


Abstract
Introduction: Surgical planning of high tibial osteotomy (HTO) typically requires the measurement of lower limb alignment from standing anteroposterior radiographs. Although every effort is made to maintain a standardized patient position, factors such as pain or anatomic constraints may necessitate acquiring the radiograph in a less than optimal patient position. One such constraint is natural rotation of the feet with respect to the tibia. The purpose of the present study was to investigate the magnitude of the effect of foot rotation on radiographic measures of lower limb alignment.
Methods: We analyzed 19 lower limbs from radiographs obtained from 10 people who reported to an orthopedic injuries clinic. Each patient was radiographed in 3 positions: 15° of internal foot rotation, no foot rotation and 15° of external foot rotation. We measured and compared the mechanical axis angle (hip–knee–ankle) and the mechanical axis deviation from each position.
Results: Compared with the position with no foot rotation, internal foot rotation resulted in less measured varus alignment and less mechanical axis deviation from the knee joint centre, whereas external foot rotation produced greater measured varus alignment and increased mechanical axis deviation from the knee joint centre.
Conclusions: These results indicate that patient positioning is an important factor when measuring lower limb alignment from radiographs. As a result, special care must be taken when acquiring these radiographs for use in planning surgical procedures such as HTO.
Osteoarthritis (OA) is a disabling disease affecting approximately 20% of the adult population,1 and the knee is one of the most commonly affected joints.2 It is thought that lower limb malalignment is a strong risk factor for the development and progression of knee OA.3–5 Consequently, a common treatment for this disease is surgical realignment of the lower limb.
High tibial osteotomy (HTO) is a widely used lower limb realignment surgery that has been shown to successfully reduce the symptoms associated with knee OA.6–8 Patients typically report decreased pain and increased mobility in the 1-year period after HTO. However, long-term success has been reported to vary between 60% and 90%, depending on outcome criteria and follow-up length.9–12 Because many failures have been attributed to the undercorrection of lower limb alignment,6,10,12 great care must be taken in the planning of HTO.
Many authors suggest the use of standing full-length anteroposterior (AP) radiographs for planning HTO surgery and assessing postsurgical outcome.7,13–15 Identification of the hip, knee and ankle joint centres enables the measurement of the lower limb mechanical axis (hip–knee–-ankle) angle and mechanical axis deviation, both of which have been used in calculating the predicted amount of alignment correction.15,16 Although some authors suggest positioning the patient during radiograph acquisition such that the patella points straight ahead,17 this position does not necessarily control for other factors, such as foot rotation.
Most people have a natural foot rotation with respect to the tibia, with men typically internally rotated and women typically externally rotated.18 These findings suggest some segmental rotation, likely around the tibia,19 during radiograph acquisition if the foot placement is not properly controlled. Many authors18,20–25 have indicated that rotation of segments distorts the lower limb alignment as measured on an AP radiograph and have suggested a need for controlling foot placement and orientation during radiograph acquisition. This is particularly important given the current popularity of HTO in treating knee OA. Although it is well known that foot and tibial rotation alters lower limb alignment measures, little data exist on the magnitude of the effects of foot rotation on these measures when they are used in planning HTO.
Therefore, the purpose of this study was to examine the magnitude of the changes in mechanical axis angle and mechanical axis deviation measured from AP radiographs as a result of changes in foot rotation during radiograph acquisition. Specifically, changes in measured mechanical axis angle and deviation were examined from standing, full-length AP radiographs taken in 3 different patient positions: feet straight ahead, feet internally rotated 15° and feet externally rotated 15°.
Methods
A total of 19 lower limbs were examined from bilateral, standing full-length AP radiographs obtained from 10 individuals with genu varum (mean age 39.8, range 21–55 yr) who reported to an orthopedic injuries clinic with complaints of knee pain. One patient had excessive genu varum that prevented acquisition of a bilateral film; only the symptomatic limb was radiographed for that patient. All patients signed an informed consent that was approved by the institution’s ethical review board.
AP radiographs were taken in the following positions: feet straight ahead, feet internally rotated 15° and feet externally rotated 15° 26 (Fig. 1). A device similar to a protractor was placed under each patient’s feet allowing accurate manipulation of toe-out angle. During radiograph acquisition, the x-ray beam was centred on the knee at a distance of approximately 8 feet. On each radiograph, the following landmarks were determined bilaterally: centre of the hip, centre of the knee and centre of the ankle. The centre of the hip was measured as the geometric centre of the femoral head using a circular template.27–29 As suggested by Moreland and colleagues,29 the centre of the knee was measured by identifying the midpoint of the tibial spines and extrapolating inferiorly to the surface of the intercondular eminence. Last, the centre of the ankle was defined as the mid-width of the tibia and fibula at the level of the tibial plafond.28

Patient positioning during radiograph acquisition: 15° internal foot rotation (A), no foot rotation (B) and 15° external foot rotation (C).
The mechanical axis angle of the lower limb and mechanical axis deviation were measured bilaterally on each radiograph. The mechanical axis angle was defined as the included angle formed between a line drawn from the centre of the hip to the centre of the knee and a line drawn from the centre of the ankle to the centre of the knee, as shown in Fig. 2a.14 The mechanical axis deviation was defined as the perpendicular distance from the centre of the knee to a line drawn from the centre of the hip to the centre of the ankle, as indicated in Fig. 2b.28
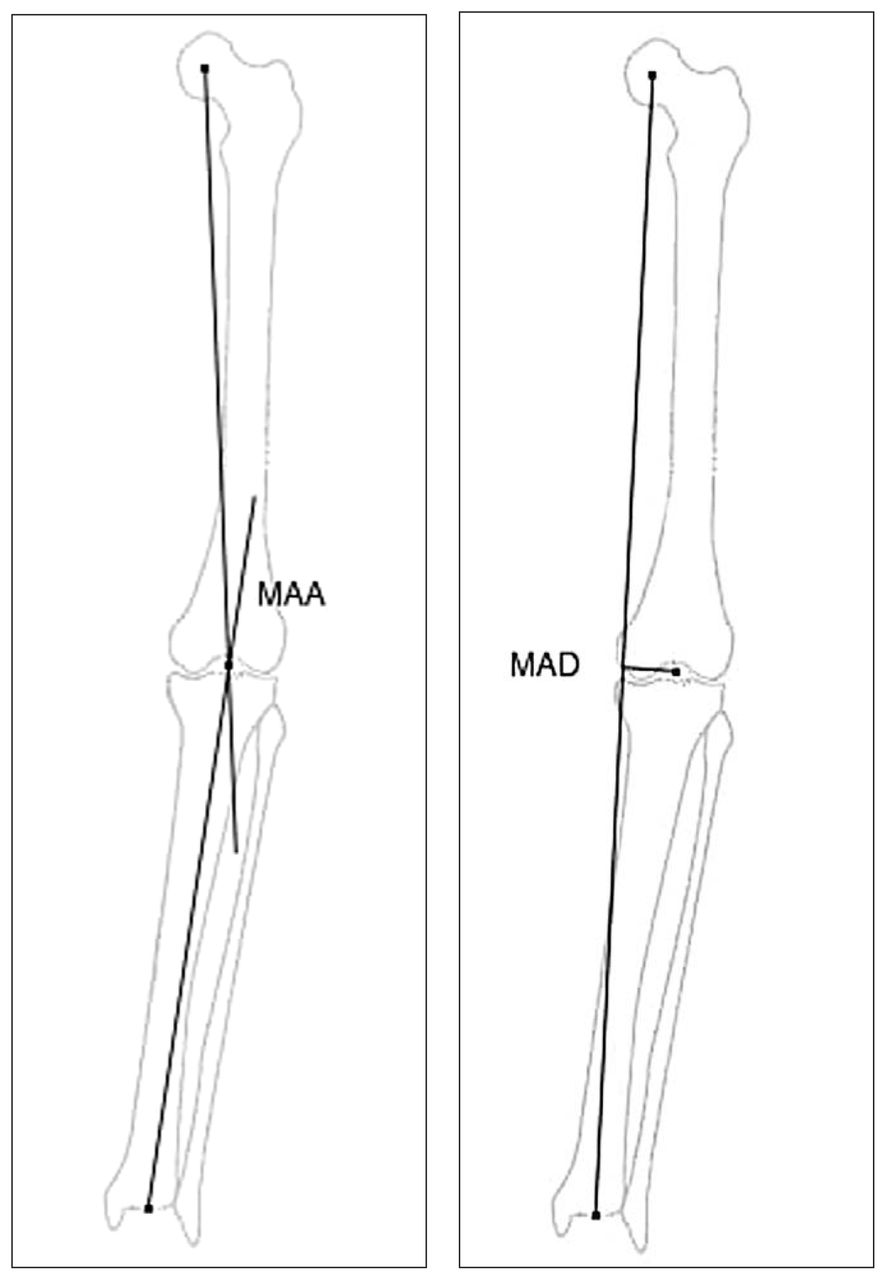
The mechanical axis angle (MAA) was defined as the included angle between a line drawn from the hip centre to the knee centre and a line drawn from the ankle centre to the knee centre (A). The mechanical axis deviation (MAD) was defined as the perpendicular distance between the knee centre and a line drawn from the hip centre to the ankle centre (B).
For the 9 subjects with bilateral measurements, the average of the 2 limbs was computed for the mechanical axis and mechanical axis deviation in each test position. For the subject with unilateral measurements, values from the single limb were used in the analysis. Differences between the 3 test positions for the mechanical axis angle and mechanical axis deviation were examined with a separate analyses of variance with repeated measures; an a priori level of statistical significance was set at 0.05. Tukey honestly significant difference post-hoc analyses were performed after the significant main effects. All statistical analyses were performed with Statistica (version 5.1, Statsoft Inc: Tulsa, Okla).
Results
Summary data for all measures and test positions are shown in Table 1. As well, radiographs for all 3 foot orientations from a representative patient are shown in Fig. 3. Compared with no foot rotation, internal foot rotation resulted in decreased measured varus and mechanical axis deviation. In contrast, external foot rotation resulted in increased measured varus alignment, compared with no foot rotation. Significant differences existed for the mechanical axis angle (F2,18 = 26.58, p < 0.001) and mechanical axis deviation (F2,18 = 24.36, p < 0.001). Tukey post-hoc analyses indicated that all positions were statistically different from each other (p < 0.05) for mechanical axis angle, as well as mechanical axis deviation. The mean differences between the internal and external rotation test conditions were 3.59° (95% confidence interval [CI] 1.81–5.37) and 13.19 mm (95% CI 6.38–19.98) for the mechanical axis angle and mechanical axis deviation, respectively.

Representative radiographs from a single subject in (A) 15° internal foot rotation, (B) 0° foot rotation and (C) 15° external foot rotation.
Mean (and standard deviation) values for mechanical axis angle and deviation for each of the 3 testing positions
Discussion
Our current study examined the effect of internal and external foot rotation on measures of lower limb alignment obtained from AP radiographs. As expected, results indicated that foot rotation had a significant effect on the measured values of the mechanical axis and mechanical axis deviation, confirming the assertions of previous authors.18,20,21 Specifically, internal foot rotation resulted in less apparent varus alignment, whereas external foot rotation resulted in greater measured varus alignment.
Observations from this study are consistent with previous findings. In a previous cross-sectional study, Cooke and colleagues21 reported that abnormal lower limb alignment in a group of patients with inwardly pointing knees was primarily due to tibial rotation. Patients exhibited greater measured varus angulation than control subjects, as well as significantly greater external foot rotation. In addition, Krackow and others25 showed mathematically that internal rotation of the hip would result in decreased apparent varus angulation, as measured on an AP radiograph, whereas external hip rotation will result in more apparent varus angulation. Similar observations would result with internal and external rotation of the tibia.
The discrepancies in measures obtained from AP radiographs arise from the complexity of obtaining a true representation of the 3-dimensional lower limb in a 2-dimensional radiograph. Three-dimensional positioning of the lower limb bones can be represented with orthogonal coordinate systems that follow the bones as they move. As a bone rotates about a single axis, the relative positioning of a point on the bone changes along the other 2 axes. This is known as kinematic crosstalk. 30–32 In our study, the movement of the tibial spines, and subsequent position of the knee joint centre, would have moved as the tibia rotated about its longitudinal axis, as it followed the rotation of the foot. Specifically, internal rotation of the tibia would shift the positions of the tibial spines medially on an AP radiograph, whereas external rotation would shift their positions laterally. Both rotations would also result in anteroposterior movement of the tibial spines that could be observed on a sagittal radiograph. Therefore, internal foot/tibial rotation would decrease apparent varus angulation, while external foot/tibial rotation would increase apparent varus angulation on an AP radiograph.
Accurate measures of lower limb alignment are critical in the preoperative planning of HTO. Many authors have reported that measures of lower limb alignment, such as the mechanical axis angle and mechanical axis deviation, are the predominant factors used in calculating the predicted correction angle.6,14,16,33 Further, it has been shown that postoperative lower limb alignment is associated with the long-term success rate of HTO.6,7,10 For example, Hernigou and colleagues6 showed that osteotomies resulting in postoperative alignment of 3°–6° of valgus were more successful than limbs with greater than 6° or less than 3° of postoperative valgus alignment.
In this study, 15° of external foot rotation was found to result in approximately 3.5° more measured varus alignment, compared with 15° of internal rotation. Therefore, if an AP radiograph taken with a foot rotation of up to 15° in either direction was used in planning an HTO, the postoperative alignment could vary by greater than 3°. If the window of success for postoperative alignment is so narrow (approximately 3° according to Hernigou), it is imperative that the measures obtained from radiographs used in the planning of these lower limb realignment procedures are indeed true measures of alignment. Therefore, care must be taken during radiographic acquisition of the lower limb in this patient population. To that end, devices that standardize patient positioning may increase the reliability and validity of radiographic measurements,20–23 thereby improving the success of HTO.
Conclusions
The planning of lower limb realignment procedures such as HTO rely on accurate measures of preoperative alignment obtained from standing AP radiographs. Results of the present study indicate that with as little as 15° of foot rotation in either direction, significant changes can occur in measured values of lower limb alignment. These findings highlight the importance of standardizing patient position during the radiograph acquisition.
Footnotes
Competing interests: None declared.
- Accepted August 23, 2005.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.