


Abstract
Objective: To investigate quantitative differences in vertebral scalloping between children who have scoliosis with and without neurofibromatosis type 1 (NF1).
Design: A retrospective study.
Setting: A university-affiliated children’s hospital.
Patients: Twenty-seven children with scoliosis, 13 of whom had NF1 and 14 of whom did not.
Method: Existing radiographs of the lumbar vertebrae were used to measure and compare the degree of vertebral scalloping.
Main outcome measures: The distribution of posterior scalloping ratios in the 2 groups and the most extreme ratio in each subject in each group were compared.
Results: Scalloping ratios from the children with NF1 were not normally distributed: 31% had ratios greater than 1.20. Scalloping ratios from the non-NF1 children were normally distributed, with a mean ratio (and standard deviation) of 1.13 (0.03). The distribution between the 2 groups was significantly different (p < 0.05).
Conclusions: In children who have scoliosis but no NF1 there was a range of mild scalloping whereas those with NF1 has severe scalloping. Further studies are needed to determine the possible role of vertebral scalloping in scoliosis severity and progression in children who have NF1.
Neurofibromatosis type 1 (NF1) is a disease with autosomal dominant genetic inheritance and a prevalence in childhood of about 1 in 3000. The responsible gene, NF1, has been identified and mapped to the long arm of chromosome 17.1–4 NF1 is extremely variable clinically, but characteristic features include peripheral neurofibromas, café-au-lait macules and Lisch nodules.5
NF1 produces skeletal abnormalities in a large proportion of affected patients. Scoliosis is the most common skeletal manifestation of NF1, with an estimated rate of 10% to 60% in various studies,4,6 generally seen in the form of a single curve involving 4 to 6 thoracic vertebrae,6 but there is great variation in the type and severity of spinal curvature. Many NF1 patients with scoliosis have associated features (generally called dystrophic features) like vertebral scalloping, rib pencilling, a paravertebral soft-tissue mass or defective pedicles.7,8 Scoliosis in NF1 is, therefore, classified into 2 main types: with and without associated dystrophic features.6,9
Vertebral scalloping refers to an exaggerated concavity of the dorsal surface of a vertebra,10 although there is currently no accepted definition that clearly distinguishes between vertebral scalloping and the normal slight concavity of healthy vertebral bodies. Scalloping of the vertebrae occurs at an extremely young age in NF1. Funasaki and associates6 reported that of 65 NF1 patients with scoliosis, 31 had scalloping that was apparent by the age of 10 years. Eleven of these children were followed up for an average of 14 years each, and no new vertebral scalloping was noted after the age of 10 years. According to Casselman and Mandell,7 posterior scalloping is a more characteristic finding than anterior or lateral scalloping among NF1 patients.
The cause of vertebral scalloping in NF1 has not been determined and may differ from case to case.8 Dural ectasia, an increase in the thickness of the thecal sac, can cause expansive and erosive deformities to adjacent vertebral bodies.9 Scalloping may also be caused by erosion from nearby neurofibromas or even by primary mesodermal dysplasia of meninges. Finally, abnormal development of the vertebral tissues (i.e., true vertebral dysplasia) may also give rise to scalloping. Vertebral scalloping may be seen in patients with dysplastic scoliosis, such as that seen secondary to Marfan’s syndrome.
The goal of this study was to characterize vertebral scalloping quantitatively in NF1 and non-NF1 patients with scoliosis, and to identify any differences between the 2 populations.
Methods
Sample population
We reviewed the anteroposterior and lateral spinal radiographs from 27 children with scoliosis seen in the Scoliosis Clinic at British Columbia’s Children’s Hospital. Of these children, 13 had NF1 and scoliosis, and 14 had idiopathic scoliosis but no NF1. The children with NF1 ranged in age from 3 to 18 years and had primary curves ranging from 36° to 75° (average 52.7°). The non-NF1 group, identified through the clinic database, ranged in age from 7 to 17 years old at examination and had primary curves ranging from 30° to 90° (average 51.0°).
Measuring scalloping
Vertebral scalloping was measured from lateral radiographs of the lumbar spine only. The lateral films were scanned into a personal computer and stored as digital images. Measurements were obtained using a digital measurement tool in Adobe Photoshop 5.5. This method allowed better visualization and enhanced accuracy and reliability. All measurements were performed blindly by the first author (E.S.H.K.). Vertebral scalloping was estimated as a ratio, using a modification of the procedure described in the study of Funasaki and associates.6 Three width measurements were obtained for each individual vertebral body: superior, inferior and waist (Fig. 1). The average of the superior and inferior measurements was divided by the waist measurement to obtain a “scalloping ratio.” A ratio of 1.0 indicated no scalloping (no indentation in either the anterior or posterior edge). A ratio greater than 1.0 indicated scalloping, and the larger the ratio the more severe was the vertebral scalloping.

An example of vertebral scalloping and a diagram showing where measurements were taken on lateral films of lumbar vertebral bodies.
Data analysis
An individual patient may have more than 1 scalloped vertebral body, but we used only the largest scalloping ratio from each child for analysis to maintain the statistical independence of each case. For children who had more than one set of radiographs at different ages, ratios were obtained from all the sets, and the largest scalloping ratio measured was used in the analysis. The distribution of maximum scalloping ratios in each group was tested for normality with a Shapiro–Wilks test. The distributions of maximum scalloping ratios in the NF1 and non-NF1 groups were compared by the Mann–Witney U test. Comparisons with p < 0.05 were considered to be statistically significant.
Results
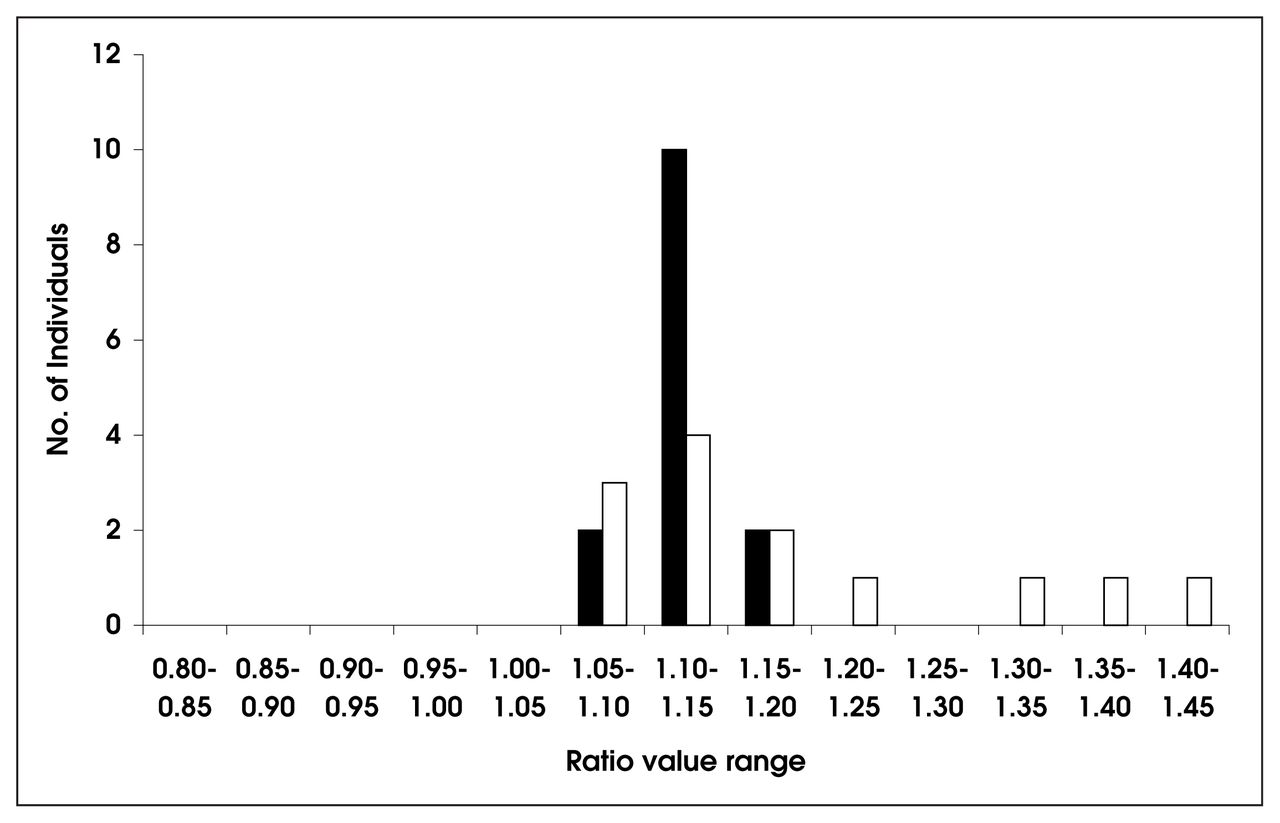
The mean (and standard deviation) for the maximum scalloping ratio in the NF1 children was 1.18 (0.13). For the children without NF1, the mean was 1.13 (0.026). The much greater variability of values in the NF1 group is also seen in Fig. 2, which shows the frequency distribution of values for the largest scalloping ratio obtained in each child. The distributions of maximum scalloping ratios for the 2 groups are clearly different. In children without NF1the distribution did not differ significantly from normal (p = 0.62), whereas among children with NF1 the distribution differed significantly (p = 0.02). None of the non-NF1 children in this sample had maximum scalloping ratios above 1.21 (3 SDs above mean of the normal distribution), whereas 4 out of the 13 children with NF1 did. On the basis of the normal distribution observed for non-NF1 cases, we estimated the probability that a randomly-chosen non-NF1 patient with scoliosis had a lumbar scalloping ratio greater than 1.21 to be 0.0028. The distributions for the maximum scalloping ratios did not differ significantly (p = 0.61) between these small groups.

The distributions of the maximum vertebral scalloping ratio obtained from each patient from both NF1 (black bars) and non-NF1 (white bars) population samples of children with scoliosis.
Discussion
This study showed there was a group of patients with NF1 who had significant vertebral lumbar scalloping. This evidence is promising for developing diagnostic criteria in young patients who present with only a few of the clinical criteria for NF1. As we observed, the scalloping is not confined to older patients. Conclusive diagnostic criteria could be made with a larger population sample across more ethnic groups with a multicentre study.
The method of measuring the images digitally enhanced the visualization accuracy; however, the images were still 2-dimensional. The superior, waist and inferior vertebral measurements varied considerably depending on the 3-dimensional orientation of the patient and individual vertebrae in the radiograph. Without 3-dimensional imaging, this problem was difficult to overcome. Three-dimensional computed tomography scans may be the most accurate method of assessing vertebral scalloping. However, this technique is costly and exposes the patient to increased radiation.
Another limitation of the study was that we only measured the lumbar vertebrae. Salerno and Edeiken8 suggested that scalloping of vertebral bodies is most frequent on the posterior surface. Posterior vertebral scalloping was best visualized on lateral radiographs as a concave indentation of the posterior margin of a vertebral body toward the centre.7 We used measurements from lumbar vertebrae for this study because they provided the best quality images of large vertebral bodies that were free of overlap from the ribs. However, we know that vertebral scalloping in NF1 patients is often focal,7,8,10 so some patients who do not have vertebral scalloping in the lumbar region may have it elsewhere in the spine. Further study of scalloping in other sections of the spine is needed to determine how representative our findings are for the whole vertebral column.
Funasaki and associates6 used a single measurement for each vertebral body to determine the presence or absence of scalloping. They measured the distance from the posterior limit to the deepest anterior point of the posterior margin and diagnosed scalloping if this value was greater than 4 mm in a lumbar vertebra. This method did not account for differences that occur in the sizes of vertebral bodies from different patients, in children of different ages or in different regions of the spine. We used a ratio of vertebral measurements in this study to allow vertebrae of different sizes to be compared directly.
The maximum scalloping ratios in lumbar vertebrae of children with scoliosis who did not have NF1 were normally distributed, but this was not true for children with scoliosis who had NF1 (Fig. 2). Vertebral scalloping, defined as a scalloping ratio more than 3 standard deviations above the mean for the non-NF1 group with scoliosis, was seen in the lumbar vertebrae of 4 of the 13 NF1 children studied. The distribution of scalloping ratios in other 9 children was similar to that in patients without NF1, so we conclude that there were 2 classes of NF1 patients with scoliosis — those with and those without vertebral scalloping. This conclusion is consistent with clinical experience6,9 but cannot be made only on the basis of the current study, in which we examined vertebral bodies of just the lumbar spine.
The pathogenesis of vertebral scalloping in NF1 is unknown. A recent study by Durrani and associates11 suggests that “dystrophic” features may be correlated with clinical progression of a spinal deformity, but no independent effect was shown for vertebral scalloping.
Conclusions
Our study indicated there may be a subset of children who had NF1 associated with scoliosis who had increased lumbar vertebral scalloping. However, long-term longitudinal studies of vertebral scalloping measured quantitatively in NF1 patients are required to determine whether scalloping is progressive as well as to clarify its relationship, if any, to the severity and progression of scoliosis.
Acknowledgements
This work was supported by the British Columbia Neurofibromatosis Foundation and theGizeh Shrine, Vancouver, BC.
- Accepted June 21, 2001.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.