


Case report
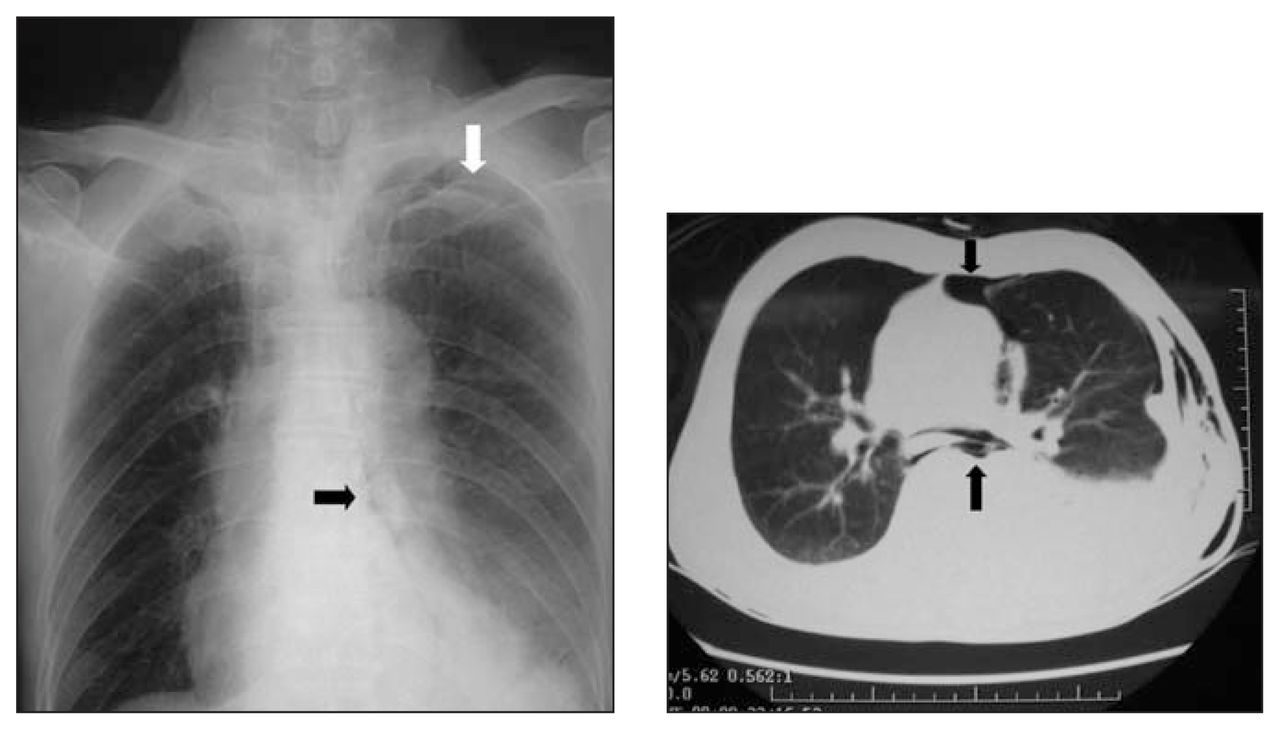
A 70-year-old man presented with nausea and a single episode of violent vomiting, followed by intense left pleuritic chest pain and epigastric pain. On admission, he was mildly agitated, tachycardic and hypotensive. Physical examination showed a tender epigastrium without guarding and with normal bowel sounds. In addition, subcutaneous emphysema was detected over the left lower chest wall, and auscultation revealed a Hamman’s crunch, suggestive of pneumomediastinum. An erect chest radiograph showed a left apical pneumothorax, pneumomediastinum and small left pleural effusion (Fig. 1a). The insertion of a chest drain yielded 180 mL of bloodstained effusion. The blood results reported leucocytosis of 17.2 × 109/L and elevated C-reactive protein level but were otherwise unremarkable. An urgent contrasted CT scan confirmed the chest radiograph findings (Fig. 1b) and also revealed significant left cervical emphysema. Esophageal perforation was confirmed after the contrast esophagram demonstrated leakage from the lower esophagus (near the esophageal gastric junction) into the left pleural space (Fig. 2). Emergency exploration through the left thoracotomy revealed a small tear in the lower esophagus, which was successfully repaired with prolene sutures and re-inforced with adjacent pleural. The patient made an uneventful recovery and was discharged on postoperative day 8.
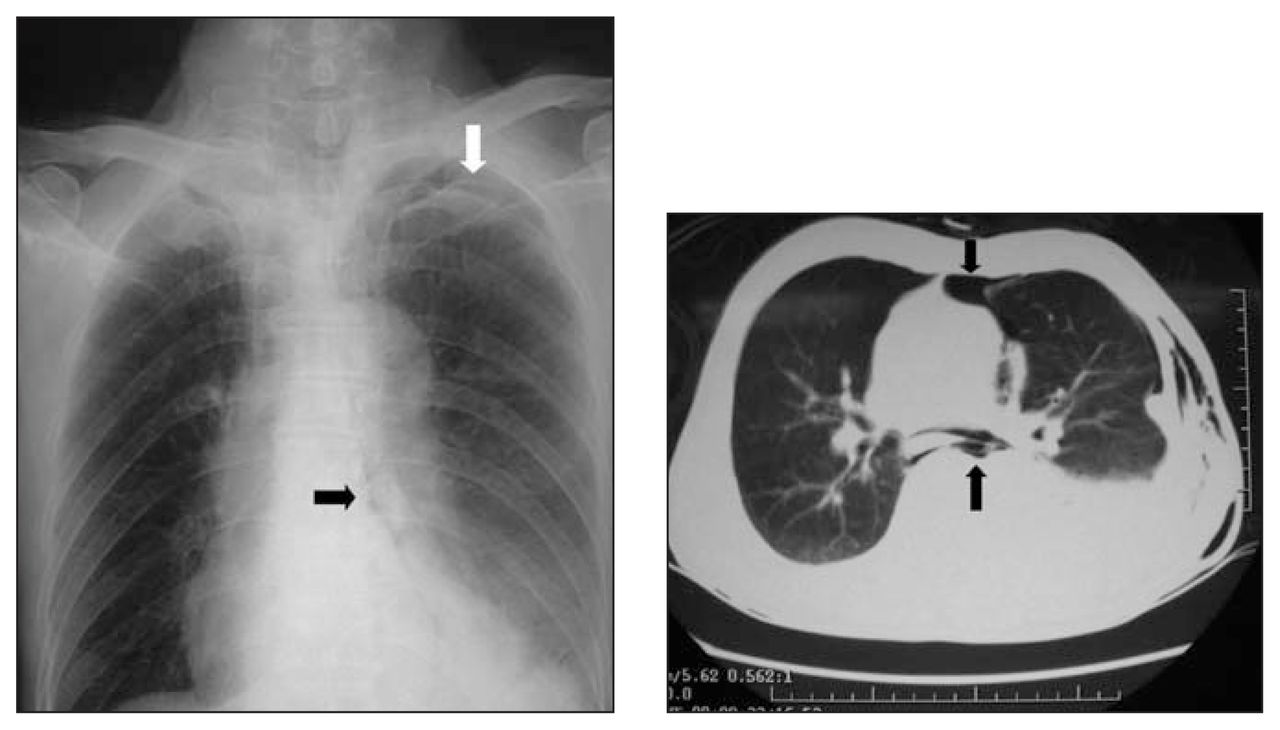
Chest radiograph showed pneumomediastinum, left apical pneumothorax and pleural effusion (left). CT thorax confirms pneumomediastinum and detected left chest wall subcutaneous emphysema (right).

Contrast esophagram demonstrated leakage from the lower esophagus (near the esophageal gastric junction) into the left pleural space.
Discussion
Boerhaave syndrome is named after Herman Boerhaave, who in 1723, elucidated the pathology of barogenic esophageal perforation by describing the fatal case of Dutch Grand Admiral, Baron Jan van Wassenaer, who vomited forcefully after a heavy meal.1 During the next 220 years, only about 50 similar cases were reported in the literature. Boerhaave syndrome is a life-threatening condition that should be diagnosed and treated urgently, because delay is well-known to result in high mortality and morbidity.2 Previously reported associations include gastresophageal reflux, neurological diseases, hypertension, alcoholism, peptic ulcer disease, esophageal stricture, esophagitis and neoplasm.
A chest radiograph may show the “V” sign of Naclerio — a V-shaped collection of air in mediastinum and along the diaphragm — indicating the presence of pneumomediastinum and pneumothorax. Pulmonary atelectasis and pleural effusion may also be found. Computed tomography is usually diagnostic, although confirmation may require an esophagram to demonstrate extravasation of the contrast and provide information on the level of perforation.3 Esophagoscopy may also be helpful but is rarely required. The effluent from the chest drain can appear clear with food particles, or it may turn rusty brown in colour in cases when diagnosis is delayed. Emergency surgical repair of the esophageal rupture is mandatory. Several reports have described thoracoscopic repair and endoscopic management strategies. However, the left-sided thoracotomy approach is most often used, although the transabdominal approach can be employed in selected cases.4 The most common intraoperative finding is a full-thickness tear at the left posterolateral aspect of the lower third of the esophagus. Débridement of the perforation, a 2-layer primary buttressed repair and drainage of the pleural cavity, remains the gold standard for treatment of this condition. Reinforcement with either pericardium, pleura, gastric fundus or absorbable mesh with fibrin glue over the repair is recommended. 5 Clinicians should have a high index of suspicion and make an early diagnosis of Boerhaave syndrome, so that prompt repair can be accomplished to minimize morbidity and mortality.
Footnotes
Competing interests: None declared.
- Accepted June 29, 2005.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.