


Abstract
Background: Lipofibromatous harmartoma (LFH) is a rare tumour that requires early diagnosis and treatment. To alert physicians to the possibility of this tumour, we review the epidemiologic and pathological characteristics, the presentation, diagnosis and treatment of LFH in the upper extremity.
Methods: We obtained data from a MEDLINE search of the English literature from 1966 to June 2003, using the search terms “lipofibromatous,” “hamartomas of the nerve,” “macrodactyly” and “intraneural lipoma.”
Study selection: Articles that demonstrated institutional experience (epidemiologic, diagnostic and therapeutic, and complications) and those that provided general reviews were selected for inclusion. Of 501 identified articles, 42 fulfilled the review criteria.
Data extraction: Relevant clinical, diagnostic and therapeutic evaluations were extracted from the literature and synthesized.
Data synthesis: LFH is distinguished pathologically from other intraneural tumours by fibrofatty infiltration around the nerve fascicles. Typically, patients present either early with macrodactyly or later with a forearm mass lesion or symptoms consistent with a compressive neuropathy of the affected nerve. Although MRI is an important tool in the diagnosis of LFH, the diagnosis should be supported with a tissue biopsy. Treatment for patients with no neurologic deficit involves prophylactic decompression of affected nerves at all points of possible compression. Patients with macrodactyly may benefit from debulking, joint reconstruction or amputation.
Conclusions: LFH differs from other benign nerve tumours with respect to clinical presentation, pathological characteristics, MRI features and management. Because LFH is extensive and inseparable from the nerve fascicles, excision is not recommended.
Lipofibromatous hamartoma (LFH) is a benign, extremely rare intraneural tumour, which needs to be differentiated from other more common peripheral nerve tumours such as intraneural lipomas. It affects the peripheral nerves, most commonly in the upper extremity. Unlike other nerve tumours, LFH cannot be excised but requires early prophylactic decompression at points of potential compression in order to avoid permanent nerve damage. LFH was first reported by Mason1 in 1953 and then by several others.2–4 Synonyms for the condition include: fatty infiltration, 3 intraneural lipofibroma,5 fibrofatty proliferation,6 lipofibroma,7 and hamartoma,8 but LFH is currently the most accepted name.9 LFH is associated with macrodactyly in more than one-third of cases.10,11 Patients present early in childhood with macrodactyly or later in adolescence with a volar forearm mass. Symptoms consistent with compressive neuropathy of affected peripheral nerves can also occur later in life. Traditionally, management has included decompression of symptomatic nerves at points of compression and debulking of soft tissues or, in patients with severe macrodactyly, amputation. Radical excision of the affected nerve is not recommended. In this review, we will alert physicians to this rare form of nerve tumour that requires early diagnosis and treatment.
Methods
For this review we selected articles from a MEDLINE search of the English language literature from 1966 to June 2003. Further references from the bibliographies of these articles were identified and reviewed. The search terms used were “lipofibromatous,” “hamartomas of the nerve,” “macrodactyly” and “intraneural lipoma.”
Study selection
We identified 501 articles; of these, 42 articles and selected reviews demonstrated institutional experience (epidemiology, diagnosis, treatment, complications) or were general reviews.
Data extraction
From these 42 articles and reviews, we extracted all relevant etiologic, epidemiologic, pathological, diagnostic and therapeutic information and synthesized the data.
Data synthesis
Etiology and epidemiology
The etiology of LFH is unclear, although several potential etiologic factors have been described, including abnormal development of flexor retinaculum in children,7 antecedent trauma12 and chronic nerve irritation. 6 Many authors believe that LFH is a congenital condition.3,10 It most commonly manifests well before the third decade, although several reports have described patients who first presented past the fifth decade.13–17 The condition is most common among white people. It occurs sporadically across populations and has no association with neurofibromatosis. 18 LFH commonly results in digital enlargement due to an increase in perineural soft tissue and skin. When accompanied by true macrodactyly, the tumour is referred to as macrodystrophia lipomatosa. More than one-third of LFHs are associated with macrodactyly.10,11 Females are more commonly affected when macrodactyly is present;10,11 when LFH is not associated with macrodactyly, both males and females are equally affected.
The distal peripheral nerves are most often affected in LFH; cranial nerve involvement is rare.19 LFH involves the upper extremities 3 times more frequently than the lower extremities, and specifically the median nerve.20–27 Cases of LFH affecting the entire brachial plexus,28 proximal ulnar nerve,14,29 distal ulnar nerve,10 superficial branch of the radial nerve,15,30 superficial peroneal nerve31 and the medial plantar nerve of the foot32 have also been reported.
Pathological findings
Gross findings
On gross pathological examination, LFH consists of lobulated, soft, grey-yellow, sausage-shaped masses within the epineural sheath (Fig. 1). Nerves may be markedly increased in length and diameter in the involved area (Fig. 2); indeed, cases of fusiform median nerve enlargement of up to 17 cm in length and 30 mm in diameter have been reported.17,33 LFH can be extensive and follow nerves even up the brachial plexus. Along their course, the affected peripheral nerves do not adhere to surrounding tissue. 12,17,22,34,35 In some instances, hypertrophy of surrounding skin and soft tissue is associated with the enlargement of the bone (macrodystrophia lipomatosa).12

The typical gross appearance of lipofibromatous hamartoma. This 45-year-old man’s right index finger contains multiple soft, grey-yellow, sausage-shaped masses within the epineural sheath of the radial digital nerve. The epineurium of the digital nerve had extensive perineural fibrosis.

Significant enlargement can occur in a peripheral nerve affected by lipofibromatous hamartoma. In this 29- year-old man with advanced cubital tunnel syndrome, the ulnar nerve was more than 10 times larger than a typical ulnar nerve, both proximal and distal to the cubital tunnel. The ulnar nerve was slightly enlarged within the cubital tunnel and showed signs of advanced compression.
Microscopic findings
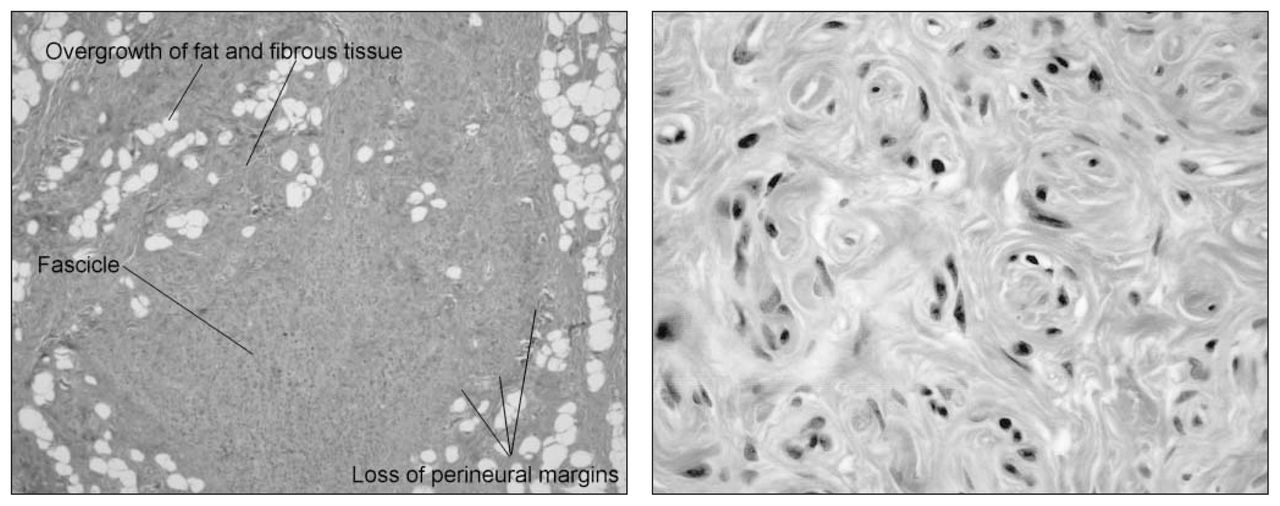
In LFH, the diffuse involvement of the nerve showing relatively bland histologic changes is consistent with a hamartomatous rather than a neoplastic tumour. The lesion is described as a hamartoma because of the overgrowth of the normal connective tissue constituents: fat and fibrous tissue (Fig. 3, left).11,23 Histopathological examination shows infiltration of the epineurium by fibrofatty tissue, which separates and compresses the nerve fascicles. This infiltration causes atrophy of the neural elements,30 often accompanied by extensive perineural fibrosis. 10,21,23 Axonal loss and collagen deposition add further chronic changes. In one case reported by Louis and Dick,25 a biopsy specimen of the median nerve showed the presence of fat and heterotopic bone, an occurrence that is very uncommon. The affected nerve may display other features in addition to adipose tissue, such as perineural septation of nerve fascicles and microfascicle formation. Pseudo-onion bulb-like hypertrophic change is an effect of the increase in perineural cells. Although this condition resembles intraneural perineuroma, it should not be misdiagnosed as such (Fig. 3, right).
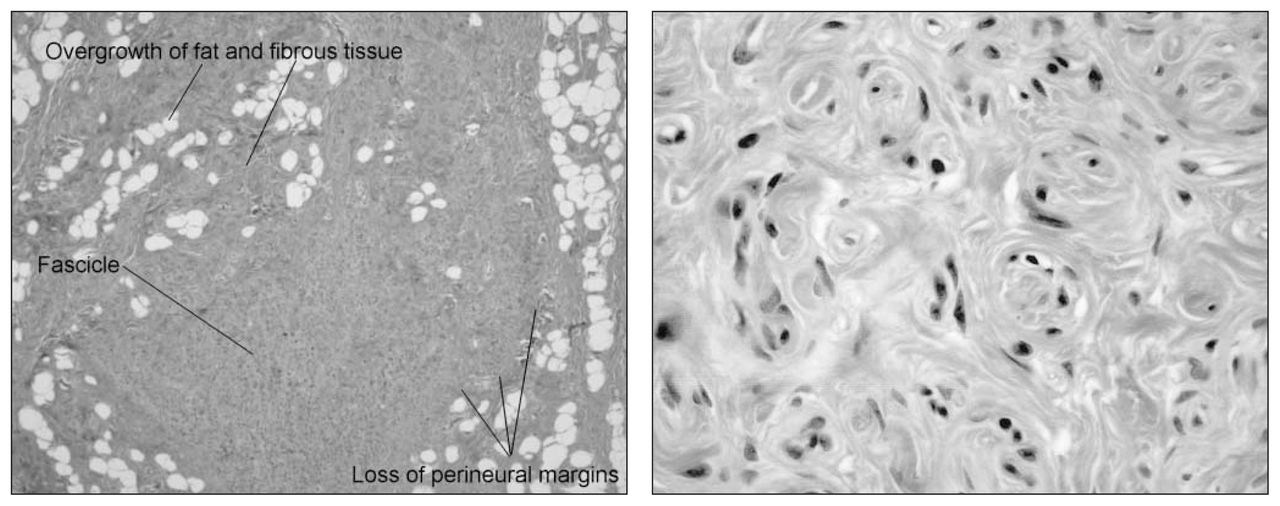
Left: characteristic histologic findings in lipofibromatous hamartoma. There is overgrowth of fat and fibrous tissue within the substance of the nerve. Note the fibrofatty infiltration around the nerve fascicles (arrows) with loss of perineural margins (trichrome stain; original magnification ×2.5). Right: characteristic pseudo-onion bulb change that may be seen due to an increase in perineural cells. Such changes should not be misdiagnosed as intraneural perineuroma (trichrome stain; original magnification ×63).
Histologic differential diagnosis
Other benign soft-tissue tumours in the upper extremity need to be distinguished from LFH; these include neurilemmomas, neurofibromas and intraneural lipomas. LFH differs from other intraneural tumours by its characteristic fibrofatty infiltration around the nerve fascicles. Neurilemmomas and neurofibromas arise from Schwann cells. Neurilemmomas are encapsulated tumours, extrinsic to the nerve fibres and easily separated from the nerve fascicles. Neurofibromas are not encapsulated and show intermingling with the nerve fascicles. Intraneural lipomas arise from normally occurring adipose cells within the nerve; like neurilemmomas, they are encapsulated and easily detached from the nerve fascicles. Finally, intraneural ganglia have been described in the histologic differential diagnosis.36 Unlike LFH, neurilemmomas, intraneural lipomas and intraneural ganglia do not intermingle with nerve fascicles.12,13,36–39
Clinical presentation
The most frequent presentation of LFH is a swelling or mass on the volar aspect of the wrist or distal forearm. The mass usually appears several years before the onset of neurologic symptoms.26 Neurologic deterioration ensues after some years.36 Associated clinical symptoms include pain and numbness, along with motor and sensory deficits in the median nerve distribution.12,23,36,40 Since most of these tumours involve the median nerve, the symptoms are caused by the compression of this nerve in the carpal tunnel.
The macrodactyly with which LFH is commonly associated can be present at birth or can be diagnosed during early childhood.39 When present, macrodactyly can be symmetric — involving equally the radial or ulnar sides of the same digit — or asymmetric. Although the phalanges are usually affected, the metacarpals are involved inconsistently. According to Dell,39 the involvement of metacarpals often occurs in older patients and is a manifestation of the severity of the disorder. Macrodactyly is unilateral 90% of the time. The majority of patients with macrodactyly present in their first to third decades because of aesthetic concerns (Fig. 4).17

Left: macrodactyly in the left hand of a 29-year-old man with lipofibromatous hamartoma of the ulnar nerve. Note the massive overgrowth of the ring finger of the left hand and the fullness along the ulnar aspect of the forearm owing to increased size of the ulnar nerve and overlying soft tissues. A ray amputation of the small finger was performed at an early age. Right: the palmar fullness along the hypothenar eminence is also caused by the increased size of the ulnar nerve and overlying soft tissues. Typically, macrodactyly is seen only in the sensory distribution of affected nerve.
Diagnosis
A carefully taken history and physical examination are the cornerstones of the correct diagnosis of LFH. Plain radiographs are valuable for assessing changes in the underlying skeleton when macrodactyly is present (Fig. 5). In some cases, a biopsy of the palmar cutaneous branch or the dorsal ulnar portion of the median nerve has been obtained to confirm the diagnosis. When this is done, the biopsy should be studied by an experienced neuropathologist so that malignant lesions such as neurofibrosarcomas can be ruled out.20,21,36,41

Characteristic radiologic features associated with macrodactyly in lipofibromatous hamartoma include symmetric overgrowth of the affected phalanges and metacarpal of the thumb and index finger with bony overgrowth concentrated around the metacarpophalangeal and interphalangeal joints.
MRI plays a major role in confirming the diagnosis of LFH. It is now being recommended for all patients suspected of having the condition. Cases are being identified more frequently as the use of MRI increases. 17 MRI not only confirms the diagnosis, it also provides a detailed assessment of nerve involvement preoperatively. A characteristic feature on MRI is the appearance of serpentiform nerve fascicles surrounded by fibrofatty tissue within the expanded nerve sheath.29 Distribution of fat between fascicles is asymmetric. On coronal images, the nerve has a spaghetti-like appearance that is pathognomonic for LFH (Fig. 6).17,42 Although MRI is an important tool in the diagnosis of LFH, the diagnosis should be supported with a tissue biopsy, particularly in cases presenting as an asymptomatic mass lesion or in centres without a large clinical experience in dealing with rare peripheral nerve tumours.
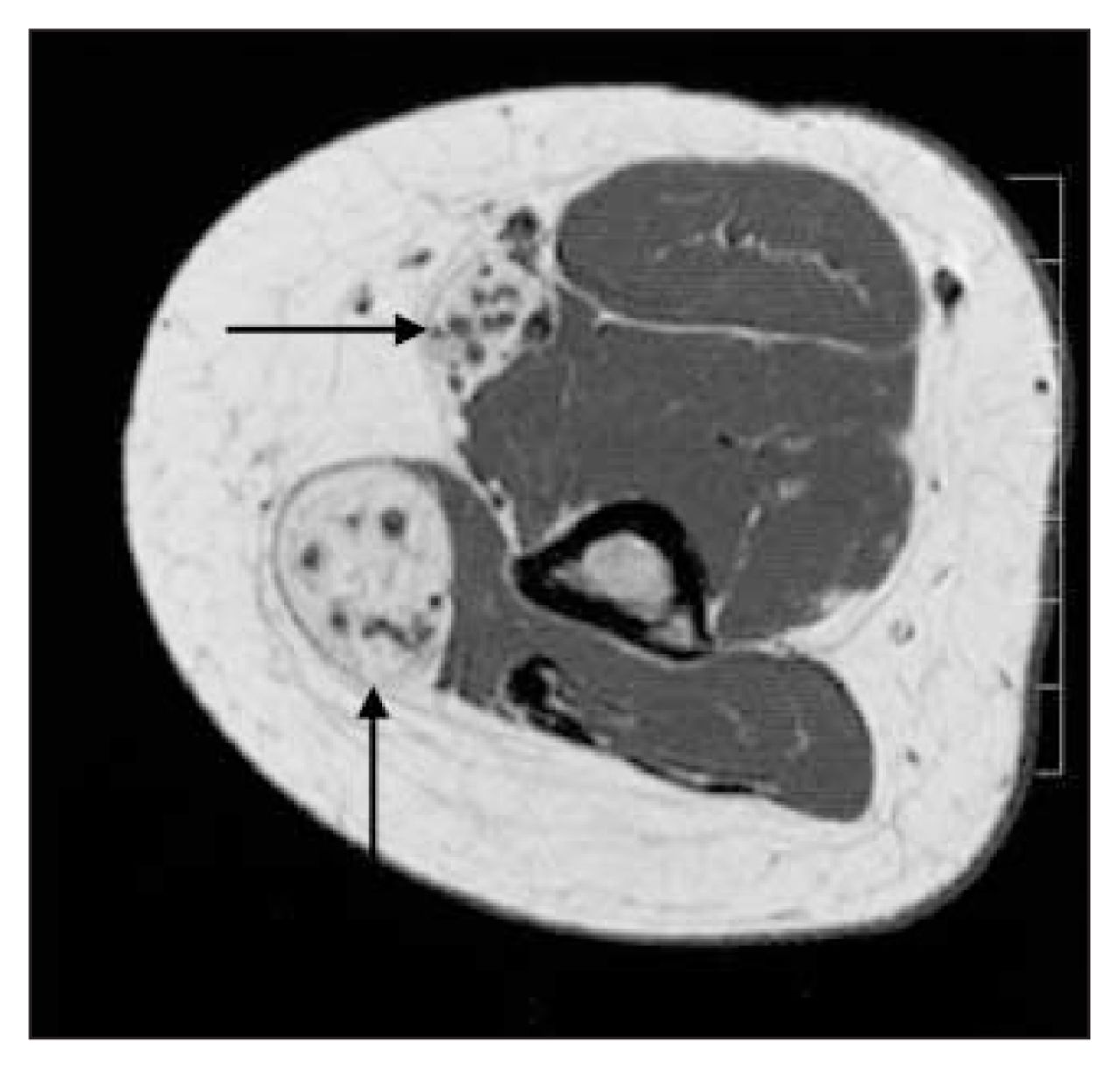
Characteristic features of lipofibromatous hamartoma seen on MRI. This axial image shows serpentiform nerve fascicles (arrows) surrounded by fibrofatty tissue within the expanded nerve sheath. Distribution of fat between fascicles is asymmetric. The nerve has a spaghetti-like appearance that is considered to be pathognomonic for lipofibromatous hamartoma.
Electromyography and nerve conduction studies (EMG-NC) can also provide valuable information needed to confirm a diagnosis of LFH. EMG-NC can show prolonged distal latency of sensory or motor innervation and fibrillations in distal muscles to confirm a compressive neuropathy.11,26,29
Treatment
Surgical excision of LFH is not recommended for several reasons. First, the effects of excision are devastating in terms of motor and sensory function. 10,12,21 Second, patients may suffer neurogenic pain after resection. Third, LFH can involve the entire nerve all the way up to the plexus, making the resection margins difficult if not impossible to identify.
In cases of LFH without macrodactyly, most authors agree with a conservative approach that includes decompression of all compromised peripheral nerves to help alleviate pain and paresthesia to reduce the likelihood of permanent motor and sensory sequelae.6,9,12,21,22,41 If the disease is extensive — with marked enlargement of the peripheral nerves as determined by MRI — consideration should be given to prophylactic decompression, even in the absence of motor or sensory symptoms. If LFH is associated with gross macrodactyly in an adult, the preferred procedure is either debulking or amputation of the finger. Amputation of the finger is less frequently indicated in childhood. 39 In selected patients, other reconstructive procedures aimed at improving hand function include joint debridement, excision of osseous overgrowth and tendon transfers (i.e., opponensplasty).
Conclusions
Our understanding of this rare benign tumour of the peripheral nerves remains limited. LFH differs from other intraneural tumours owing to its characteristic fibrofatty infiltration around the nerve fascicles, which, unlike other nerve tumours, rules out excision. LFH requires early prophylactic decompression at points of potential compression in order to avoid permanent nerve damage. Patients with significant macrodactyly may benefit from debulking, joint reconstruction or amputation. Patients who present late with advanced disease may benefit from reconstructive procedures aimed at improving hand function. Radical excision of these tumours is not recommended.
Footnotes
Presented in part at the annual meeting of the British Society of Hand Surgery, London, UK, October 2003.
Competing interests: None declared.
- Accepted July 7, 2004.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.