


Klippel–Trenaunay syndrome is a congenital disease of arteriovenous malformations. A MEDLINE search of the literature revealed no reports of total knee arthroplasty in this disease. We report one such case.
Case report
A 35-year-old man had suffered pain in his left knee for several years. He found walking extremely difficult. Nonsurgical treatment did not alleviate the pain.
On examination, he had an enlarged left lower extremity. There was an abundance of hemangiomas and varicose veins throughout the affected extremity. There was a varus alignment. He had a fixed flexion deformity with extension to only 30° and flexion to only 80°. True leg-length discrepancies were difficult to measure because of the flexion contracture. The neurologic findings were normal. The dorsalis pedis and posterior tibial arteries were difficult to palpate. However, the extremity was warm, had good capillary refill and was well perfused. Radiographs (Fig. 1) revealed severe degenerative arthritis in the left knee with bone loss from the medial plateau. The femoral condyles were large and squared. There was subchondral sclerosis with osteophytic formation. There was generalized osteoporosis. Angiography revealed that none of the cutaneous hemangiomas communicated with the deep venous system. The patient’s coagulation indices were normal.
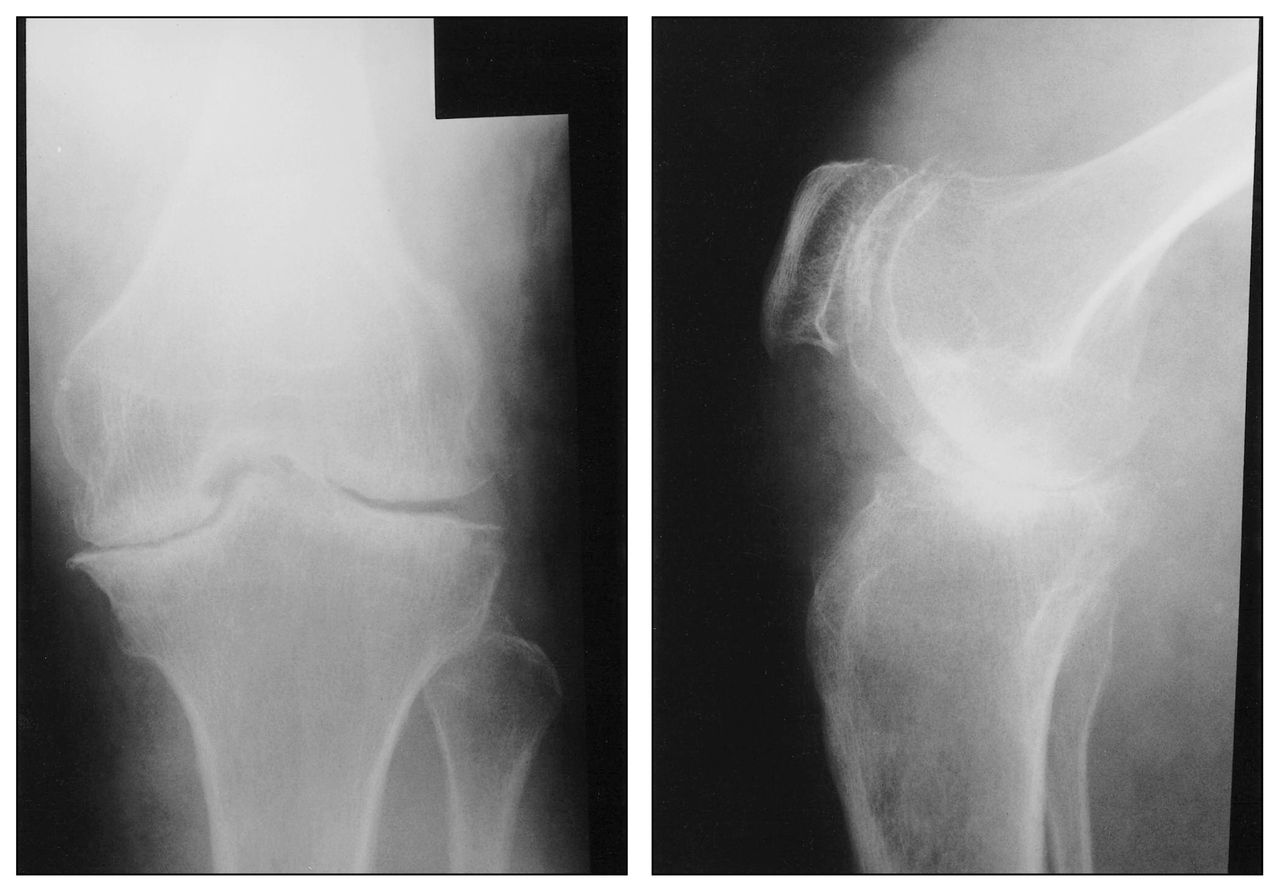
Anteroposterior (left) and lateral (right) views of the knee demonstrate severe degenerative change and “squaring” of the femoral condyles.
A tourniquet was used during surgery. Many hemangiomas and varicosities were encountered, but hemostasis was obtained. The synovium had a grey-black appearance. The remaining articular cartilage had an orange tinge. Total knee arthroplasty was performed without complication. A cemented prosthesis with modular tibial components was implanted. The patella was well preserved and not resurfaced. Patellar osteophytes were removed.
His postoperative course was uncomplicated. He did not require transfusion of any blood products. Low molecular weight heparin was administered prophylactically. He had no signs or symptoms of pulmonary embolus or deep vein thrombosis (DVT). Duplex ultrasonography of both lower extremities was performed on postoperative day 5. The scan was technically difficult but showed no evidence of DVT.
Histologic examination of excised knee tissue showed that the synovium contained labyrinths of wide vascular spaces with occasional thrombi. The walls of the vascular spaces were formed by fibrous tissue with small amounts of smooth muscle without obvious elastic lamina resembling venous walls. The observed synovial siderosis was an apparent consequence of the vascular lesion.
Discussion
Klippel–Trenaunay syndrome has 3 essential features: cutaneous hemangiomas, varicose veins and hypertophy of the involved limbs in length or girth, or both.1 Both bones and soft tissue are usually affected by the hypertrophy. The arteriovenous malformation effects are polysystemic.
Patients with this syndrome are at risk of thromboembolic disease. Baskerville’s report2 shows that 7 (14%) of 49 patients with Klippel–Trenaunay syndrome had pulmonary emboli and 8 (16%) of 49 had DVT. Muluk and colleagues3 also suggested that patients with Klippel–Trenaunay syndrome are at risk for pulmonary emboli and DVT. Our patient was given anticoagulation prophylactically and has no evidence of DVT.
Surgery for patients with Klippel–Trenaunay syndrome has been recommended only for disabling problems when the benefit is fairly predictable.
Our patient clearly had a severe degenerative arthritis secondary to the underlying arteriovenous malformations. The radiographic findings of an enlarged and squared patella and femoral condyles, and generalized osteoporosis are similar to the radiographic findings of hemophiliac arthropathy.4 The grey-black synovium found in our patient is also similar to the synovial siderosis found in hemophilia. In both hemophilia and Klippel–Trenaunay syndrome, chronic recurrent intra-articular bleeding is thought to result in these changes. The siderosis and arteriovenous malformations found within the synovium of our patient support this theory.
There are no known previous reports of total knee arthroplasty in patients with Klippel–Trenaunay syndrome. Since the radiographic and histologic findings of knee arthropathy in this case of Klippel–Trenaunay syndrome bears a great similarity to hemophiliac arthropathy, it is reasonable to assume that the long-term results of total knee arthroplasty in this syndrome will be similar to those in hemophilia. Most hemophiliacs with total knee arthroplasty have a good to excellent long-term result.5 Long-term follow-up of our patient will reveal if this assumption is correct.
Footnotes
Competing interests: None declared.
- Accepted March 8, 2004.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.