


The keys to successful treatment of tracheal tears after endotracheal intubation are early recognition, control of airway, antibiotic therapy and surgical repair. Surgical approaches to the repair of iatrogenic membranous tracheal injuries depend on the extent and location of the tear. Tears of the upper two-thirds can usually be repaired through a cervical incision. Lower tracheal or juxtacarinal tears can be approached through a right thoracotomy. Exposure for total or near-total membranous tears may be best obtained by median sternotomy and collar incision, with the repair performed through a longitudinal anterior tracheal incision. We have used this novel approach to such an extensive tear with success.
Case report
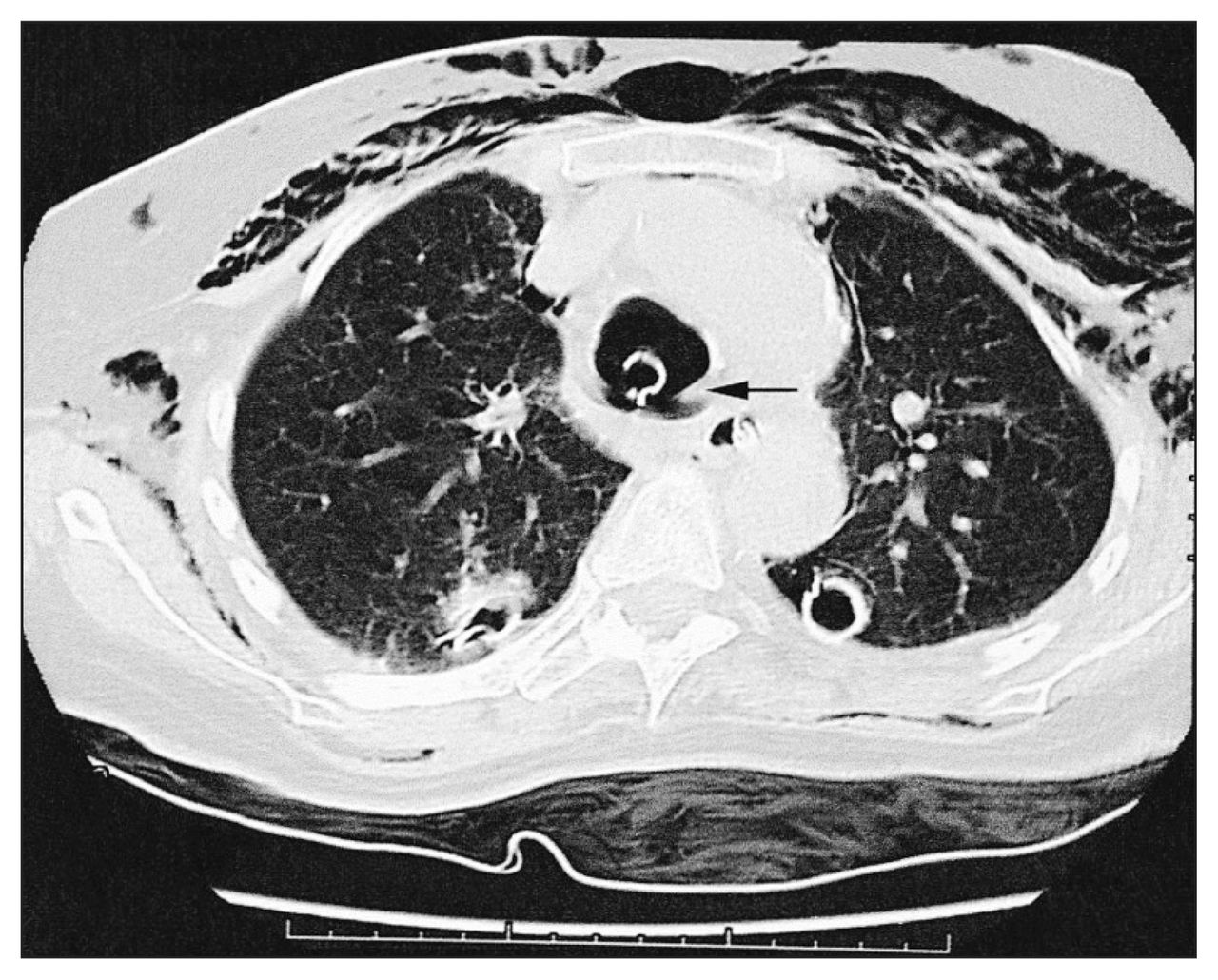
A 66-year-old woman who had previously suffered a stroke had a myocardial infarction, seizure and respiratory arrest at a nursing home. Urgent care was obtained at a community hospital, where she was intubated with an 8-mm diameter endotracheal tube. The next day, she had subcutaneous emphysema and bilateral pneumothoraces requiring tube thoracostomies, thought to be the result of ventilator-induced barotrauma. An attempt at extubation 4 days later failed as she immediately had stridor and dyspnea. She was reintubated orally, with an 8-mm diameter endotracheal tube. Postintubation chest radiography (Fig. 1) and computed tomography (Fig. 2) suggested tracheal rupture. The patient remained hemodynamically stable, and there were no problems with respect to oxygenation or ventilation. Antibiotics were begun, and the patient was transferred to the thoracic surgical service.

Chest radiograph showing subcutaneous emphysema, bilateral chest tubes for pneumothoraces and the endotracheal tube with an overinflated balloon cuff (arrow).
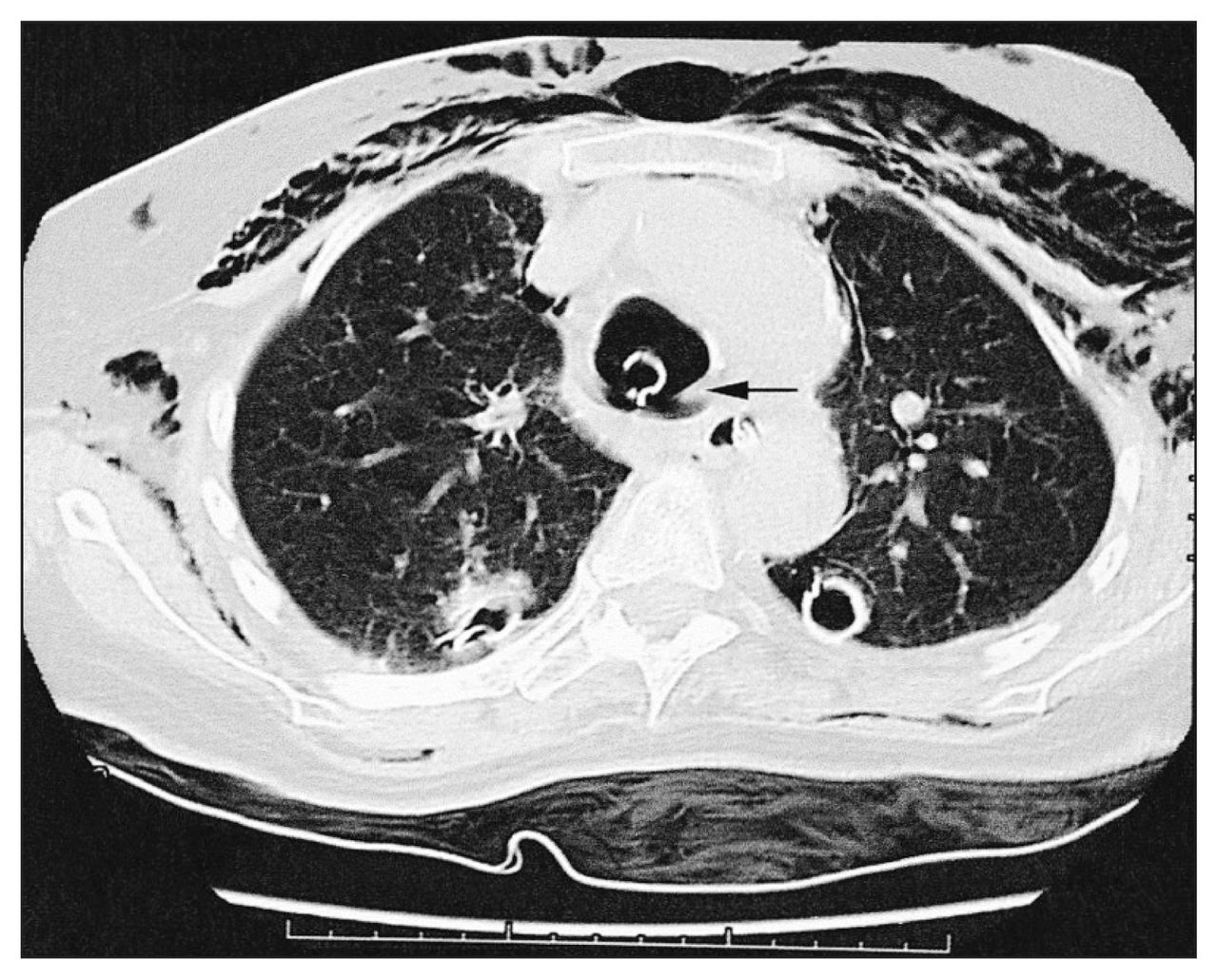
Computed tomography scan showing a dilated trachea from an overinflated endotracheal balloon cuff with an adjacent membranous tracheal tear (arrow).
Fibreoptic bronchoscopy revealed a 9-cm near-total longitudinal membranous tear of the trachea, beginning 1.5 cm below the vocal cords and extending to just above the carina. Esophagoscopy revealed normal esophageal mucosa.
Surgical technique
With the patient in the supine position a combined median sternotomy and cervical incision was performed. Blood flow through the innominate artery and left innominate vein was controlled with vessel loops. Exposure of the entire trachea was obtained in 2 steps. First, the upper two-thirds was exposed by dividing the thyroid isthmus and retracting the innominate vessels in a caudad direction. Second, exposure of the distal third was accomplished transpericardially. The anterior pericardium was incised and, with the superior vena cava retracted to the right and the aorta to the left, the posterior pericardium was opened. With the right main pulmonary artery retracted caudad and the innominate vessels cephalad, the distal third of the trachea, carina and both main-stem bronchi were clearly exposed.
The anterior tracheal rings of the distal third of the trachea were incised longitudinally, stopping 1 cm above the carina. Satisfactory airway control was best obtained by cross-field dual lung ventilation with 5-mm armoured endotracheal tubes placed directly into each main-stem bronchus. The anterior longitudinal tracheal incision was then extended cephalad to the level of the third tracheal ring. The full extent of the posterior membranous tear was now clearly visible. The tear extended 9 cm from the second tracheal ring to just above carina. The edges were healthy, and there was no evidence of infection. Interrupted 3–0 polydioxanone sutures (PDSs) (Ethicon, Somerville, NJ) were used to provide primary repair in 2 steps: the distal third followed by the proximal two-thirds, adjusting tracheal exposure for each step as described for the anterior tracheal incision. A 36-French Maloney bougie was passed down the esophagus to prevent injury during the tracheal repair. The anterior tracheal incision was then closed with interrupted 3–0 PDSs, again in 2 steps. First, the armoured endotracheal tubes were removed, and under apnea oxygenation the lower third was closed, allowing passage of a 7-mm oral endotracheal tube into the distal trachea for conventional dual lung ventilation. Second, the remaining upper two-thirds of the anterior tracheal incision was closed. A pericardial flap was then interposed between the trachea and innominate artery.
Postoperative course
Bronchoscopy performed on postoperative day 14 revealed intact anterior and posterior tracheal suture lines and a somewhat narrowed but adequate tracheal lumen. There was prolonged neurologic recovery and pneumonia, which necessitated operative insertion of a 6-mm tracheostomy tube on postoperative day 33. Four days later, the patient was weaned from the ventilator and transferred to the ward. Because of the patient’s slow neurologic recovery, the tracheostomy was not removed until 110 days after operative insertion. The patient remains well and without airway difficulty 13 months postoperatively.
Comment
Tracheal tear is a rare complication of endotracheal intubation.1 Prompt recognition is important. Bronchoscopy is essential not only for diagnosis but also for assessing the location and extent of the tear. This allows the surgeon to choose an operative approach. Collaboration with the anesthesiologist for airway control before, during and after operative repair is essential.
Tears less than 4 cm long in a stable, spontaneously breathing patient may be managed with observation and antibiotics,1–3 otherwise early operative repair is mandatory. For tears of the upper two-thirds of the trachea, a cervical incision is used.3–5 Distal third or juxtacarinal tears are approached through a high right thoracotomy. 1,3,6 Combined cervical incision and right thoracotomy has been described for successful repair of long total or near-total membranous tracheal tears.6 We used an anterior approach of combined median sternotomy with collar incision and repair through an anterior tracheal incision.
Repairs of smaller membranous tracheal tears through cervical and anterior tracheal incisions have been reported,3–5 but no patient had a tear longer than 5 cm with extension down to the carina, thus allowing exposure solely through a cervical incision. In our patient, because of the length and juxtacarinal location, an additional median sternotomy and transpericardial exposure of the distal trachea and carina were required.
The advantages of the anterior approach for repair of long tracheal tears include the following:
Excellent exposure of the entire trachea through a single continuous incision. Superior exposure of the upper two-thirds of the trachea is well known, but the anterior approach also provides excellent exposure to the lower third of the trachea, similar to that used in transpericardial approaches for carinal resections7 or management of post-pneumonectomy bronchial fistulas.8
Various double lung ventilation strategies can be quickly and easily employed should single lung ventilation fail.
Lateral dissection and circumferential mobilization of the trachea are avoided so as to preserve tracheal circulation and recurrent laryngeal nerve function.
We did not notice the potential disadvantage of significant tracheal narrowing from 2 longitudinal suture lines and this has not been reported by others.3,5 Also, we did not find it necessary to extend the anterior tracheotomy above the third tracheal ring to repair the high proximal aspect of the membranous tear. This retained the option of future tracheostomy placement above the anterior tracheal suture line. We believe that an anterior approach should be considered in the management of long iatrogenic membranous tracheal tears.
- Accepted May 29, 2001.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.