


A 23-year-old man presented with a 6-month history of progressive lower back pain. Three months earlier, the pain had started radiating into his legs, with numbness in the perineal area. Constitutional symptoms included night pain and a 9.1-kg weight loss over 6 months. Shortly before he presented to the orthopedic clinic he noted some difficulty initiating urination. He had been treated for mechanical back pain by 3 physicians.
On physical examination, the patient walked with an antalgic gait, favouring the right side. He had moderate discomfort to direct palpation over the right sacroiliac joint with no mass in the area. Lateral compression of the pelvis or external rotation of his hip aggravated his discomfort. Flexion, extension and rotation of the spine or leg were limited by pain in the same area.
On neurologic examination there was weakness in dorsiflexion and plantar flexion of the right ankle. Also, the right extensor hallucis longus muscle was weak. Sensation was decreased over the L5, S1, S2 and S3 distribution. The ankle reflex was absent, but muscle tone was normal. His anal tone and bulbocavernosus reflex were preserved. The left side was neurologically intact.
Radiographs of the area had been read as normal at an outside institution (Fig. 1). Close inspection revealed loss of definition of the anterior cortex of the sacrum on the lateral view. Urgent CT and MRI were carried out (Fig. 2, Fig. 3). CT revealed complete destruction of bony architecture on the right sacral ala and of the body of S1. The soft-tissue component of the lesion was better appreciated on MRI, where complete invasion of the spinal canal was seen. The lesion extended anteriorly into the pelvis.

Initial anteroposterior and lateral radiographs read as “normal.”
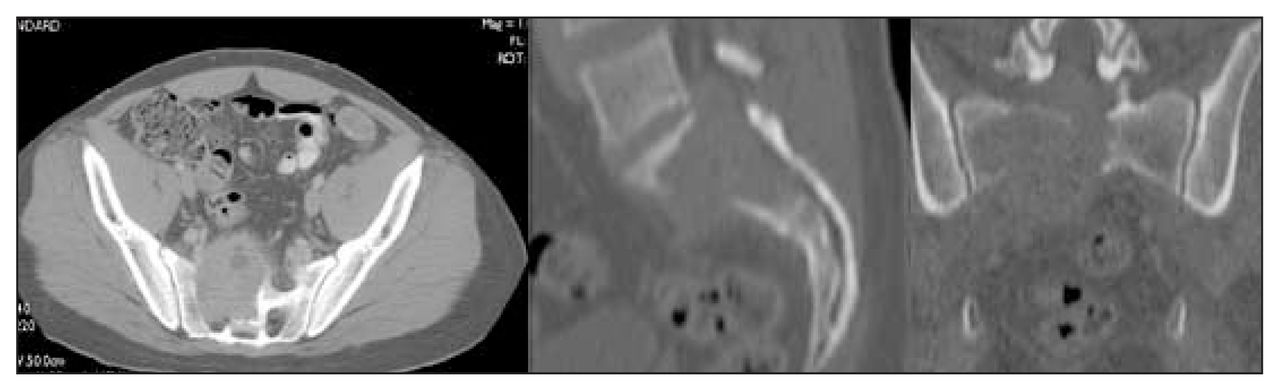
CT shows destruction of bony architecture of the right sacral ala and body of S1.

MRI shows invasion of the lesion into the spinal canal.
Biopsy of the lesion revealed a giant cell tumour. Microscopic examination showed inconspicuous stromal cells with mitotic activity, with abundant multinucleated giant cells along with invasion of bone into surrounding soft tissue (Fig. 4). Histologic grade was 1 of 3 (according to Jaffe).

Biopsy specimen showing many multinucleated giant cells (hematoxylin–eosin, original magnification ×200).
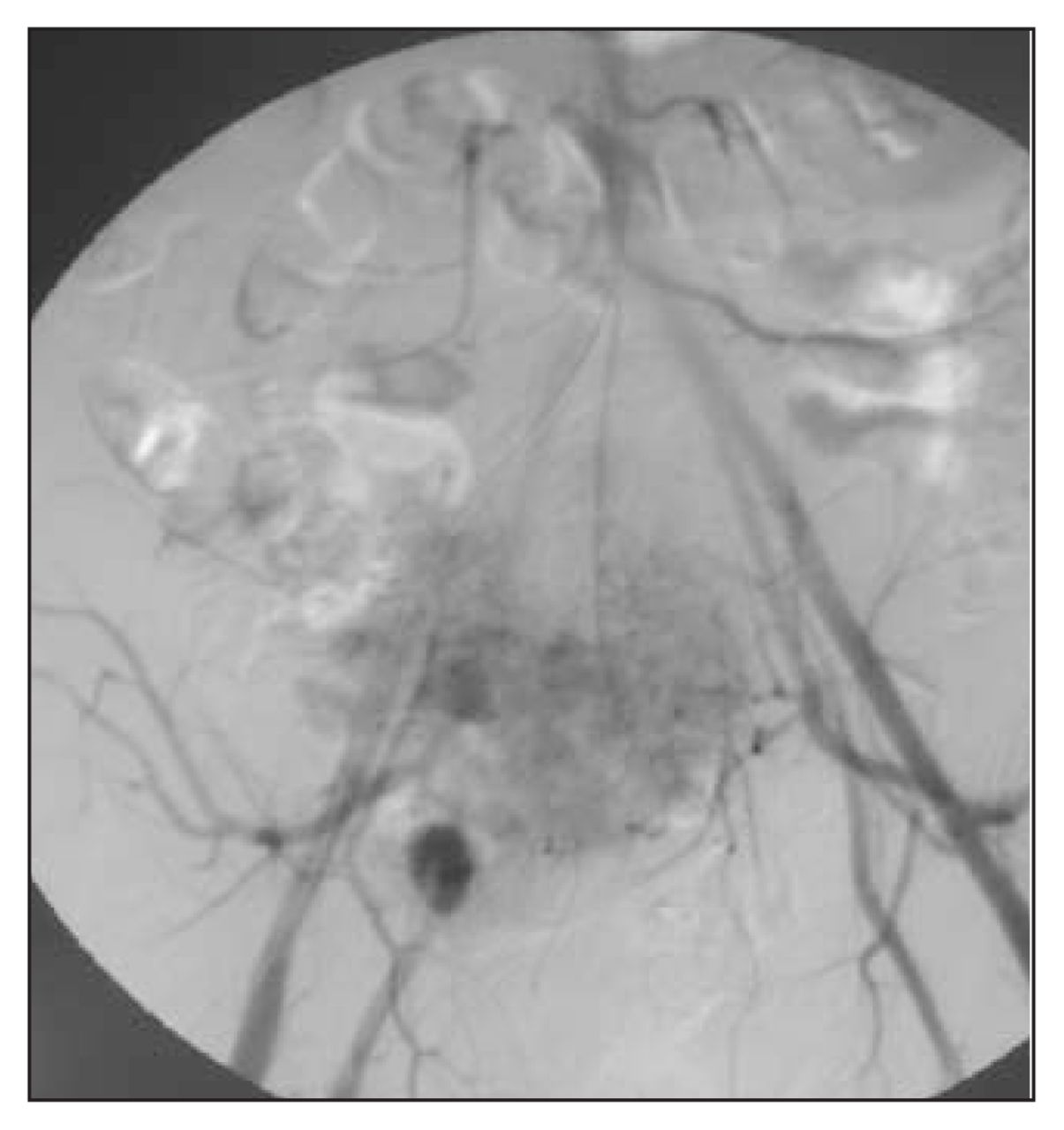
Because of the vascularity of giant cell tumours, embolization was performed preoperatively. Angiography (Fig. 5) confirmed the vascular nature of the lesion. A hemisacrectomy was performed through a posterior approach. The pelvis was stabilized with pedicle screws into L4 and L5, which were connected to screws placed into the iliac wings. A fibular autograft was used to bridge the defect left by the resection (Fig. 6).
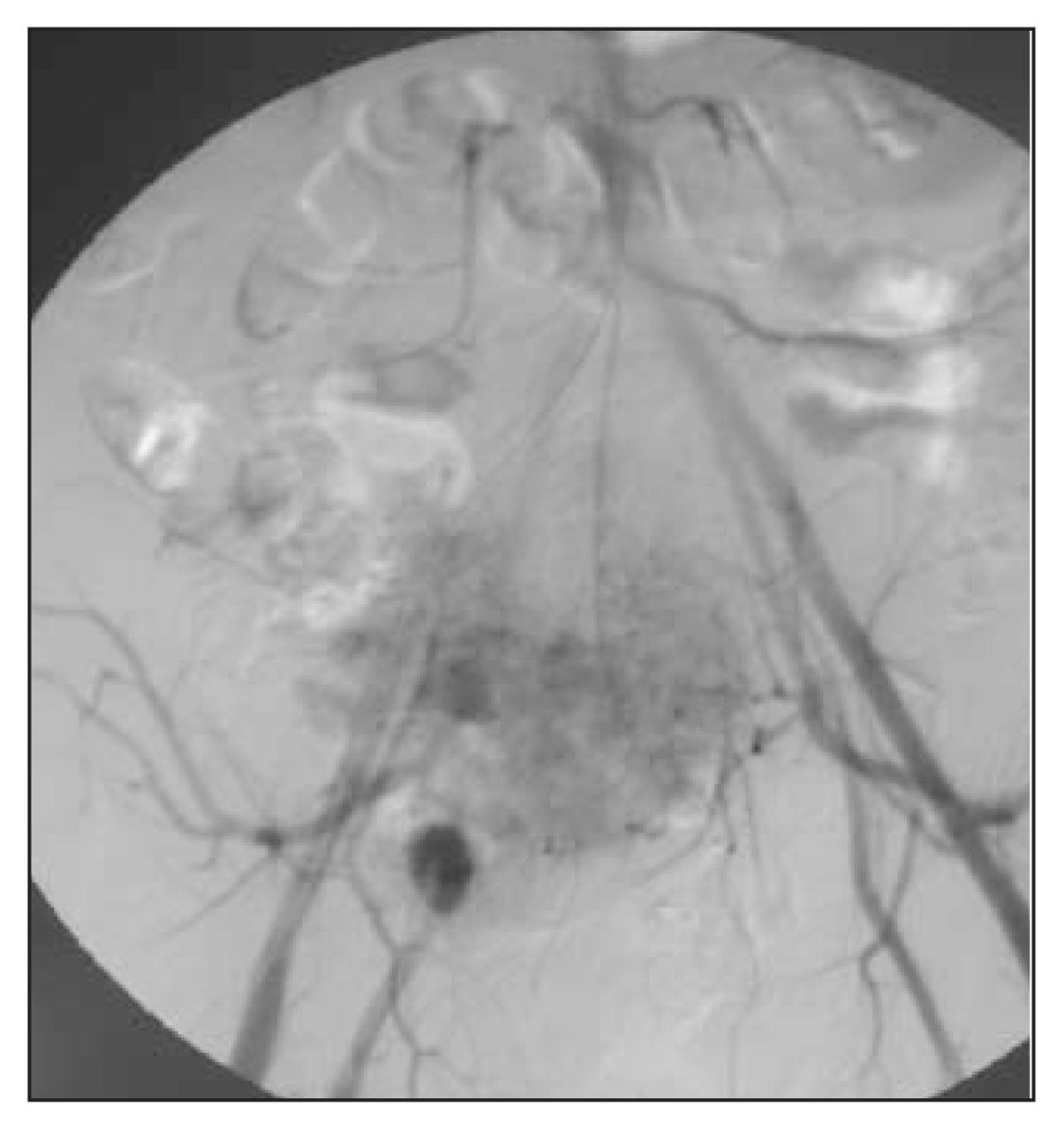
Angiogram shows the vascular nature of the tumour.

Radiograph shows stabilization of the pelvis with pedicle screws into L4 and L5 and iliac wings to stabilize the pelvis.
A second-stage transperitoneal approach with mobilization of the sigmoid colon and rectum was then used to access and resect the tumour anteriorly. Two years postoperatively, the patient had some sacral root deficits on the right side but was disease free.
Footnotes
Submissions to Surgical Images, musculoskeletal section, should be sent to the section editor: Dr. Edward J. Harvey, McGill University Health Centre, Montreal General Hospital, 1650 Cedar Ave., Rm. B5.159.5, Montréal QC H3G 1A4; edward.harvey{at}muhc.mcgill.ca
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.