.673 ) or in donor vessel length (p = 0.24). One LDN patient required conversion to ODN; her recipient had delayed graft function for 1 week, not requiring dialysis, that resolved completely. There was no statistically significant difference in intraoperative and postoperative complications between the LDN and ODN groups. There were no ureteral or vascular graft complications.
LDN patients return to normal diet and are discharged sooner, without adversely affecting recipient graft function.
31. SURGICAL OUTCOME IN GASTROESOPHAGEAL REFLUX DISEASE PATIENTS WITH INADEQUATE RESPONSE TO PROTON PUMP INHIBITORS
Laparoscopic fundoplication (LF) has been shown to be effective in treatment of gastroesophageal reflux disease (GERD) patients requiring long-term medical therapy. Its effectiveness in patients with poor response to proton pump inhibitors (PPIs) has been questioned. We prospectively followed 445 patients with proven GERD inadequately controlled on PPI (up to 120 mg/d) and 274 GERD patients with good response to PPIs (20–120 mg/d) after LF. Patients in both groups underwent 24-hour pH testing, esophageal manometry, symptoms score evaluation and quality-of-life (QOL) assessment (SF-36) before and at 6 months, 2 years and 5 years after surgery.
Results:
LF was associated with a marked improvement in percentage acid reflux, lower esophageal sphincter pressure, and symptom control in both groups of patients; however, the poor responders to PPIs also had a significant improvement in both physical and mental health component of the QOL assessment.
Conclusions:
Laparoscopic fundoplication provides an excellent symptom control for GERD patients; even those who have responded inadequately to large doses of PPIs. GERD patients who respond poorly to PPI therapy have significantly lowered physical and mental health QOL scores. Laparoscopic fundoplication in this group of patients leads to marked im- provement of both components of QOL by 2 years after surgery.
| Characteristic | Poor responder n = 445 Mean (SD) | Good responder n = 274 Mean (SD) | p |
|---|---|---|---|
| Age | 48.1 (13.6) | 42.6 (12.5) | <0.0001 |
| Gender, % female | 69% | 50% | <0.0001 |
| GERD symptom score off meds | 34.3 (14.8) | 33.7 (12.7) | 0.49 |
| GERD symptom score on meds | 22.6 (14.7) | 13.2 (11.3) | <0.0001 |
| 24-h pH, % < 4 | 8.5 (8.7) | 10.2 (9.7) | 0.0201 |
| LES, mm Hg | 6.3 (5.5) | 6.0 (5.2) | 0.57 |
| QOL physical health | 36.4 (10.8) | 43.5 (10.5 ) | <0.0001 |
| QOL mental health | 43.5 (12.2) | 47.2 (11.3) | 0.0004 |
32. A MODEL FOR EVALUATION OF LAPAROSCOPIC SKILLS: IS THERE CORRELATION TO LEVEL OF TRAINING?
Performance of basic laparoscopic skills has been measured objectively and scored in a trainer box with a video-laparoscopic cart system. A series of structured tasks has been previously developed and described, along with an objective scoring system. The performance scores of all subjects evaluated to date were compared and related to level of training.
One hundred and forty-nine subjects were tested performing the 7 laparoscopic tasks (peg transfers, pattern cutting, clip and divide, endolooping, mesh placement and fixation, suturing with intracorporeal or extracorporeal knots). Performance was measured using a scoring system that rewarded both speed and precision. Student’s t-test was used to evaluate differences between junior (PGY 1, 2, 3) and senior (PGY 4, 5, fellows, and surgeons) participants. Data were analyzed by simple linear regression to assess the relationship of performance to level of training for each task.
There was a significant difference between the performance of junior versus senior participants, and good correlation between level of training and performance for each task. (*p < 0.0001, **p < 0.12.)
Analysis of all participants who have been evaluated with the laparoscopic skills model has shown that there is correlation between level of training and performance on 6 of the 7 tasks, thus showing construct validity. Basic laparoscopic skills models such as this one can become useful in the evaluation and improvement of technical skill in trainees and practising surgeons.
| Task | 1* | 2* | 3** | 4* | 5* | 6* | 7* | Total* |
|---|---|---|---|---|---|---|---|---|
| Junior | 117±7 | 131±54 | 74±21 | 59±38 | 275±78 | 189±152 | 142±80 | 989±333 |
| Senior | 173±46 | 170±53 | 78±20 | 95±30 | 332±67 | 358±117 | 200±80 | 1409±297 |
| r | 0.5 | 0.39 | 0.25 | 0.51 | 0.48 | 0.56 | 0.39 | 0.62 |
33. IMPARTIAL LONG-TERM REVIEW OF VERTICAL BANDED GASTROPLASTY IN A LOW-VOLUME COMMUNITY HOSPITAL PRACTICE
This impartial review of vertical banded gastroplasty in a 228-bed non-teaching community hospital examines whether bariatric surgery can be done well in a low-volume community hospital setting.
All patients more than 2 years postop. were included. Charts were reviewed and patients interviewed by an independent investigator, not associated with the hospital. Results were collated by another author, who had not participated in these operations. Complications, weight loss, change in comorbidities of obesity, patient satisfaction and quality of life (using the SF-36 questionnaire) were assessed.
Thirty-two vertical banded gastroplasties were done 1986 to 1998; 7 were lost to follow-up. Thus, 25 (78%) were followed up 6.2 years (2–13) after surgery. Average age was 32 years (19–44). There were no fatalities, no splenic tears, no stomal stenoses and no symptomatic gastroesophageal reflux. Two reoperations and 5 incisional hernias were noted. BMI fell from 44.3 to 34.9 kg/m≈. Fourteen of the 25 patients (56%) were fully satisfied. Lack of complete satisfaction was noted for all patients whose BMI decreased less than 10 kg/m≈ and, regardless of BMI decrease, for patients whose final BMI was above 35 kg/m≈ or who had reoperations. Hypertension was eliminated in 57% and dyspnea in 55%. Quality of life (SF-36): physical function, physical role and lack of body pain — above 90; general health, social function, emotional role and mental health — above 75; vitality — 56%; and health transition — all patients felt better than a year earlier, 91% much better and 9% somewhat better.
These impartial results from a low-volume community hospital practice are similar to those reported by operators in large specialized series. Obesity is so common, its nonsurgical treatment so ineffective and the vertical banded gastroplasty so well established, that to suggest this intervention be excluded from community hospitals is untenable.
34. COLORECTAL CANCER SCREENING PRACTICES BY FAMILY PHYSICIANS
Controlled studies have shown significant reduction in mortality from colorectal cancers with regular screening of average risk individuals. Public organizations have recently published guidelines supporting routine screening of all individuals over the age of 50. We performed this study to learn if family physicians (FP) have implemented these guidelines in their practices.
We conducted a mail survey of 7855 Quebec FP. Several clinical vignettes of various risk groups for colorectal cancer were presented. FP were asked what screening modality they would recommend for each hypothetical patient as well as the interval at which test would be repeated, considering normal results.
Seven hundred and ninety-seven (10%) questionnaires were returned. For average risk patients, depending on the scenario, 19% to 29% of physicians offered an appropriate initial screening modality and 75% of those offered an accepted screening interval for the chosen modality.
For high genetic risk patients, HNPCC and FAP, 89% and 92% of physicians offered an appropriate initial screening modality in the respective case, but only 60% of those offered an accepted screening interval. For patients with chronic ulcerative colitis, 66% of physicians offered the appropriate initial screening modality and 63% of those, the recommended screening interval.
Most FP are not screening their average risk patients according to the latest guidelines. In this study, high genetic risk patients were offered appropriate methods of screening but there were major variations in the screening interval offered. Although the majority of physicians screen chronic ulcerative colitis patients appropriately there is a large portion that still do not. Correction of observed deviations from the guidelines may have a significant impact on population mortality from colorectal cancer.
35. THYROID SURGERY IN GENERAL SURGERY
This study was done to evaluate the quality of thyroid surgery performed by general surgeons.
We have reviewed the charts of 321 consecutive patients operated for thyroid disease between 1990 and 1997 in our service of general surgery. There were 261 women and 60 men. Mean age was 45 years. Surgery was performed for 55 papillary cancers, 10 follicular cancers, 3 medullar cancers, 4 Hurthle cell cancers, 45 follicular adenomas, 9 Hurthle cell adenomas, 74 vesicular adenomas, 9 benign cysts, 30 nodular hyperplasias, 54 goitres, 9 Graves’ diseases and 18 Hashimoto’s diseases. We performed 195 hemithyroidectomies (HT), 84 total thyroidectomies (TT), 29 subtotal thyroidectomies (ST), 6 isthmectomies and 7 lumpectomies.
Mean operative time was 99 minutes for HT (including frozen sections), 151 minutes for TT and 130 minutes for ST. Neurostimulator was never used to locate recurrent laryngeal nerves. We use closed drain for 24 hours in 99% of cases. Mean hospital stay was 1.7 days for HT and 2.1 days for TT and ST. We had 1 postoperative hemorrhage from the wound after a HT, none in TT and ST. There was 1 reversible recurrent nerve paralysis, and 1 irreversible recurrent nerve paralysis, both occurring after a TT. We noted 17 asymptomatic hypocalcemias and 9 symptomatic hypocalcemias, none requiring long-term therapy
Thyroid surgery performed by an experienced general surgeon is a safe procedure with very low morbidity.
36. ASSESSMENT OF BED UTILIZATION REVIEW TOOLS IN GENERAL SURGERY
We compared 2 tools measuring the “appropriateness” of acute bed utilization in general surgery patients.
The hospitalization days of a random sample of 75 patients on 2 general surgery teaching wards were reviewed using among the most popular commercial instruments: MCAP™ (MCAP) and ISD-AC™ (ISDA). A trained registered nurse performed the primary assessment, and a surgeon subsequently reviewed all inappropriate days. The order of the primary review was randomized, and end points included time to perform the review, ease of use with a visual analog scale (VAS) and appropriateness of each day. For every “inappropriate” day, each reviewer attributed a single hypothetical alternate level of care (ALC) where the patient should have been referred, according to a pre-established list. The possible ALCs were categorized into either reflecting a limitation in available resources or “ineffective” current clinical organization.
Four hundred and thirteen days were reviewed, covering 39 diagnostic related groups, including nonoperated as well as operated patients. The percentage of “appropriate” days with ISDA was 43% versus 60% with MCAP (odds ratio = 1.9, 95% CI = 1.49–2.64, p < 0.0001). For nonoperated patients, ISDA ascertained that 90% of patient-days were inappropriate compared with 53% with MCAP (OR = 7.8, 95% CI = 3.8–17.1, p < 0.0001). The attribution of ALC for “inappropriate” days with ISDA was 1.85 times more likely related to limitations in available resources rather than “ineffective” organization (CI = 1.22–2.8, p = 0.003).
Review of either the whole patient chart or individual days was quicker with MCAP (6 ± 3.35 min per chart, p < 0.0001). MCAP was also deemed easier to use (mean difference by VAS/10 = 1.83, 95% CI = 1.46–2.2, p = 0.0001).
MCAP and ISDA are associated with important differences in interpretation and use in general surgery patients.
37. SURGICAL MANAGEMENT OF PANCREATIC INCIDENTALOMAS
Improved quality and widespread availability of diagnostic abdominal imaging has resulted in increased discovery of incidental intra-abdominal lesions (incidentalomas). The most common incidentalomas are adrenal, hepatic and renal lesions. A preponderance of these lesions are benign and can be followed, usually without biopsy. Less is known about the prevalence, pathology and management of incidental pancreatic masses. In this report the clinical features of patients in whom surgical resection was performed for an incidental pancreatic lesion are examined.
A prospective surgical hepatobiliary database reflecting a single surgeon’s experience was reviewed to identify asymptomatic, resected pancreatic lesions.
Resected pancreatic masses (n = 55) were analyzed for presentation, preoperative imaging and outcomes.
A total of 8 patients underwent resection of an asymptomatic, incidentally discovered pancreatic mass. Six of the lesions were discovered in the last 3 years. A majority of the lesions occurred in women (n = 7) and were located in the tail or body of the pancreas (n = 6). Six lesions were treated with distal pancreatectomy and 2 with pancreaticoduodenectomy. No postoperative death or major morbidity was observed. The most common neoplasms were nonfunctional neuroendocrine (NE) tumours followed by serous cystadenoma (SCA), solid and papillary (SP) and intraductal papillary-mucinous (IPM) tumours (see table). All patients were alive with no evidence of disease at a median follow-up of 14.5 months. Abdominal imaging was reviewed (n = 7 cases) by a radiologist blinded to the final pathology. The working diagnosis based on the radiologic assessment was correct in only 3 of 8 cases.
Improvements in and increased usage of abdominal imaging has resulted in the discovery of more pancreatic incidentalomas. Radiologic examination can direct the surgeon toward resection or watchful waiting but do not accurately predict final histologic diagnosis. The pathology of resected lesions is variable but, in our experience, justified surgical intervention.
| Tumour type | n |
|---|---|
| NE | 4 |
| SCA | 2 |
| SP | 1 |
| IPM | 1 |
38. HEMORRHAGIC SHOCK ATTENUATES THE LPS-INDUCED COUNTERINFLAMMATORY RESPONSE
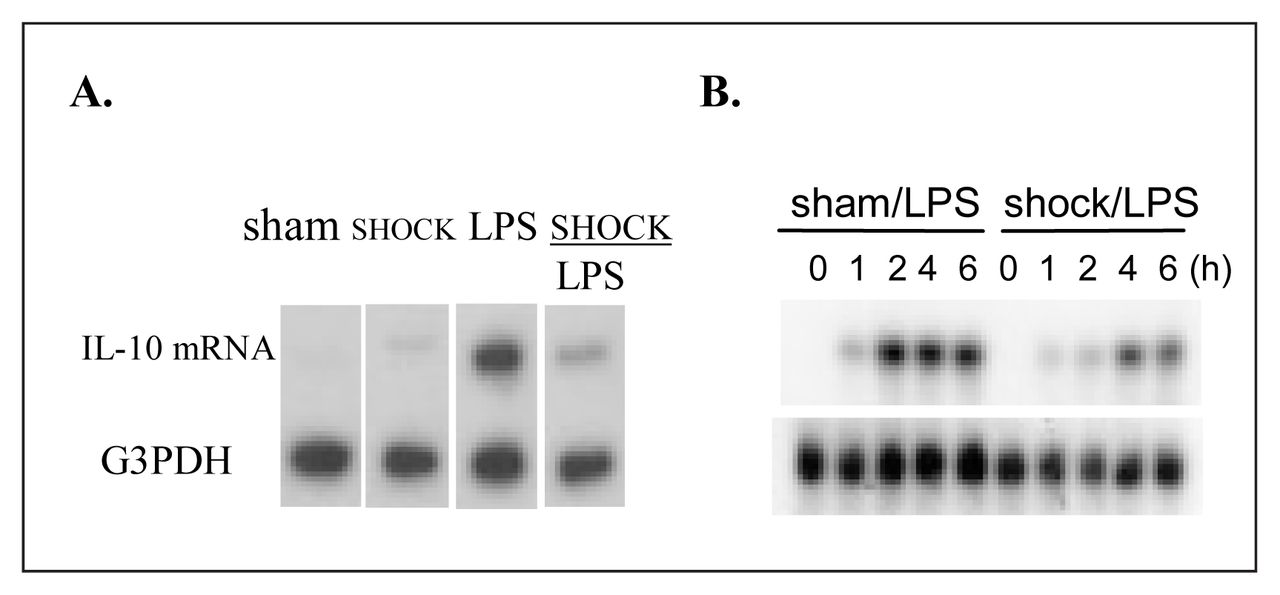
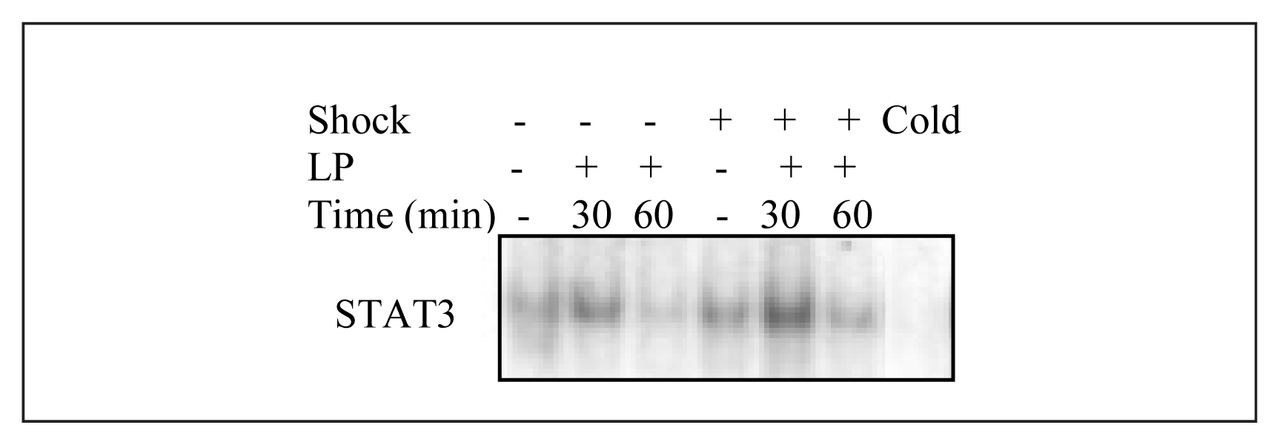
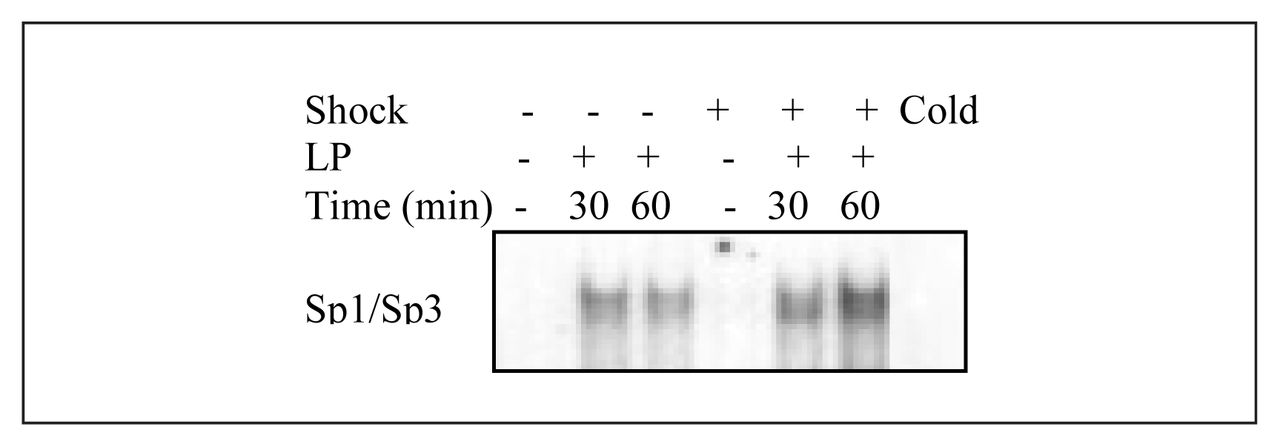
Patients sustaining major trauma are at risk for developing organ dysfunction. We have previously shown in rats that resuscitated hemorrhagic shock primes for increased lung injury in response to LPS. Since counterinflammatory cytokines such as IL-10 can inhibit lung injury, we hypothesized that failed upregulation of IL-10 in animals sequentially exposed to SHOCK/LPS might contribute to exaggerated lung IL-8 expression and hence lung injury. We also hypothesized that the known transcription factors for LPS-induced IL-10, STAT3 and Sp1/Sp3, might be altered by antecedent resuscitated shock.
Rats were bled to a MAP of 40 mm Hg and maintained for 1 hour, then resuscitated with shed blood and equal volumes of Ringer’s lactate. Alveolar macrophages (AM) were lavaged at end resuscitation and exposed to LPS or vehicle for 0 to 4 hours. IL-10 mRNA and protein expression was analyzed by Northern blot and by Western blot respectively. STAT3 and Sp1/Sp3 were analyzed using electrophoretic mobility shift assay.
LPS caused an early rise in IL-10 mRNA in the AM, while antecedent SHOCK both delayed and attenuated the LPS induction (Fig. 1A). The ability of SHOCK to attenuate LPS-stimulated IL-10 was also seen in the protein levels (Fig. 1B). Nuclear extracts of cells recovered from SHAM or SHOCK AM demonstrated no evidence of translocation of either STAT3 or Sp1/Sp3. By contrast, LPS induced a rapid rise in translocation of both STAT3 and Sp1/Sp3 (Figs. 2 and 3). Further, antecedent shock augmented the LPS-induced nuclear translocation of both STAT3 and Sp1/Sp3 compared with LPS alone.
SHOCK suppresses LPS-induced IL-10 mRNA and protein production. The mechanism of this attenuated protective effect is not through the IL-10 transcription factors STAT3 and Sp1/Sp3. Other signalling factors may contribute to the failed LPS-induced upregulation of IL-10 mRNA following shock/resuscitation. This study provides an initial step toward a detailed analysis of the pathways responsible for IL-10 induction. Failed up-regulation of counterinflammatory cytokines such as IL-10 may contribute to augmented organ dysfunction in trauma patients.
39. A THREE-AND-A-HALF-YEAR AUDIT OF FINE-NEEDLE ASPIRATION BIOPSY OF THE THYROID IN SASKATOON, CANADA
The purpose of this study was to assess the accuracy of fine-needle aspiration biopsy (FNAB) of the thyroid in a tertiary care centre in Canada, and compare our results with those reported in specialized centres. A retrospective review of all consecutive FNABs of the thyroid in Saskatoon between July 1996 and December 1999 was performed. A total of 888 aspirates were reviewed. Thirty different cytologic interpretations were reported. These were then classified into 1 of the following 4 categories for statistical analysis: benign, suspicious, malignant or nondiagnostic. Pathology reports from cases going on to surgical resection (n = 196) were then compared to the FNAB results and the sensitivity, specificity, positive predictive value (PPV) and surgical yield of cancer were calculated. A sensitivity of 90%, specificity of 95%, and a PPV of 86% were found. The surgical yield of cancer was 22%. Our results for sensitivity and specificity of FNAB of the thyroid were similar to those reported in previous studies; however, the surgical yield of cancer was at the lower end of the range reported in the literature. Possible explanations for the lower surgical yield of cancer include a relatively high proportion of nondiagnostic aspirates in our series, 27%, and the finding that 29% of patients going on to surgical exploration had previous aspirates interpreted as benign. The lack of a standardized protocol for aspiration technique and pathologic reporting may be partially responsible for these findings. In conclusion, FNAB of the thyroid was found to be accurate at our centre; however, we feel standardization of aspiration technique and pathologic reporting may result in fewer nondiagnostic aspirates and reduced surgical exploration rates.
40. “NEEDLESCOPIC” HELLER MYOTOMY
The purpose of this study is to examine our early experience applying needlescopic technology to the surgical management of achalasia.
A retrospective analysis of Heller myotomy procedures performed at our institution since Jan. 1, 1997 was performed. The results of 14 needlescopic Heller myotomy procedures (utilizing instruments with an external diameter of 2–3 mm) were compared to that of 15 laparoscopic Heller myotomy procedures. Both demographic and short-term outcome data were compared for each group. Analysis was performed utilizing chi-square, Fisher exact test, and Student t-test where appropriate.
Both groups were similar with respect to age (37.1 v. 43.3 yr, p = 0.58) and gender (8/6 v. 8/7, p = 0.84). However, the needlescopic group weighed less. (72.2 v. 83.5 kg, p = 0.049). Intraoperatively, the needlescopic procedures were shorter (98.2 v. 131.9 min, p = 0.03). There were no conversions to open surgery or difference in the number of intraoperative complications (0/14 v. 1/15, p = 1.0) for either group. Postoperatively, the groups were similar with respect to complications (0/14 v. 1/15, p = 1.0), time to normal diet (1.5 v. 2.0 d, p = 0.23) and analgesia requirements (17.1 v. 29.6 morphine equivalents, p = 0.86). Nonetheless, the needlescopic group had a shorter length of stay in hospital (1.1 v. 2.0, p = 0.04).
In selected patients, needlescopic Heller myotomy is a viable treatment option resulting in a shortened operative time, a decreased length of stay and improved wound cosmesis.
41. IS VAGUS FUNCTION INTACT IN PATIENTS WITH GASTROESOPHAGEAL REFLUX AND NONCARDIAC CHEST PAIN?
Cortical evoked potentials (EPs) provide a direct approach to assess afferent autonomic pathways arising from the esophageal mucosa. We hypothesize that patients with noncardiac chest pain (NCCP) or gastroesophageal reflux disease (GERD) may show increased sensitivity to electrical stimulation of the esophagus.
Eight consecutive patients with NCCP (mean age 43 ± 10 yr), 7 patients with GERD (mean age 39 ± 8 yr) and 12 healthy volunteers (mean age 32 ± 8 yr) were studied. We delivered 20 to 24 electrical stimuli to the esophagus (10/min, 200 μs wide at 15 mA) through stainless steel electrodes attached to a standard esophageal manometric tube. Twenty-two gold-plated electrodes were positioned on the scalp using the International 10–20 system. Cortical EPs were recorded using Biologic Brain Atlas (Mundelein, Ill., USA).
The threshold for sensory perception of the stimulus was 7.8 ± 2 mA for controls, 5.1 ± 1.5 mA for GERD patients and 3.6 ± 2 mA NCCP patients (p < 0.04). The control subjects had the following latencies (in ms) of various peaks: 76.4 ± 9.3 (N1), 101.9 ± 5.5 (P1), 141.4 ± 19.4 (N2), 215 ± 23.2 (P2), 262 ± 38 (N3) and 302.7 ± 41 (P3) with an N2-P2 amplitude of 10.55 ± 1.05 μV. The GERD patients had the following latencies of various peaks (ms): 77 ± 9.8 (N1), 99.4 ± 4.8 (P1), 136.5 ± 17.9 (N2), 207 ± 37.1 (P2), 282.3 ± 44 (N3) and 324 ± 32 (P3) with an N2-P2 amplitude of 9.9 ± 2.5 μV. The patients with NCCP had the following peaks: 76 ± 5 (N1), 104 ± 7 (P1), 137 ± 9 (N2), 191 ± 14 (P2), 248 ± 14 (N3) and 324 ± 32 (P3). Amplitude of the main peak in the EP (N2-P2 wave) had the following values: 10.55 ± 1.05 μV for controls, 9.9 ± 2.5 μV for GERD patients and 6.2 ± 1.4 μV for NCCP patients (p < 0.0001).
A decreased threshold for electrical stimulus perception suggests both patient groups have increased esophageal sensitivity compared with controls. A reduced amplitude of the N2-P2 waveform suggests that afferent vagal circuitry may be adversely affected in patients with NCCP group when compared with controls and GERD patients.
42. FIVE-YEAR COMPREHENSIVE FOLLOW-UP OF 181 PATIENTS AFTER LAPAROSCOPIC NISSEN FUNDOPLICATION
Laparoscopic Nissen fundoplication (LNF) has been shown to be an effective antireflux procedure by a number of short-term follow-up studies. Longer follow-up is necessary to prove the effectiveness of this procedure. From August 1992 to November 1995, 271 patients with proven GERD and on long-term medication underwent LNF. Patients underwent a 24-hour pH recording, esophageal manometry, and symptom score assessment for 5 GERD symptoms, and quality-of-life questionnaire (SF-36) preoperatively. All patients were invited and to date 181 (67%) patients have undergone follow-up 5 years after LNF.
Results:
20 patients (7%) have experienced recurrence of reflux symptoms, but only 18 have required repeat surgery. All redo fundoplications for recurrence were carried out successfully laparoscopically. The follow-up results at 5 years after surgery are tabulated below:
Conclusions:
Laparoscopic Nissen fundoplication remains an effective antireflux procedure at 5 years. It is associated with a low recurrence rate. Most recurrences are treated medically, although laparoscopic redo fundoplication is also very effective when necessary. In the majority of patients, there is no significant deterioration in the high pressure zone at LES, percent reflux in 24 hours or symptom control at 5 years following the surgery, suggesting that the longer term results should be satisfactory.
| N = 181 | Before surgery | 5 yr after surgery | p value |
|---|---|---|---|
| % reflux in 24 h | 9.1 ± 9.0 | 1.0 ± 2.2 | <0.0001 |
| LES pressure, mm Hg | 6.2 ± 5.4 | 15.1 ± 8.5 | <0.0001 |
| Symptom score | 34.0 ± 14.1 | 14.5 ± 14.1 | <0.0001 |
| Physical health SF-36 | 39.2 ± 11.3 | 42.2 ± 12.2 | 0.0035 |
| Mental health SF-36 | 44.9 ± 12.01 | 47.4 ± 10.4 | 0.0175 |
Data is presented as mean ± SD.
43. TEACHING APPLIED ANATOMY TO MEDICAL STUDENTS USING LIVE INTERACTIVE LAPAROSCOPIC SURGERY
The purpose of this pilot study was to evaluate the effectiveness of a teaching module incorporating live interactive laparoscopic surgery to teach anatomy and demonstrate the application of this knowledge to surgical treatment of a specific disorder. The test module was based on a case of biliary pancreatitis and consisted of a review of embryology and anatomy of the GI tract and biliary system using a computer animated presentation, review of different radiologic and radionuclide investigations of the GI tract and biliary system, and use of 3D reconstruction of various GI abdominal organs. The students then observed a live surgery projected by ATM lines into the conference room onto a large screen. The students were able to interact live with the surgeon. The surgery consisted of a laparoscopic cholecystectomy in a patient with gallstones. The surgeon demonstrated the main features of the abdominal anatomy with specific attention to the biliary system and then carried out the cholecystectomy demonstrating the importance of the knowledge of the anatomy of the region for safe performance of the surgery. After completion of the surgery the students moved into the minimal access skills laboratory and used an artificial Silastic cadaver (Limbs & Things, Prior Lake, Minn.) to dissect the cystic duct and artery. They also used computerized 3D programs to practise 2-handed laparoscopic skills and perform pre-designed tasks (Mist VR, Virtual Presence, London, UK).
One hundred medical students completed the pilot project. The students went through each module in groups of 10 to 12, for a total of 8 sessions. They evaluated each segment of the session on a scale of 0 (useless) to 10 (excellent). The average score for all sections of the module was over 9 out of 10. The pilot study was an overwhelming success and the students have asked for more modules on other organs and disorders. Similar modules are currently being developed for gastroesophageal disorders, bowel disorders, kidney and urinary tract, pulmonary disorders, cardiac and vascular disorders.
44. MESH PLUG MIGRATION
A case series of 3 incidental findings of mesh plug migration into the peritoneal cavity.
Four cases relating to mesh plug migration were discovered in our MEDLINE search with 1 migrating into the peritoneal cavity causing acute intestinal obstruction.
Mesh plug migration is an uncommon and possibly unrecognized complication of mesh plug hernioplasties.
45. EXAMINING DOUBLE GLOVING ATTITUDES
The aim of this study is to determine the attitudes surrounding double gloving and other universal precautions utilized in the operating room by surgeons in Edmonton, Alta. It examines the rationale for not double gloving and attempts to change this behaviour.
A questionnaire was developed after reviewing pertinent literature on surgical safety issues. The questionnaire was sent out to all staff physicians and residents in the specialties of general surgery, orthopedics, obstetrics and gynecology, urology, plastic surgery, otolaryngology, cardiovascular surgery, and neurosurgery. A double mail-out design was used. A second questionnaire containing recent research on safety issues was sent to all general surgeons and general surgery residents to explore whether or not they would change their practice based on this information.
Of the 268 surgeons sent the original questionnaire, 170 replied (63.4 % response rate.) Fifty-eight point three percent of the respondents do not double glove (highest ratio — 100% of urologists; lowest ratio — 12.5% of orthopedic surgeons). The most common reason (45.9 %) was a decrease in manual dexterity. Ninety-seven percent of respondents are immunized for hepatitis B with 53.2% having had their titre checked in the last 3 years. Thirty-seven second questionnaires were mailed out. Early numbers show that 55.6% would change their practice and begin to double glove.
Safety should be of the utmost importance to the surgeon in the operating room. The majority of surgeons actively participate in basic universal precautions. However, given the low double gloving rate and lack of regularly checked hepatitis B titres, it appears that most are reluctant to incorporate further safety measures into their practice. When provided with additional information supported by research, surgeons contemplate embracing new safety techniques.
46. “PORCINE” LIVE DONOR PARTIAL HEPATECTOMY: DEVELOPING A MIS TECHNIQUE
The application of advanced laparoscopic techniques to hepatic surgery is evolving, suggesting a role for MIS in liver transplantation surgery. The purpose of this animal study was to develop a MIS technique using a porcine model for live donor partial hepatectomy.
Four pigs underwent laparoscopic live donor partial hepatectomy removing the 2 great left lobes in an effort to mimic left lateral segmentectomy in the human. In each case the porta hepatis was explored and the vascular and biliary structures were isolated and transected only after completion of hepatic parenchymal dissection. The hepatic parenchyma was transected using the HALS technique in combination with ultrasonic shears, hemostatic clips, and endo-linear staplers with vascular cartridges. Graft viability was assessed by measuring warm ischemic time, confirming vascular integrity with angiogram, and examining the graft for evidence of injury.
The mean operating time was 275 minutes. There were 2 successful procedures where the blood loss was 250 mL and 500 mL and the warm ischemic time was 255 and 510 seconds. For each successful procedure, an angiogram confirmed vascular integrity and histology confirmed parenchymal preservation. Two experiments were considered to be failures secondary to complications. A significant intraoperative complication occurred in experiment #2 with major laceration of the middle hepatic vein which was not amenable to laparoscopic repair. In experiement #4, the left hepatic vein bifurcated near the vena cava origin and our resection resulted in 2 separated lobes.
Laparoscopic live donor partial hepatectomy is technically feasible in the porcine model. The technique developed in this study could potentially have clinical application in humans.
47. EFFECT OF RESIDENTS ON OUTCOMES OF LAPAROSCOPIC CHOLECYSTECTOMY
In laparoscopic surgery only one pair of hands controls the instruments and operative field, so the proceptor is not as close to the operation as in open surgery. This study reports on the effect of introducing trainees into an established laparoscopic practice.
Prospective contemporaneous records were kept for all laparoscopic cholecystectomies of 3 consecutive senior surgical residents coming to a nonteaching hospital with no previous house staff. Trainees were allowed to operate after adequate demonstration, with the attending surgeon assisting throughout all operations. Results were compared to the attending surgeon’s most recent pre-resident operations, matched for age, sex, ASA status, weight, previous abdominal surgery and disease acuity.
There were 39 resident operations, including 3 taken over by the attending surgeon. Mean operative time and standard deviation were greater for residents (p < 0.05). Perioperative complication rates (give-up, reoperation, conversion and admission) were higher for resident operations (p < 0.05) as were wound infection rates (p < 0.05) (see table).
Laparoscopic surgery does not lend itself to controlling trainees’ movements as well as open surgery. In addition to an expected increase in operative time and standard deviation, despite supervision, there is an increase in combined perioperative complications (give-up, reoperation, conversion and admission rates) as well as wound infection rate. This poses an ethical dilemma, which, at the very least, must form an integral part of informed consent when residents perform laparoscopic surgery.
| Comparator | Residents | Staff | p:0.05 |
|---|---|---|---|
| Op Comp | 23% | 5% | < |
| Wd inf | 15% | 0% | < |
| Time | 41 min | 27 min | < |
| SD | 14 min | I8 min | < |
48. ROLE OF PARATHYROID HORMONE-RELATED PROTEIN IN ANAPLASTIC THYROID CANCER
The role of parathyroid hormone-related protein (PTHrP) as the mediator of humoral hypercalcemia of malignancy is well recognized. Recent studies have suggested additional effects of this protein including a possible signalling/cytokine role. Anaplastic thyroid cancer is one of the most aggressive human malignancies with a mean survival of only 2 to 6 months. Recent studies from our laboratory have demonstrated that manumycin, a farnesyltransferase inhibitor and inhibitor of ras activation, decreased anaplastic thyroid cancer cell proliferation and induced apoptosis. We hypothesized that the mechanism of the manumycin treatment effect may be mediated by PTHrP and that modulation of PTHrP levels may have potential therapeutic benefit in anaplastic thyroid carcinoma.
Studies were performed in 2 anaplastic thyroid cancer cell lines (Aro, Kat-4). Immunohistochemistry demonstrated intense nuclear staining with anti PTHrP antibody. To investigate a possible intranuclear signalling role of PTHrP, nuclei were then isolated using density centrifugation and differential detergent extraction techniques (>90% purity achieved). By Western blot analysis, manumycin decreased nuclear PTHrP suggesting a mechanism for its antiproliferative effect. Further, anti-PTHrP antibody decreased anaplastic thyroid cell proliferation in a cell proliferation assay (Wst-1). Thus, modulation of cellular PTHrP may be of therapeutic benefit in anaplastic thyroid cancer and other poorly differentiated malignancies.
49. EARLY EXPERIENCE WITH LAPAROSCOPIC ILEAL POUCH–ANAL ANASTOMOSIS FOR ULCERATIVE COLITIS
The purpose of this study is to describe our MIS technique and outline perioperative and medium-term outcomes in those undergoing laparoscopic ileal pouch–anal anastomosis (LIPAA) for ulcerative colitis.
Data was obtained from a prospective database of over 700 colorectal procedures. Long-term follow-up data was obtained by telephone interview.
Ten LIPAA were performed (5 males, 5 females), all of whom had previously undergone total abdominal colectomy with ileostomy. Median operative time was 255 minutes (range, 200–398) with 1 conversion due to adhesions. There were no deaths or intraoperative complications; however, 6 patients experienced 7 postoperative complications within 30 days of final closure of defunctioning ileostomy (2 leaks, 2 wound infection, 1 pulmonary embolus, 2 reoperation for small-bowel obstruction). Median length of stay was 7 days (range, 5–13).
Median follow-up was 34 months (range, 14–66). The average number of day and night bowel movements was 5.7 (range, 3–9) and 1.6 (range, 1–3) respectively, with 5 requiring medication to control frequency. None had incontinence of stool or retrograde ejaculation, however, 1 had occasional incontinence of gas, 3 had occasional nocturnal soiling and 1 was impotent. Three patients (30%) had pouchitis all treated successfully with oral antibiotics. All patients were satisfied with the outcome of their operation and preferred their pouch to previous ileostomy. Patients reported their overall social, emotional and physical well-being to be satisfactory to excellent. Results of the SF-36 were similar to those from studies of patients following an open pelvic pouch procedure.
LIPAA is technically feasible in experienced centres. We feel that the technique is still evolving and that more time and experience is required to refine the procedure.
50. PROSPECTIVE VALIDATION OF A MODEL FOR PREDICTING CONVERSIONS TO OPEN SURGERY IN LAPAROSCOPIC COLORECTAL RESECTIONS
The objective of this study was to prospectively validate a previously developed clinical model for predicting conversions to open surgery in laparoscopic colorectal resections.
This scoring system awarded points for 3 predictive factors: diagnosis of malignancy (1 point), surgeon experience of 50 cases or less (1 point) and weight level (60 to 90 kg, 1 point, >90 kg, 2 points). This model, originally derived from 367 procedures performed by one surgical group between 1991 and 1998, was prospectively applied to 248 subsequent procedures performed by the same group including 1 new fellowship-trained minimally invasive surgeon.
The overall conversion rate was 8.9%, unchanged from previous experience. Expected trends of higher conversion rates for increasing weight level (6.8%, <60 kg, 9.0%, 60 to 90 kg, 12.1%, >90 kg, p > 0.05) and a diagnosis of malignancy (10.1% v. 7.3% for benign disease, p > 0.05) were observed. However, the conversion rates for scores of 0 to 4 points did not appear to be different among groups (8.0%, 6.9%, 10.8%, 7.9% and 20%, respectively). The fellowship-trained surgeon, contrary to the model, had a conversion rate that was not higher than the rest of the group (7.4% v. 9.3%, p > 0.05). Recalculated scores that excluded the inexperience penalty demonstrated good fit of the model (chi square = 4.43, p = 0.729) and an orderly stepwise progression.
Fellowship training in minimally invasive surgery appears to reduce or eliminate the learning curve in laparoscopic colorectal surgery. After eliminating the inexperience penalty for the fellowship-trained surgeon this model predicted risk categories for conversion to open surgery. This validates the predictive value of this model for one surgical group.
| Total score | Procedures | Converted | Unconverted | ||
|---|---|---|---|---|---|
| Predicted | Actual | Predicted | Actual | ||
| 0 points | 31 | 0 | 2 | 31 | 29 |
| 1 point | 93 | 4 | 7 | 89 | 86 |
| 2 points | 104 | 12 | 10 | 92 | 94 |
| 3 points | 20 | 6 | 3 | 14 | 17 |
51. MANAGEMENT OF HIGH-RISK PATIENTS WITH ACUTE CHOLECYSTITIS BY PERCUTANEOUS CHOLECYSTOSTOMY FOLLOWED BY LAPAROSCOPIC CHOLECYSTECTOMY
Fifty-one consecutive patients undergoing percutaneous cholecystostomy between January 1995 and December 2000 were reviewed. Patients were reviewed with attention given to indications for cholecystostomy and outcome of the cholecystostomy. All patients had significant comorbidity.
Fifty-one patients had a percutaneous cholecystostomy. Seventeen tubes were placed for a presumed diagnosis of acalculous cholecystitis, 34 were placed for calculous cholecystitis. Of the patients with tubes placed for calculous cholecystitis, 15 underwent cholecystectomy. One patient underwent urgent laparoscopic cholecystectomy for bile leak and cholecystitis following removal of the tube. Twelve patients had attempted laparoscopic cholecystectomy, 9 were successful and 3 were converted to open procedures due to adhesions preventing visualization of the gallbladder. Four patients underwent open cholecystectomy, 3 because of the attending surgeon’s preference and 1 for known cirrhosis. No patients had significant morbidity from their cholecystectomy. Nine of 11 patients had successful laparoscopic procedures (81%).
Three thousand and fifty-four cholecystectomies were performed at the local institution during the period reviewed. Patients with percutaneous cholecystostomies represent a very specific subset of patients. The local experience suggests that laparoscopic cholecystectomy can be safely performed following percutaneous cholecystostomy in these patients. Percutaneous cholecystostomy followed by interval laparoscopic cholecystectomy is a suitable alternative procedure for high-risk surgical patients with calculous cholecystitis.
52. p66Shc — A NOVEL MARKER OF TUMOUR PROGRESSION IN BREAST CANCER
The mechanisms responsible for malignant transformation in breast epithelium remain largely unknown. The p46/52 isoforms of the mammalian proto-oncogene Shc have been implicated in cellular transformation in vitro. However, the role of the third isoform, p66Shc, in cell transformation and breast cancer is unknown. The purpose of this study was to evaluate the function of the Shc proto-oncogene in breast cancer.
Shc expression was determined by immunoprecipitation and Western blotting in 11 breast cancer cell lines. p66Shc was transfected into a non-p66Shc expressing fibrocystic derived breast cell line, MCF10A, to determine the effects of p66Shc on anchorage independent growth and tumour progression. p66Shc expression in tumour tissue was determined by immunohistochemistry (IHC) of paraffin-embedded tumour blocks, using p66Shc specific sera, in 33 stage I and 28 stage III breast cancer patients. Statistical analysis was performed by χ2 test.
All breast cancer cell lines examined expressed the p46/52 Shc isoforms at equal levels. Strikingly, p66Shc was differentially expressed and expression correlated with a loss of epithelial architecture, a more dispersed growth pattern and a more transformed phenotype (8 out of 11 lines). Moreover, the introduction of p66Shc into a p66Shc-negative fibrocystic derived breast cell line promoted increased anchorage independent growth, a hallmark of cell transformation. Furthermore, IHC using p66Shc-specific sera indicated a significantly (p < 0.01) greater expression of p66Shc in more advanced breast cancers (Table).
This study demonstrates that the p66Shc isoform is a new marker of tumour progression and can play a pivotal role in breast cancer progression. Better understanding of this role will provide development of new therapeutic strategies.
| Staining | Stage I (n = 33) | Stage III (n = 28) |
|---|---|---|
| Low | 17 (51.5%) | 9 (32.1%) |
| Intermediate | 14 (42.4%) | 7 (25.0%) |
| High | 2 (6.1%) | 12 (42.9%) |
53. EARLY POSTOPERATIVE SMALL-BOWEL OBSTRUCTION — A 16-YEAR RETROSPECTIVE ANALYSIS
Small-bowel obstruction (SBO) is a particularly vexing problem in the postoperative period. Goals of this study were to highlight risk factors for this entity and to compare the results of operative versus nonoperative treatment.
The medical records of patients at a university affiliated hospital (1985–2000) who developed SBO after undergoing a laparotomy during that admission were reviewed retrospectively. Postoperative SBO was defined as cessation of flatus or bowel movements after their resumption following operation.
Of 52 patients who developed SBO in the immediate postoperative period, 37 were male, 5 had inflammatory bowel disease, 6 had a previous SBO, 25 had colorectal surgery and 9 had a gastrectomy as the initial operation on admission; 22 had virgin abdomens prior to the current operation and 11 had adhesions noted at the initial operation. The median time to the development of obstructive symptoms was 8 days (range 1–33). The reoperation rate was 42% overall (67% in women and 32% in men, p = 0.02). For operatively treated patients, the median time between onset of symptoms and surgery was 5 days (range 1–23). The median time to the return of bowel function was greater in the operatively treated patients compared to nonoperatively treated patients (11.5 days [range 4–37] v. 6 days [range 1–28], p < 0.0001), as was median length of stay, from onset of obstruction, (23 days [range 6–60] v. 12 days [range 2–45], p = 0.009).
Early SBO can be treated nonoperatively in stable patients resulting in significantly quicker return of bowel function and shorter lengths of hospital stay.
54. MANAGEMENT OF SPLENIC INJURIES: A 5-YEAR EXPERIENCE AT A CANADIAN TRAUMA CENTRE
A retrospective study comparing operative versus nonoperative management of 159 adult patients with blunt splenic injuries over 5 years at a Canadian trauma centre, and identifying those factors associated with an increased risk of failure. Statistical analysis included Pearson χ2, Wilcoxon rank sum and multiple logistic regression generating odds ratio and 95% confidence intervals. Our study shows that 52% of adults with blunt splenic injuries can be managed nonoperatively with only a 6% failure rate. Multiple logistic regression demonstrates that a severe splenic injury (AIS 4 or 5) increases a patient’s odds of being managed operatively by nearly 7 times, while a high PTT (>32 s) quadruples one’s chances of going to the OR. Age, shock, neurologic status, and number of pRBCs transfused did not lead to increased operative management.
55. TAMOXIFEN FOR BREAST CANCER CHEMOPREVENTION: A “PARADIGM SHIFT” WITH AN INSIGNIFICANT EFFECT ON CLINICAL PRACTICE
The Breast Cancer Prevention Trial (BCPT) published results in September 1998 demonstrated that the use of tamoxifen in high-risk women reduces the incidence of invasive breast cancer by 49%. The FDA has since approved the use of tamoxifen for breast cancer chemoprevention in this population of women. This study examines the clinical impact of the BCPT, to determine if high-risk women are taking tamoxifen for chemoprophylaxis and to investigate the factors influencing this decision. Eighty-nine high-risk women, as defined by the Gail model, were sent notification of their elevated risk following evaluation in our breast assessment clinic. They were explained that there exists a medication demonstrated to reduce breast cancer risk, and were encouraged to discuss its therapeutic use with their family physician. Each family physician was sent a letter notifying them of their patient’s increased risk along with copies of the 3 largest tamoxifen chemoprevention studies including the BCPT. Follow-up was conducted by telephone to determine each woman’s choice regarding tamoxifen use. Of the 89 high-risk women included in the study, 1 decided to take tamoxifen for breast cancer chemoprevention. Forty-eight women (54.5%) discussed the issue of taking tamoxifen with their family physician. The family physician recommended the use of tamoxifen in 3 cases, made no recommendations in 8 cases and in the remaining 37 cases the family physician advised against tamoxifen. The most frequently cited factors influencing this decision were a fear of adverse effects (46.8%), the family physician’s decision (31.9%) and a perceived low risk (34%). Noted side-effects included blood clots, uterine cancer and symptoms such as hot flushes. Women are unwilling to take tamoxifen to reduce their risk of breast cancer, and family physicians are reluctant to recommend the use of tamoxifen to their patients. The major barrier appears to be the lack of agreement as to when the benefit of tamoxifen in reducing the incidence of invasive breast cancer outweighs the risks incurred by tamoxifen’s serious adverse effects. An algorithm, developed by Gail et al, to subclassify patients by risk/benefit ratio is summarized in the discussion. It is anticipated that this will facilitate more informed discussions and decisions surrounding tamoxifen use for chemoprophylaxis.
56. MICROSATELLITE INSTABILITY IN THE DEVELOPMENT OF COLITIS-ASSOCIATED NEOPLASIA
The molecular events involved in the development of colitis-associated neoplasia (CAN) remain poorly understood. The purpose of this study was to determine the presence of microsatellite instability in a relatively large cohort of CAN.
Archival pathology specimens with the diagnoses of IBD and either dysplasia or carcinoma were identified. Neoplastic areas were microdissected, and microsatellite instability (MSI) status was determined using PCR-based techniques. All cases also underwent immunohistochemical staining to detect expression of hMLH-1 and hMSH-2. Cases displaying high frequency MSI and loss of expression of hMLH-1 were assayed to determine hypermethylation of hMLH-1.
One hundred and sixteen CANs were identified in 87 patients. There were 86 cancers, 14 DALMs, and 16 high-grade dysplasias. Four of the cancers were found to be high-frequency microsatellite instability (MSI-HI) tumours, while none of the dysplastic lesions were MSI-HI. All 4 of the MSI-HI tumours had loss of expression on immunohistochemistry; 3 had loss of hMLH-1 expression, while 1 had loss of hMSH-2 expression. None of the tumours showed evidence of hMLH-1 hypermethylation.
Colitis-associated neoplasia remains poorly understood. Microsatellite instability appears to play a small role in the development of these neoplasms. Continued research in this area is warranted to identify novel genes that might allow early identification of patients at risk for neoplastic transformation.
57. THE FRENCH CONNECTION: AN EXTRAMUCOSAL BOWEL ANASTOMOSIS TECHNIQUE
The best technique for connecting 2 pieces of bowel remains controversial. We describe a bowel anastomosis technique that originated in France. Bowel is approximated using a continuous single-layer 5.0 polydioxanone suture on a fine round-bodied vascular needle. Knots are tied on the outside and each suture bite encompasses seromuscular and submucosal layers and does not include the mucosa. Bites are 3 to 4 mm deep and 3 to 4 mm apart. Where possible the bowel mucosa is not opened until after the posterior wall is completed. The records of patients in whom this technique was utilized over a 2-year period were reviewed. Ninety-seven patients received 113 different anastomoses. Most of the anastomoses were in the upper gastrointestinal tract as a part of a hepatobiliary or pancreas procedure (pancreaticoduodenectomy 27, palliative bypass 18, hepaticojejunostomy 27, pancreaticojejunostomy 8, other 17). There were 7 different types of anastomoses performed: end–side jejunojejunostomy — 53, end–side duodenojejunostomy — 23, side–side gastrojejunostomy — 22, end–end entero-enterostomy — 8, end–end ileocolostomy — 3, end–side ileocolostomy — 2 and end–end colocolostomy — 2. Intraoperatively, 2 patients required their anastomoses be redone due to bowel edge hematoma. Postoperatively 1 patient had a possible leak that was treated conservatively. One patient post pancreaticoduodenectomy had a significant intraluminal bleed whose origin could have been the duodenojejunostomy. No patients required reoperation for anastomotic leakage, bleeding or stricture formation. This continuous single-layer extramucosal bowel anastomosis technique is a secure way on connecting any 2 pieces of bowel.
58. CAUSES OF INCREASED LENGTH OF STAY ON A GENERAL THORACIC SURGERY SERVICE: A PROSPECTIVE OBSERVATIONAL STUDY
The recent re-allocation of hospital resources has dramatically reduced the availability of acute hospital beds for elective surgical patients. We conducted a prospective observational study in order to characterize medical and nonmedical reasons for a delayed discharge on a thoracic surgery unit.
Between February 1999 and July 2000, we prospectively evaluated the in-hospital progress of 130 patients following an elective thoracic surgery procedure at the MUHC. On a daily basis, the surgeon recorded any complications and judged whether the patient was medically ready for discharge. The day the patient was deemed fit for discharge (medically required length of stay) was compared with the actual day of discharge (actual length of stay).
The 3 most frequent medical complications that delayed discharge were persistent air leaks, pulmonary infections and atrial fibrillation. The presence of persistent air leak increased the medically required length of stay by 13.1 days (11.0–15.2, 95% CI), pneumonia by 9.6 days (4.96–14.2, 95% CI) and atrial fibrillation by 2.4 days (−2.6–7.4, 95% CI).
The mean medically required length of stay was 6.9 days, and this differed from the actual length of stay (7.35 d, p = 0.01), contributing 45 excess days of hospitalization per 100 patients. The causes of this discrepancy were the lack of home support (10.6% of patients) and the unavailability of convalescent facilities (7.5% of patients). A prolongation of hospital stay for nonmedical reasons was associated with increased mean age (67.4 v. 60.7, p = 0.05).
Length of stay following elective thoracic surgery may be prolonged for medical or nonmedical reasons. The unavailability of home care and convalescent facilities prevented discharge from a tertiary care hospital in 18.1% of our patients. This emphasizes the importance of a quicker transition to a less cost-intensive setting.
59. COVERED SELF-EXPANDING METAL STENTS VERSUS PLASTIC PROSTHESES FOR THE PALLIATION OF DYSPHAGIA DUE TO INOPERABLE ESOPHAGEAL STRICTURES
Self-expanding metal stents (SEMS) have replaced conventional plastic prostheses for the treatment of inoperable esophageal strictures because of the high complication rates, suboptimal palliation of dysphagia and reduced survival associated with plastic stents. However, studies comparing conventional stents and SEMS have not demonstrated consistent results and, moreover, recent studies have demonstrated excellent results with conventional prostheses. The present study was designed to compare the safety and efficacy of conventional plastic Atkinson stents versus covered Ultraflex™ stents for the palliation of dysphagia due to inoperable esophageal strictures. A total of 40 patients underwent esophageal stent placement at our institution between 1989 and 2000. Eight patients were treated with an Atkinson stent and 32 patients with a covered Ultraflex™ stent. The data was collected retrospectively for the conventional groups and prospectively for the Ultraflex™ group. The degree of palliation, incidence of complications, survival and length of stay were compared in both groups. Technical success was similar in both treatment groups (88.5% v. 96.9%, p = NS). The improvement in the dysphagia scores post stent was 2.13 in the SEMS group as compared to 0.25 in the conventional group (p < 0.000). The immediate complications rate was significantly higher in the conventional group (62.5% v. 25%, p = 0.16) as was the mortality at 1 week (62.5% v. 12.5%, p = 0.002). In the Ultraflex™ group 13 late complications occurred in 10 patients and included tumour overgrowth (4 cases), food bolus impaction (4 cases), stent migration (2 cases), pneumonia and TEF (3 cases). Reintervention was required for 9 patients in the Ultraflex™ group. Survival was significantly longer in the Ultraflex™ group (13 d v. 137 d, p = 0.00). SEMS provide superior palliation of dysphagia and are associated with significantly fewer immediate complications and improved long-term survival.
60. EFFICACY OF LAPAROSCOPIC COLLIS–NISSEN GASTROPLASTY FOR THE TREATMENT OF ESOPHAGEAL SHORTENING
Esophageal shortening (ES) has been recognized as a factor that may lead to failure of standard laparoscopic Nissen fundoplication for severe gastroesophageal reflux disease (GERD). This study reviewed the efficacy of laparoscopic Collis–Nissen gastroplasty (LCNG) for the treatment of complex GERD presenting with ES.
Since January 1998, approximately 500 patients with GERD have been evaluated at our 2 institutions. Of these, 54 patients (23 men, 31 women) with a mean age of 57 (range 18–85) underwent LCNG. A retrospective review of these patients was performed with 100% follow-up (median 8.1 mo) obtained by cross-sectional contact as of January 2001.
In 85% of cases, patients presented with typical GERD symptoms. Preoperative testing included barium esophagogram and esophagogastroduodenoscopy (100%), esophageal manometry (62%), and 24-hour pH study (22%). Preoperative hernia classification was: I (50%), II (12%), III (34%), IV (4%). Indications for gastroplasty included obvious ES preoperatively (60%) and subtler degrees of ES identified intraoperatively (40%). For all cases, mean operative time was 4 hours 28 minutes. Mean operative time for the last 20 cases was decreased to approximately 3 hours. There were 6 (11%) intraoperative complications (1 transected vagal nerve, 5 pneumothoraces). There were 4 (7%) major postoperative complications of which 2 were pulmonary emboli and 2 staple line leaks. Both leaks occurred in our early experience (first 20 cases) with 1 repaired laparoscopically and 1 by open technique. No operative mortalities were reported. Median hospital stay was 3 days (range 2–25). Subjective follow-up results were good (improved with occasional symptoms) to excellent (asymptomatic) in 52 patients (96%), and poor (unimproved or worse) in 2 patients (4%).
Conclusions:
LCNG for complex GERD presenting with ES is technically challenging but feasible. Although long-term follow-up is required, short-term subjective evaluation suggest sthat the majority of patients obtain good to excellent results.
61. IS THE RADIOLOGIC RESPONSE OF PANCOAST TUMOURS PREDICTIVE OF PATHOLOGIC RESPONSE?
This study evaluates the role of imaging in determining response of Pancoast tumours to chemoradiation and surgery. It is unclear from previous studies whether the radiologic response measured by tumour size reduction on CT and/or MR post-induction therapy should influence the approach to further treatment. Similarly, radiologic response may not predict pathologic response. Lack of correlation between radiologic response and pathologic response has been noted previously with radiotherapy for other tumours, but has not been reported with respect to Pancoast tumours.
The records of 19 patients with Pancoast tumours treated from 1995 to present were reviewed. Pre- and post-induction tumour sizes were recorded based on CT and MRI reports and the percent size reduction was calculated based on change in tumour area. Radiologic response was defined as a decrease in area of at least 50%. Pathologic response was assessed based on the pathology reports of the resected specimens and divided into pathologic complete response (pCR) and incomplete or no response (pNCR) groups. The ability of radiologic response to predict pCR was determined. Radiologic response was also compared amongst progressors (defined as those developing distant disease during induction treatment).
Five of 19 patients developed progressive disease during induction treatment and did not go on to operation. Two of these 5 had a radiologic response. Fourteen of 19 underwent operation with a complete resection rate of 100%. Fifty percent were classified as pCRs. Six of 14 patients had a radiologic response and 4/6 of these had a pCR. On the other hand, 3/8 of those without a radiologic response had a pCR. Thus, the positive predictive value of radiologic response to predict pathologic CR was 66.7% while the negative predictive value was 62.5%.
Radiologic response was not predictive of a pathologic complete response. It should not be considered a reflection of resectability and should not influence the approach to treatment. Nonetheless, post-induction imaging remains helpful in planning the technical aspects of the resection and to rule out the development of distant metastatic disease.
62. MONITORING STAGE I AND II LUNG CANCER PATIENTS POST-THORACOTOMY USING LOW-DOSE SPIRAL CT
Low-dose spiral CT (LDCT) is more sensitive than chest x-ray (CXR) for the detection of lung nodules, and is being used to screen asymptomatic smokers for early stage lung cancer. In stage I and II lung cancer patients who have undergone curative resection, the rate of a second primary lung cancer is approximately 3% to 4% per year. We reasoned that serial LDCT will allow the earlier detection of second primary lung cancers in this high-risk group compared with concurrent CXR.
Over a 1-year period (November 1999 through October 2000) we obtained LDCT on 59 post-thoracotomy patients with either stage I or II non-small lung cancer (mean time since surgery 5.3 yr, range 10.5–0.4 yr).
No lung nodules were seen in 22/59 patients (37%), while a total of 40 noncalcified nodules 2 to 7 mm were found in 28/59 pts (47%). These smaller nodules will be followed with serial LDCT scans at 3 to 12-month intervals depending on the size and characteristics of the nodule. Ten larger nodules (average 18 mm, range 8–34 mm) were seen in 10/59 pts (17%). Four of the 10 patients have undergone resection of a second primary lung (3 stage IIB and 1 stage IA). Five of the 10 patients have stable nodules compared with previous CTs and CXRs and are being observed. One patient has a thyroid mass with mediastinal adenopathy. Where concurrent CXR is available (9 of 10 patients), only 33% of the noncalcified nodules 8 mm or greater were identified on CXR.
The ability of LDCT to identify early stage second primary lung cancers compares favourably to conventional chest radiography in the post-thoracotomy stage I and II lung cancer patients. These findings are the basis for an ongoing trial comparing LDCT with CXR in monitoring post thoracotomy lung cancer patients.
63. LUNG TRANSPLANTATION FOR CYSTIC FIBROSIS
From 1994 to 2001, 19 bilateral sequential lung transplants and 1 bilateral lower lobar transplant were performed for patients with end-stage cystic fibrosis. Retrospective data was collected and entered into a database, and newer data was collected prospectively. Follow-up is complete on all patients transplanted. Student’s t-test was used to test for significant improvement in spirometry post-transplant.
There were 3 in-hospital deaths, including 2 perioperative deaths, from coagulopathy and from acute right ventricular failure, and a death at 52 days, from Aspergillus superinfection and lymphoproliferative disease in the setting of an Epstein–Barr virus mismatch. There were 5 late deaths, ranging from 346 to 1974 days after transplant. Four deaths were due to chronic rejection, while 1 was due to respiratory failure from diffuse alveolar damage. The 1- and 5-year survivals for patients at risk were 80% and 57% respectively. At present, 12 of 20 patients transplanted for cystic fibrosis are still alive. The mean FEV1 at baseline, 12 months and 24 months were 0.69 ± 0.16 L, 2.42 ± 0.92 L and 2.25 ± 1.09 L respectively, with a significant improvement seen post transplant (p < 0.0001).
The functional results and survival after lung transplantation for cystic fibrosis in Manitoba are comparable to those of larger centres. Chronic rejection remains a problem for our local transplant population.
64. CLINICAL APPROACH TO 44 PATIENTS WITH HYDATID CYSTS
Hydatid cystic disease is endemically encountered in Turkey. We here present a retrospective analysis of patients with hydatid cyst disease who were hospitalized during a 5-year period (January 1995 to December 2000). We analysed the patients with respect to preoperative signs, surgical methods and postoperative follow-ups, and reviewed the literature. The patients had pulmonary cysts alone or pulmonary and hepatic cysts. Diagnosis and operative decisions were based on the findings of plain chest radiography, abdominal ultrasonography and thoracoabdominal tomography. Nine patients had simultaneous hepatic and pulmonary hydatid cysts, and 1 of these also had a splenic cyst. We performed right thoracophrenotomy and cystotomy/capitonnage for pulmonary cysts, and cystotomy alone for hepatic cysts. Thirty-one patients with pulmonary disease alone underwent thoracotomy/cystotomy/capitonnage, and 2 patients underwent decortication. We used median sternotomy/cystotomy/capitonnage for 1 patient with bilateral disease. We performed 1 lobectomy for parenchymal destruction due to abscess formation. Postoperatively, there were 2 major complications: 1 patent cavity and 1 empyema; minor complications included 3 cases of prolonged air leakage and 1 wound infection. In spite of the alternative therapeutic methods, we believe that the most effective approach to the cyst hydatid disease is surgery, which provides the least morbidity and the highest effectivity. Cystotomy and capitonnage are the most frequently performed procedures.
In this issue

{kind=link}
{kind=link}
{kind=link}
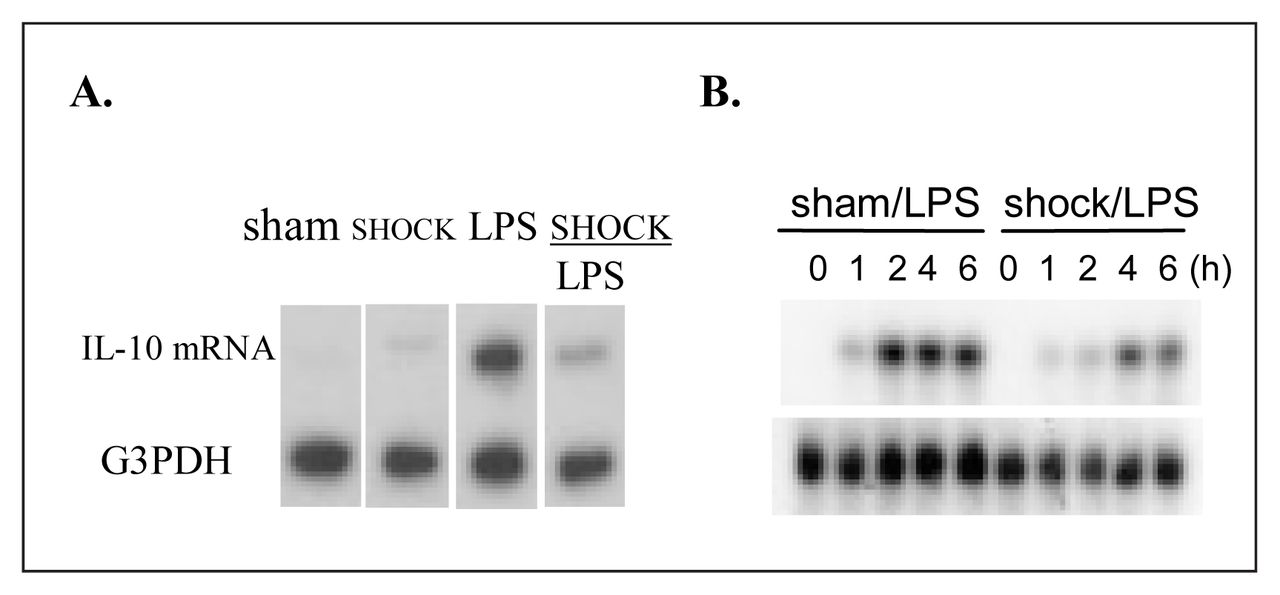{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.