


Abstract
Objectives: To compare the efficacy of combined oral and systemic antibiotics (combined) versus systemic antibiotics (systemic) alone in preventing surgical site infection in elective surgery of the colon, and to perform a meta-analysis of randomized studies comparing combined versus systemic antibiotics in elective colon surgery.
Design: A double-blind, placebo-controlled, randomized clinical trial.
Setting: The Queen Elizabeth Hospital, Montreal, a university-affiliated community hospital.
Participants: Two hundred and fifteen patients scheduled to undergo elective surgery of the colon.
Interventions: Patients were randomized to receive neomycin and metronidazole orally (109 patients) or identical placebos (106 patients) on the final preoperative day. All were given amikacin and metronidazole intravenously just before operation. Thirteen randomized series comparing combined and systemic antibiotic prophylaxis in elective colon surgery were identified for meta-analysis.
Outcome measures: Rates of postoperative surgical site infections: risk differences, risk ratios (RRs) and 95% confidence intervals (CIs); organisms found in the colon and wound fat at surgery, and in infected wounds.
Results: Three patients in the systemic group, and 5 in the combined group were excluded. Wound infections occurred in 5 patients in the combined group but in 17 in the systemic group (p < 0.01, RR = 0.29, 95% CI 0.11–0.75). Bacteria isolated from wound infections and wound fat were similar to those found in the colon. They were more frequent in the colon in the systemic group (p < 0.001) and occurred in wound fat in the systemic group twice as often as in the combined group (p < 0.001). By stepwise logistic regression, the presence of bacteria in wound fat at surgery was the strongest predictor of postoperative wound infection (p < 0.002). In the meta-analysis, the summary weighted risk difference in surgical site infections between groups (dw) and the summary RR both favoured combined prophylaxis (dw = 0.56, 95% CI 0.26–0.86; RR = 0.51, 95% CI 0.24–0.78; p < 0.001).
Conclusions: In elective surgery of the colon combined oral and systemic antibiotics are superior to systemic antibiotics in preventing surgical site infections. Orally administered antibiotics add value by reducing bacterial loading of the colon and wound fat contamination, both associated with postoperative wound infection. Meta-analysis of randomized clinical trials reported from 1975 to 1995 supports these conclusions.
The use of antibiotic prophylaxis in patients who undergo elective surgery of the colon is now accepted universally. Infections at the surgical site occur in 40% of patients not receiving antibiotic prophylaxis, but in only 5% to 15% of those receiving antibiotics. 1,2 Indeed, by 1983 Baum and associates3 had concluded that it was no longer justifiable to include placebo controls in trials of antibiotic prophylaxis in colon surgery. The best route for giving the antibiotics is still controversial. In the United States the trend favours a combination of oral and systemic administration. Condon and associates4 in their survey found that just over one-third of surgeons used the oral route for prophylaxis, half preferred combined oral and systemic routes, and only 8% used the systemic route alone. By 1990, 88% of 372 board-certified colon and rectal surgeons used both oral and systemic routes in preoperative preparation, and 3% used the oral route alone.5 In contrast, most surgeons in Europe and Asia now use systemically administered antibiotics only,6,7 and the recent withdrawal from the Canadian market of neomycin, the most commonly prescribed antibiotic for oral prophylaxis, indicates a similar trend in this country. We compared these 2 approaches — combined versus systemic antibiotic prophylaxis in elective colon surgery — to find out whether oral prophylaxis adds to the protection afforded by systemic prophylaxis, and if their topical mucosal effect in reducing the bacterial load of the colon is of value in decreasing the rate of postoperative surgical site infection. Our results support added value. Previous studies, some flawed, have examined this question with conflicting results. Therefore, we present a meta-analysis of randomized studies that, along with the present study, send a message from the 1990s.
Methods
From 1992 to 1995, all patients who underwent elective surgery of the colon at the Queen Elizabeth Hospital in Montreal were eligible to enter the study. Patients who were allergic to the study antibiotics or who had received antibiotics within the 2 weeks before operation, pregnant patients and those who refused informed consent were excluded.
One day preoperatively, routine blood tests were performed, and those patients who consented to the trial were enrolled, and randomized by the pharmacist in blocks of 4. The large bowel was prepared by mechanical washout with sodium phosphate given orally until the rectal effluent was clear. If not, saline enemas were given at 1800 on the day before operation until they were clear. At 1900 and 2300 the patients received neomycin, 2 g, and metronidazole, 2 g, orally (combined group) or an identical placebo (systemic group). On the day of surgery all patients were given amikacin, 1 g, and metronidazole, 1 g, intravenously on the way to the operating room.
During the operation specimens were taken for culture from the colon when it was opened and from the subcutaneous fat just before wound closure. On arrival in the recovery room a blood specimen was taken to determine the serum amikacin level, but the result was withheld from study personnel until the trial was completed. Serum concentrations of metronidazole were not determined. At the dose prescribed, mean concentrations of metronidazole in the blood are known to be several times those required for effective prophylaxis from colon anaerobic bacteria.8 No further antibiotics were given. The patients were followed up by the infection control nurse on postoperative days 3, 5 to 7, 10 to 14, and at 1 month for diagnosis of surgical site infection, using the modified CDC criteria. 9 Postoperative bowel movements were noted, and diarrhea was assessed as 3 or more loose stools per day for 48 hours.10,11
Risk ratios (RRs) and χ2 analysis were used for categoric data, the t-test was used for continuous variables, and stepwise logistic regression was used to analyze variables associated with postoperative wound infection. Statistical calculations were done with use of the SPSS computer software. The sample size was calculated assuming an infection rate at the surgical site of 10% to 15%, and a treatment difference of 10% (α risk 0.05, β risk 0.20). The trial was concluded prematurely when unforeseen closure of the hospital was planned, and a preliminary analysis showed a positive result. A meta-analysis was performed of randomized clinical trials reported in the previous 20 years, comparing systemic and combined antibiotic prophylaxis in elective surgery of the colon.12 These studies were identified by a MEDLINE search and by manual search of associated bibliographies. For each study a quality score was calculated by the method of Jadad and associates.13 This assessment takes into account the description and appropriateness of randomization, blinding and withdrawals. A perfect score is 5 points; a point is deducted for each error of blinding or randomization. For each study, a risk difference (RD), RR and 95% CI were calculated,12,14,15 and unweighted mean summary indices were then derived by pooling results. To compensate for variability in study size, a weighted RD for each study was calculated as described by Ingelfinger and colleagues,14 and a summary weighted mean RD and 95% CI were derived.
Results
Two hundred and fifteen patients were enrolled (109 in the combined group and 106 in the systemic group). Three patients were with-drawn from the systemic group and 4 from the combined group because the operation was postponed or the colon was not opened; 1 patient who received combined prophylaxis died within 48 hours of surgery. No infection was noted postoperatively in these patients.
The treatment groups were evenly matched with respect to age, gender, body mass index and preoperative serum albumin level and blood lymphocyte count (Table 1). There were no significant differences between the groups with respect to the preoperative final diagnoses and operations performed (Table 2). Wound infections (RR = 0.29, 95% CI 0.11–0.75, p < 0.01) and total surgical site infections (RR = 0.24, 95% CI 0.9–0.62, p < 0.002) were significantly fewer in the combined than the systemic group (Fig. 1). The frequency of anastomotic leaks and intra-abdominal abscesses was similar in the 2 groups. Table 3 shows that bacteria in the subcutaneous fat at operation and in infected wounds were typical of colon flora and that there were fewer in the combined than the systemic group; and Fig. 2 emphasizes the association between bacteria found in the subcutaneous fat at surgery, and subsequent wound infection (RR = 0.49, 95% CI 0.39–0.61, p < 0.001). Fig. 3 shows the number of bacterial isolates in the colon in the 2 groups. Both aerobic and anaerobic bacterial isolates from the colon were found more frequently in the systemic group. Bacteria were also found twice as often in the subcutaneous fat in the systemic group as in the combined group (RR = 0.46, 95% CI 0.33–0.65, p < 0.001) (Fig. 4). The mean (and standard error of the mean) postoperative serum concentration of amikacin was almost identical in the 2 treatment groups (Table 1). By stepwise logistic regression only positive intraoperative fat culture (p < 0.002) and antibiotic (p < 0.03) were related to wound infection. Colon culture, patient age and weight, duration of surgery, and the presence of other diagnoses such as diabetes, metastatic disease and steroid therapy were not. Eight of 104 patients in the systemic group and 5 of 106 in the combined group had diarrhea postoperatively (p = 0.39). The mean (and SEM) number of stools per day in the first postoperative week was 0.52 (0.59) in the systemic group, and 0.39 (0.44) in the combined group (p = 0.07).

The frequency of wound infections, anastomotic leaks and intra-abdominal abscesses in patients who received antibiotic prophylaxis by the systemic route only (systemic, black bars) and by both the oral and systemic routes (combined, white bars).

A positive result from culture of the subcutaneous fat at operation in patients who underwent colon surgery increases the likelihood of wound infection (~ 2% for negative fat culture v. ~ 20% for positive fat culture). Black segments = wound infection, shaded segments = no wound infection.

Isolates of aerobic and anaerobic bacteria in cultures taken from the colon at the time of surgery were twice as frequent in patients who received systemic prophylaxis only as in those who received combined oral and systemic prophylaxis.

A positive culture of the subcutaneous fat at the time of colon surgery was twice as common in patients who received antibiotic prophylaxis by the systemic route only as in patients who received prophylaxis by the combined oral and systemic routes. Black segments = culture negative for bacteria, shaded segments = culture positive for bacteria.
Comparison of Demographics and Serum Measurements in Patients Who Received Antibiotic Prophylaxis by Two Different Routes Before Undergoing Colon Surgery*
Preoperative Diagnosis and Procedure Performed in Patients Who Received Antibiotic Prophylaxis by Two Different Routes Before Undergoing Colon Surgery
Organisms Found in the Wound and Fat of Patients Who Received Antibiotic Prophylaxis by Two Different Routes Before Undergoing Colon Surgery*
Table 4 and Fig. 516–27 summarize RRs and CIs obtained by meta-analysis of randomized series published between 1979 and 1995 comparing systemic versus combined oral and systemic prophylaxis in colon surgery. The overall trend clearly favours combined antibiotic prophylaxis. The unweighted mean RD in the rate of wound infections was 0.69 (95% CI 0.39–0.99), and the weighted mean RD in the rate of wound infections was 0.56 (95% CI 0.26–0.86) (p < 0.01).
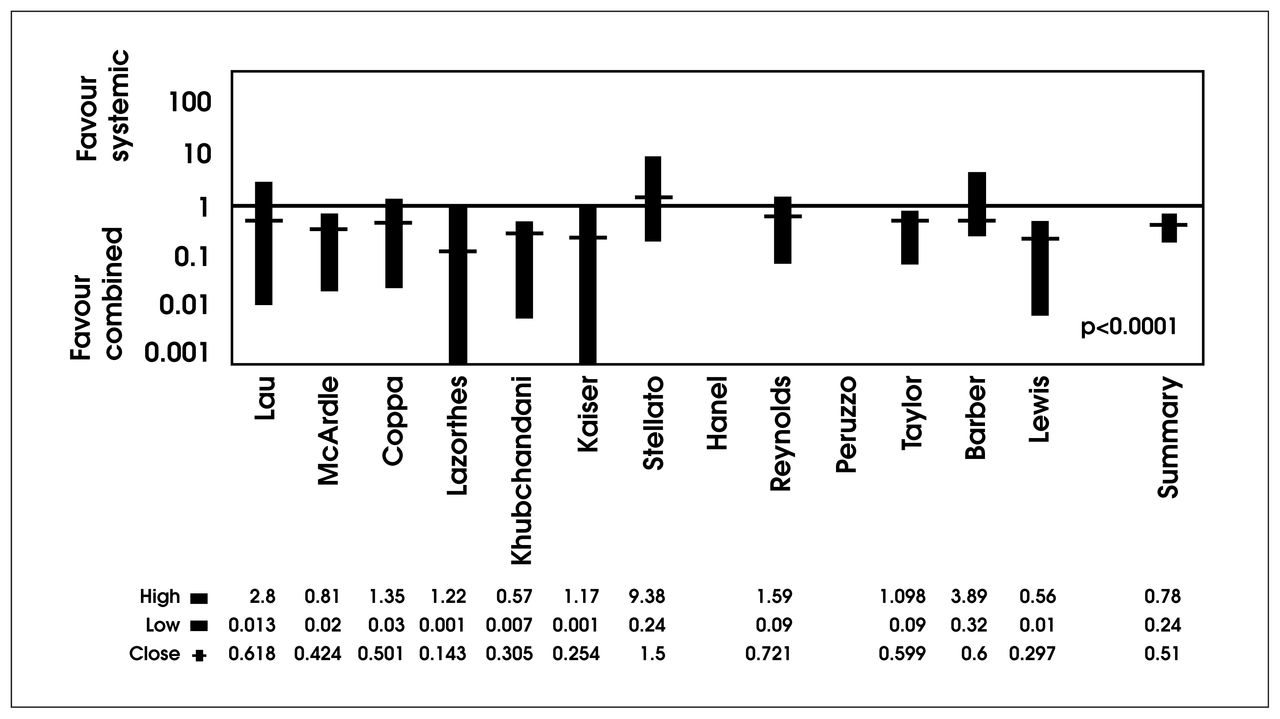
Individual study and summary risk ratios and 95% confidence intervals in the meta-analysis of randomized clinical trials reported between 1979 and 1995 comparing systemic and combined antibiotic prophylaxis in colon surgery.
Meta-Analysis of Randomized Series Published Between 1975 and 1995 Comparing Systemic Versus Combined Antibiotic Prophylaxis in Colon Surgery
Discussion
It is clear that antibiotic prophylaxis is required in elective surgery of the colon, but should the route of administration be systemic, oral, or both? This study shows the benefit of combined oral and systemic administration over systemic administration alone, and meta-analysis of randomized series reported over the last 20 years supports this view.
At first, oral antiseptics and antibiotics were advocated to reduce the risk of postoperative wound infection by decreasing the number of bacteria in the colon.28–31 Then perioperative parenteral prophylaxis, proposed by Miles and colleagues32 and Burke,33 was used widely following Polk’s landmark clinical study1 in 1969. Evaluation of these 2 routes of antibiotic administration has been complicated by such confounding issues as the spectrum of antibiotic coverage and the significance of pharmacodynamics of the antibiotics. But subsequent studies have shown that anaerobic bacteria are the preeminent cause of wound infection34,35 and that the 2 routes are equally effective when drug pharmacodynamics are adequate.36 One study,37 much criticized for its methodology did, however, confirm that adequate concentrations of antibiotic in blood and tissue are essential to prevent infection: effective topical enteral sterilization without adequate blood levels of antibiotics was associated with a 32% rate of wound infection; but this rate was only 6% with systemic antibiotics that attained high blood concentrations but failed to sterilize the bowel. In another study38 oral antibiotics that sterilized the bowel and attained adequate blood concentrations provided prophylaxis equal to that of systemic antibiotics.
In our study, we were careful to eliminate these confounding issues by including aerobic and anaerobic coverage in both arms of the study, and by ensuring that systemic antibiotic concentrations were adequate for prophylaxis throughout the surgical procedure. The mean (and SEM) postoperative serum concentration of amikacin was 32.38 (11.66) mg/mL, well above the minimal inhibitory concentration of amikacin for the usual surgical pathogens — below 16 mg/mL.2 In addition, the randomization was performed in small blocks to ensure even distribution of patients — and this was attained. Although the patients were not stratified for special risk factors such as low pelvic anastomosis, the randomization produced evenly matched groups (Table 2). Anastomotic leaks were equally infrequent in the study groups. Orally administered antibiotics protect against anastomotic leak when the bowel is ischemic, 39 but no special protection would be expected in the absence of bowel ischemia.
Wound infections and total surgical site infections were both lower in the group receiving combined prophylaxis. The RR of 0.29 implies that the combination of oral and systemically administered antibiotics prevents 1 wound infection for every 9 patients receiving antibiotics by the systemic route alone. Obviously, this is an advantage of clinical significance. Besides, this benefit was attained without a measurable additional risk. Postoperative diarrhea was no more common in patients in the combined group than those in the systemic group.40,41 Assays for Clostridium difficile toxin were obtained in patients with diarrhea but were not part of the study protocol. Furthermore, combined prophylaxis confers a clear fiscal advantage. In the dosages given, oral neomycin and metronidazole cost less than Can$20. So we can estimate that an outlay of less than Can$500 for 9 to 10 patients would result in a saving of the Can$2000 to Can$4000 of excess direct costs of a major surgical site infection.42,43 These findings render inexplicable the current trend in Canada toward the use of antibiotic prophylaxis by the systemic route alone. Orally administered neomycin base is now no longer generally available having been with-drawn recently because of a limited market. As indicated below, neomycin may not be necessary; but this study sends a message from the 1990s that would discredit the trend to using systemic prophylaxis alone.
The rationale for added value from the use of antibiotics by the oral route also follows from our results. A clear association was observed between wound infection and positive results of culture of the subcutaneous fat at the end of the operative procedure; and this finding was supported by stepwise logistic regression of factors causing wound infection. We also noted an association between positive results of culture of the subcutaneous fat and of the open colon at surgery; the mean number of aerobic and anaerobic bacterial isolates in the colon was significantly lower in the patients in the combined group. Clearly, orally administered antibiotics provided added value by their topical sterilizing effect. Of the oral antibiotics used, metronidazole offers well-established advantages.44 Although parenterally administered metronidazole enters the bowel through the enterohepatic circulation, the resulting reduction in colon bacteria is significantly less than occurs after oral administration of metronidazole.38 The difference may be due partly to the timing of parenteral dosing in relation to the sampling of colon content; in addition, the hydroxymetabolite that enters the bowel has only 65% the bactericidal activity of metronidazole.8 Our data confirm that orally administered metronidazole is far more effective than parenterally administered metronidazole in eliminating bacteria from the colon and in reducing the risk of contamination of wound fat. In contrast, nonabsorbable oral antibiotics effective against intestinal aerobic bacteria offer no clear benefit. No advantage was found in a review of over 500 patients in 4 randomized series (RR = 1.53, 95% CI 2.22–1.06, p = 0.15).44 So neomycin given orally may not be necessary;45 but this does not negate the value of the oral route.
Finally, our meta-analysis of almost 2000 patients in randomized studies lends credibility to our study results. The process employed the best methods of search, selection, summarizing and statistical analysis,46 and the results confirm the clinical and statistical value of combined prophylaxis. In elective surgery of the colon combined antibiotics given by the oral and systemic routes are superior to antibiotics given by the systemic route alone in preventing surgical site infections.
Acknowledgements
This study would not have been possible without the cooperation of my surgical colleagues of the now defunct Queen Elizabeth Hospital of Montreal. The consistent, keen and able assistance of the nurses on the surgical ward and in the operating suite was instrumental in the smooth conduct of the trial; and the tireless efforts of the Infection Control Nurse were indispensable to the complete follow-up of wounds.
- Accepted May 14, 2001.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools





