


Abstract
Objective: To assess the effectiveness of octreotide in preventing postoperative pancreatic fistula. Pancreatic fistula is one of the most common complications after elective pancreatic surgery. Several clinical trials have evaluated the use of octreotide to prevent the development of pancreatic fistula after pancreatic surgery with conflicting recommendations.
Methods: We undertook a meta-analysis of 7 identified randomized controlled trials, reporting comparisons between octreotide and a control. The primary outcome was the incidence of postoperative pancreatic fistula, and the secondary outcome was the postoperative mortality. Results: Seven studies, involving 1359 patients, met the inclusion criteria for this review. In these studies, sample sizes ranged from 75 to 252 patients. In total, 679 patients were given octreotide and 680 patients formed the control group. Perioperative octreotide is associated with a significant reduction in the incidence of pancreatic fistula after elective pancreatic surgery, with a relative risk of 0.59 (95% confidence interval 0.41–0.85, p = 0.004). However, this risk reduction was not associated with a significant difference in postoperative mortality (p > 0.05). Conclusions: The review revealed that perioperative octreotide is associated with a significant reduction in the incidence of pancreatic fistula after elective pancreatic surgery. However, this risk reduction was not associated with a significant difference in postoperative mortality; further studies are warranted to confirm the results of this metaanalysis and to define which patient subgroups might benefit the most from prophylactic octreotide administration.
More than 31 000 people develop pancreatic adenocarcinoma each year in the United States, and almost all are expected to die from the disease.1 Pancreatic resection remains the only potentially curative treatment for carcinoma of the pancreas and periampullary region.2–8 Resection of the pancreatic head or tail and surgical drainage can also be used for the treatment of chronic pancreatitis to treat disabling pain and focal lesions.9–11 Despite advances in surgical techniques and progress in intensive care unit monitoring, the morbidity rate after pancreatic resection remains as high as 30% to 50%.12
Pancreatic fistula and pancreatic stump-related complications are the main challenge after pancreatic surgery.8,13,14 In patients undergoing pancreaticoduodenectomy, the incidence of pancreatic fistula can range from 5% to 35% in most series.15–19 Because pancreatic fistula has been identified as such a common problem after pancreaticoduodenectomy, several surgical strategies have been described to manage the pancreatic anastomosis or transected gland.20–29
Inhibition of pancreatic exocrine secretion has been proposed to reduce the rate of pancreatic fistula after pancreatic resection.30 Octreotide is a synthetic octapeptide analog of endogenous somatostatin with more potency and longer half-life.31,32 Octreotide exerts its effect by inhibiting serotonin release and the secretion of gastrin, vasoactive intestinal peptide, insulin, glucagon, secretin, motilin and pancreatic polypeptide, thus inhibiting pancreatic exocrine secretion.31,32
Several clinical trials and reviews have evaluated the use of octreotide to prevent the development of pancreatic fistula after pancreatic surgery.33–50 These reports have advocated conflicting recommendations. The objective of this study was to assess the effectiveness of perioperative octreotide in preventing pancreatic fistula after pancreatic resection.
This systematic summary of the results of published randomized controlled clinical trials (RCTs) provides the most complete evidence currently available about the efficacy and safety of perioperative octreotide administration.
Materials and methods
Inclusion and exclusion criteria
We included all published RCTs that included adults (aged over 18 yr) who underwent elective pancreatic resection (defined as surgery for pancreatic cancer, periampullary cancer and chronic pancreatitis). The intervention was octreotide or somatostatin, of a specified dose and duration, given as a prophylactic measure in the intervention group and placebo or no intervention in the control group. The primary outcome was the incidence of pancreatic fistula after pancreatic surgery (defined as postoperative drain output of fluid with amylase content more than 3 times the maximum normal serum value and exceeding 10 mL/24 h for more than 3 d). The secondary end point was postoperative death.
We excluded studies that met any 1 of the following criteria: unspecified methods of detection of pancreatic fistula or unspecified period of follow-up, surgery for acute pancreatitis and pancreatic trauma.
Literature search and data extraction
Studies were identified by searching MEDLINE, EMBASE and the Cochrane Controlled Trial Register (CCTR) on the Cochrane Library, from the earliest achievable date of each database to September 2004; we also manually searched reference lists of retrieved trials. We used the following terms and keywords: “octreotide” or “octreotide acetate” or “somatostatin analog” and “fistula” or “pancreatic fistula.” We limited studies to those identified simultaneously by the highly sensitive search strategy for identifying clinical controlled trials in MEDLINE.51
The studies retrieved by the search strategy were reviewed independently by 2 reviewers, and relevant studies were selected according to the definitions in the inclusion and exclusion criteria. Disagreements were resolved by consensus. A bibliographic software (Reference Manager V.10) was used to download all references and ensured references were not duplicated.
Data were independently extracted by the same 2 reviewers. Collected data included general demographic characteristics (e.g., mean age, sex distribution), dose of octreotide, duration of the intervention and incidence of pancreatic fistula. Where studies evaluated multiple treatment arms, comparisons were made, where possible, between octreotide and placebo. We also acquired data for quality assessment. Reasons for exclusion were documented for all excluded studies. The 2 reviewers independently extracted data on to predesigned data abstraction forms. After collection, data were checked and cross-checked. Discrepancies were resolved by consensus with the senior author.
Two reviewers independently assessed the methodological quality of all included studies, using a van Tulder quality assessment scoring system.52
Statistical methods
One reviewer entered all data into the meta-analysis software package (RevMan 4.2); the second reviewer cross-checked the printout against his own data abstraction forms. All statistical analyses were performed with the RevMan 4.2 package.
First we considered clinical homogeneity of the included studies, by assessing the study population, intervention, comparison group and outcome. Statistical homogeneity was assessed by the RevMan software. Where significant heterogeneity was present, we examined the studies for the reasons of heterogeneity. Data were considered to be heterogeneous if the chi-squared value generated by RevMan heterogeneity test was associated with a p value less than 0.1. Where significant heterogeneity was present, attempts were made to explain the differences on the basis of the patient’s clinical characteristics and interventions of the included studies. We used the random-effects method to address heterogeneity, where appropriate. 53,54 Where heterogeneity prohibited pooling, data were presented as a qualitative overview. For the outcome of interest (incidence of pancreatic fistula), we used a relative risk (RR) with a 95% confidence interval (CI). We used a fixed-effects model for pooling where the trials were homogenous (see above). Where heterogeneity was evident, we used random effects models for pooling. 53,54 We performed a subgroup analysis according to the number of centres that participated in each trial (i.e., single centre v. multicentre).
Results
We identified 14 references from the search strategy and excluded 7 studies after examining the entire manuscript. The reasons for exclusion were as follows: the outcome of interest was not measured (1 study),40 it was a different target population (1 study),33 octreotide was used for the treatment (not as a prophylactic measure) of pancreatic fistula (1 study)44 and other reasons (4 studies).34,36,38,46
Seven studies, involving 1359 patients, met the inclusion criteria for this review. In these studies, sample sizes ranged from 75 to 252 patients. In total, 679 patients were given octreotide and 680 patients formed the control group. Six of the 7 studies were randomized placebo-controlled trials; the remaining study was an RCT of octreotide versus no treatment. Five studies were multicentre: Germany (2), Italy (2) and France (1). The remaining studies were from a single centre — the United States (2). The mean age of participants ranged from 47 to 65 years and the included patients in all studies were scheduled for elective pancreatic surgery. Table 1 summarizes the characteristics of the 7 studies.
Characteristics of included studies
The daily dose of octreotide ranged from 100 μg to 300 μg administered subcutaneously, and the duration of intervention ranged from 6 to 8 days (Table 1).
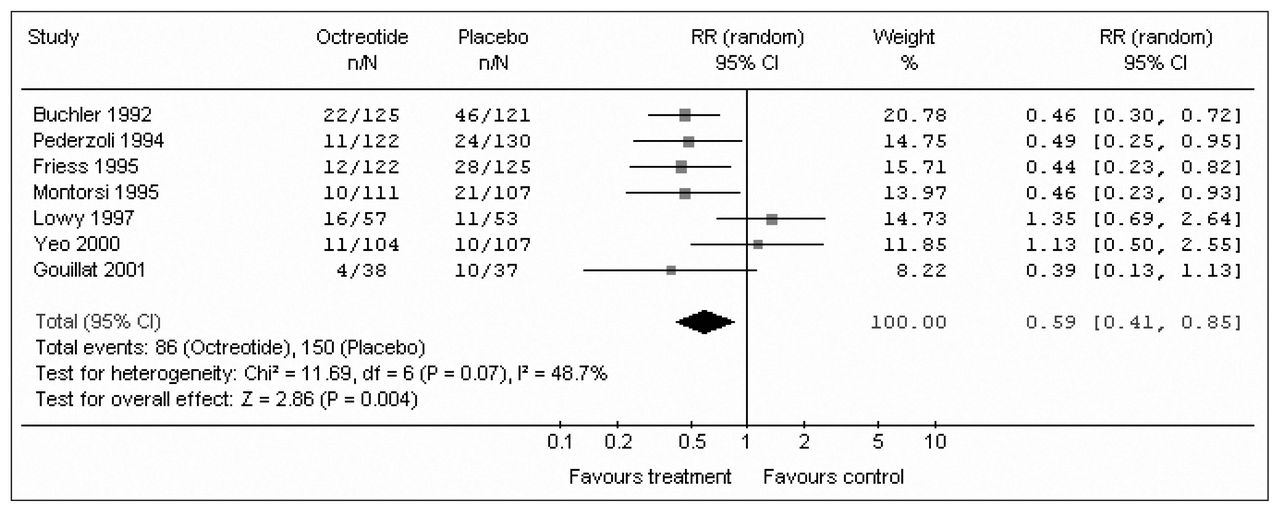
Of 679 patients in the pooled intervention (octreotide) group, 86 had a pancreatic fistula postoperatively, compared with 150 of 680 patients in the pooled control group. There was statistically significant heterogeneity (I2 = 48.7%, p = 0.07). The pooled analysis under the random-effects model showed that octreotide was associated with a significant risk reduction of postoperative pancreatic fistula (RR 0.59, 95% CI 0.41–0.85; p = 0.004). The number needed to treat (NNT) to prevent 1 patient from having pancreatic fistula was 10 (Fig. 1). A funnel plot to assess for publication bias is shown in Figure 2. The plot approximately resembles a symmetric inverted funnel (the 95% CI); all of the studies included in our final meta-analysis lie within the inverted funnel.

Meta-analysis of included studies to compare the incidence of pancreatic fistula in octreotide and control groups. RR = relative risk; CI = confidence interval.

Funnel plot. SE[log RR] = standard error of log relative risk.
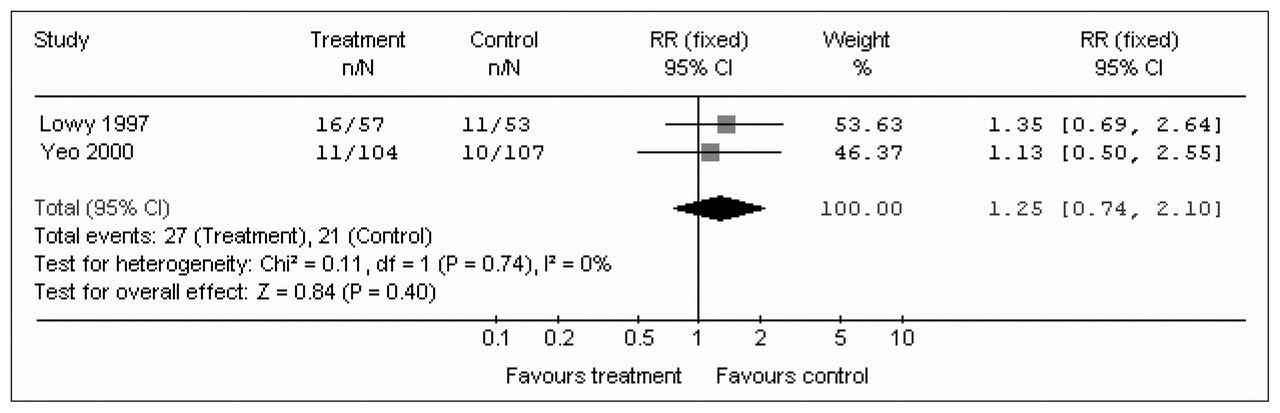
Subgroup analysis was performed according to the number of centres that participated in each trial. Five trials were from multicentres, and the remaining 2 were from single centres. In the multicentre subgroup, of 518 patients in the pooled intervention (octreotide) arm 59 had pancreatic fistula postoperatively, compared with 129 of 520 patients in the pooled control arm. There was no heterogeneity (I2 = 0%, p = 1.00). The pooled analysis under the fixed-effects model showed that octreotide was associated with a significant risk reduction of postoperative pancreatic fistula (Fig. 3) (RR 0.46, 95% CI 0.34–0.60; p < 0.001). In the single-centre subgroup, there were 161 patients in the pooled intervention (octreotide) arm, 27 of whom had a pancreatic fistula postoperatively, compared with 21 of 160 patients in the pooled control arm. There was no heterogeneity (I2 = 0%, p = 0.74). The pooled analysis under the fixed-effect model showed that octreotide was not associated with a significant risk reduction of postoperative pancreatic fistula (Fig. 4) (RR 1.25, 95% CI 0.74–2.10; p = 0.4).

Subgroup meta-analysis of multicentre studies to compare the incidence of pancreatic fistula in octreotide and control arms. RR = relative risk; CI = confidence interval.

Subgroup meta-analysis of single-centre studies to compare the incidence of pancreatic fistula in octreotide and control arms. RR = relative risk; CI = confidence interval.
The secondary end point (death after pancreatic surgery) was analyzed according to the length of follow-up. Three studies reported the 90-day mortality.35,37,43 The pooled analysis showed that octreotide was not associated with a significant risk reduction of a postoperative 90-day death (RR 0.62, 95% CI 0.26–1.48; p = 0.28), 1 study reported a 60-day mortality,42 with no significant risk reduction (RR 1.45, 95% CI 0.53–3.92; p = 0.47), 2 studies reported a 30-day mortality,39,41 with no significant risk reduction (RR 2.23, 95% CI 0.34–14.77; p = 0.4); and 1 study reported an inhospital mortality,45 with no significant risk reduction (Fig. 5) (RR 3.09, 95% CI 0.13–74.9; p = 0.49).

Meta-analysis of included studies to compare postoperative mortality stratified by length of follow-up. RR = relative risk; CI = confidence interval.
Discussion
The concept of inhibiting exocrine pancreatic secretion to prevent postoperative complications after pancreatic surgery originated in 1979, with Klempa and colleagues;30 they reported lower complication rates after a perioperative continuous infusion of somatostatin (250 mg/h) in patients who underwent a Whipple procedure. The synthetic somatostatin analogue, octreotide (SMS 201–995) is more favourable for clinical use because it possesses a longer half-life.32 Many surgeons now routinely administer perioperative octreotide to patients undergoing elective pancreatic resection.
The focus of this meta-analysis was to address the following controversial question: Is perioperative octreotide effective in reducing the incidence of pancreatic fistula and death after elective pancreatic resection?
Pancreatic fistula remains a challenging problem after pancreatic surgery. It is the most frequent complication after pancreatic resection, occurring in 5% to 35%15–19 of patients. Activated exocrine pancreatic secretion is thought to be a main etiological factor. It has been reported that the mortality after pancreatic surgery is between 3% and 10%.4,9,10,14 Our literature review identified 7 studies that were eligible for this meta-analysis: 4 European multicentre randomized, controlled double-blinded trails, 2 American RCTs and 1 French study.35,37,39,41–43,45
The 4 European studies directly opposed the results of the 2 American studies. Each of the 4 European trials reported a lower incidence of pancreatic fistula in the octreotide group. These trials were performed in many centres by many different surgeons, which might explain the high rate of pancreatic fistula in each of their placebo groups (19%–37%). This contrasts with the American studies, which were done in specialized centres with high-volume experienced surgeons. The rate of pancreatic fistula in the placebo group ranged from 6% to 9%. This low incidence cannot be explained by octreotide administration alone. The surgeon’s experience, the type of anastomosis and the quality of the tissue are important determinants.
The definition of a pancreatic fistula is very important. In this meta-analysis, we defined pancreatic fistula as a postoperative drain output of fluid, with an amylase content of more than 3 times the serum level, exceeding 10 mL per 24 hours for more than 3 days; this biochemical leak is more liberal and is adopted by European studies. Yeo and colleagues45 adopted a more conservative definition (> 50 mL after postoperative day 10). They considered biochemical leak to be unimportant, because the most leaks resolve without squelae. Lowy and colleagues41 separated both leaks. The clinical leak rate was 12% in the octreotide group, versus 6% in the placebo group, whereas the total leak rate (clinical and biochemical) was 28% in the octreotide group versus 21% in the control group. The discrepancy in the rate of pancreatic fistula between the European and American trials may partially a result of the inclusion of more biochemical leaks in the early trials.
In the European studies, patients were stratified into 2 groups: high-risk patients (soft pancreas, nonpancreatic and periampullary tumours) and low-risk patients (fibrotic pancreas, chronic pancreatitis). The low-risk group of patients had more favourable pancreatic tissue with which to create an anastomosis, due to the fibrosis of the gland, a larger pancreatic duct and, perhaps, a reduced overall pancreatic exocrine function.
Lowy and colleagues41 reported a single-centre trial at the University of Texas MD Anderson Cancer Center in Houston, Texas. All 120 patients underwent pancreaticoduodenectomy, with use of a standard operative technique. The rate of pancreatic fistula was 6% in the control group and 12% in the octreotide group. This study has received some criticism, because 46 of 110 patients received preoperative chemoradiation, and 64 of 110 patients received intraoperative radiation; this could have resulted in a lower complication rate.41 Yeo and colleagues45 at Johns Hopkins Hospital, Baltimore, studied 211 patients undergoing pancreaticoduodenectomy. The rate of pancreatic fistula was 9% in the control group and 11% in the octreotide group. They concluded that prophylactic octreotide has no benefit and should be eliminated at a considerable cost savings.
Octreotide is a well-tolerated drug with few side effects. The main side effect is pain at the injection site. Buchler and others35,36 reported 31 of 125 patients with this problem; however, it did not require discontinuation of the treatment. Other side effects include hot flashes, rash, fever, nausea, emesis and asymptomatic biliary sludge. No major systemic side effects, such as glucose imbalance, were encountered in any of these studies.35,37,41–43,45
Factors influencing the risk of pancreatic fistula development after pancreatic surgery include the type of surgery (Whipple v. distal pancreatectomy), consistency of the gland and, most importantly, the surgeon’s experience. Lerut and colleagues55 described the influence of age, preoperative renal insufficiency and emergency surgery, whereas Yeo and colleagues45 described a strong association between the texture of the gland and fistula formation, with a higher fistula rate in soft-texture glands.
The type of surgery could influence the rate of pancreatic fistula development. Montorsi and colleagues42 found no statistical difference in the rate of pancreatic fistula in patients who underwent pancreaticoduodenectomy; this was supported by the findings of Yeo and colleagues45 and Lowy and colleagues.41 On the contrary, pancreatic fistula was significantly lower in the octreotide group than in the placebo group for patients who underwent distal pancreatectomy and local pancreatic resection, when combined together.
The pooled analysis of these 1359 patients — 679 in the octreotide group and 680 in the control group — showed that prophylactic octreotide is associated with a significant reduction of postoperative pancreatic fistula. Further research is warranted to define subgroups of patients who may benefit most from octreotide administration.
Conclusions
This review revealed that use of perioperative octreotide is associated with a significant reduction in the incidence of pancreatic fistula after elective pancreatic surgery. However, this risk reduction was not associated with a significant difference in postoperative mortality; further studies are warranted to confirm the result of this meta-analysis and to define which patients’ subgroups may benefit the most from prophylactic octreotide administration.
Footnotes
Competing interests: None declared.
- Accepted March 30, 2006.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.