


Surgical excision of malignant chest wall tumours may be either palliative or curative. We present a case of a myxoid chondrosarcoma that arose from the lateral chest wall, invaded the right hemidiaphragm and was compressing the right hepatic lobe. An extensive resection of the right lower quadrant of the chest wall and a wide part of the right hemidiaphragm was carried out with simultaneous reconstruction of both defects.
Case report
A 70-year-old man presented with a painless mass on the right lower section of the chest wall that had increased in size during the previous 2–3 months On physical examination, the fixed painless tumour, which was located on the right anterior axillary line at the level of the eighth and ninth ribs, measured about 8 × 8 cm. The initial diagnosis was a chest wall tumour.
Abdominal ultrasonography revealed a solid mass lesion of 4.4 × 5.1 cm in dimension, including multiple calcified foci adjacent to the anterior segment of the right hepatic lobe along with a cystic portion about 1.8 × 1.2 cm in dimension anterior to the solid mass. The abdominal vasculature was normal, with no paraaortic lymphadenopathy, localized fluid collection or other mass lesions. Whole body radioisotope scintigraphy did not reveal any bony metastases. On CT of the thorax, the same lesion measuring about 8 × 8 × 9 cm including calcified components was seen as a hypodense tumour on the anteroinferior part of the thoracic wall adjacent to the right hepatic lobe. Injection of contrast medium caused a mild radioopacity in the peripheral tissue adjacent to the tumour. The mediastinum was free of lymphadenopathy and any other mass lesions.
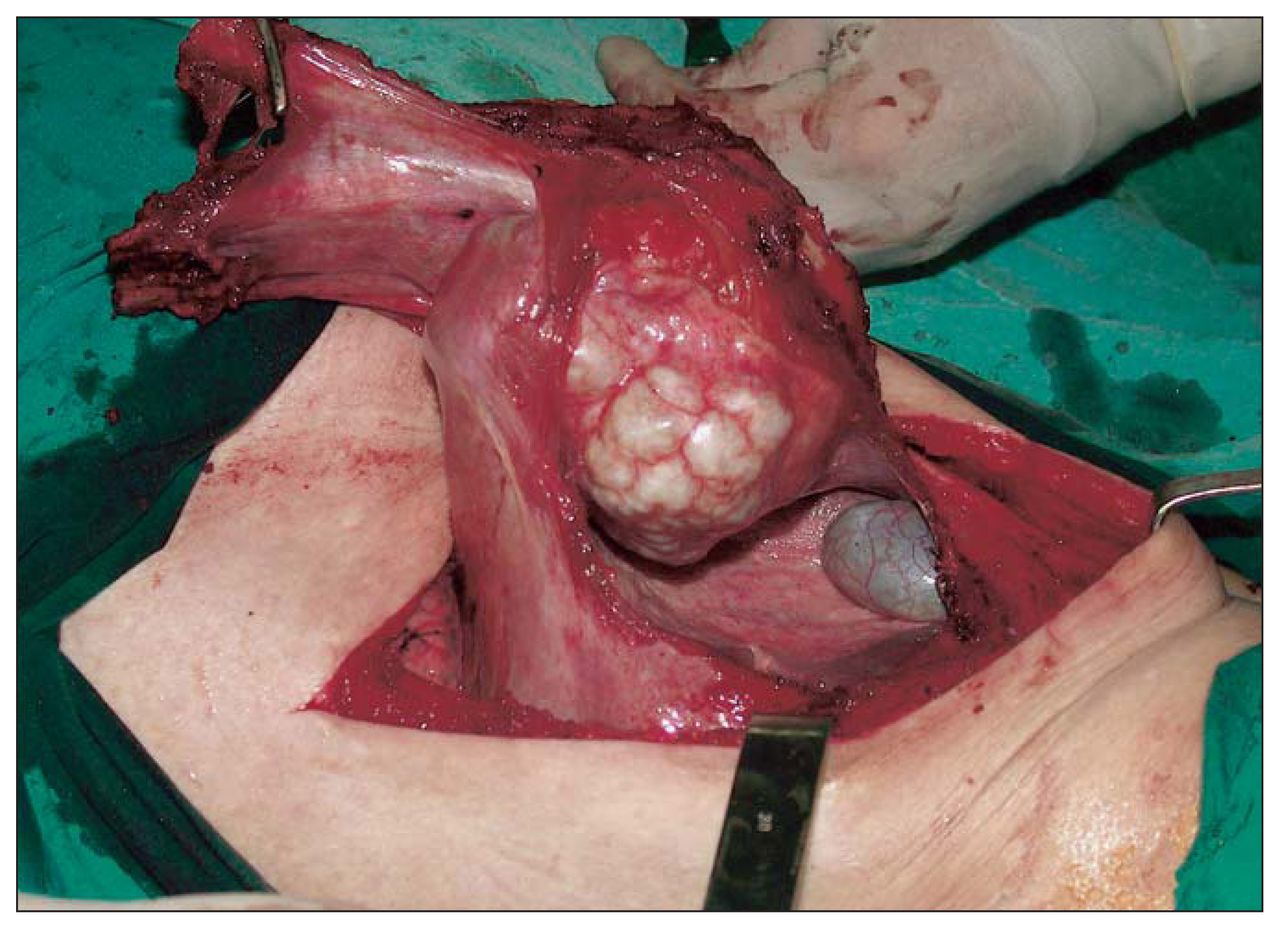
Under general and epidural anesthesia to manage the postoperative pain, controlled access to the tumour was gained through an oblique incision over the mass lesion on the right lower part of the thoracic wall. The mass lesion was observed to be located on the eighth and ninth ribs and was excised en bloc along with the endothoracic fascia securely including the seventh and tenth ribs (Fig. 1). The tumour had invaded the diaphragm. Frozen sections obtained from the adjacent liver tissue, diaphragm and endothoracic fascia were negative for tumour invasion.
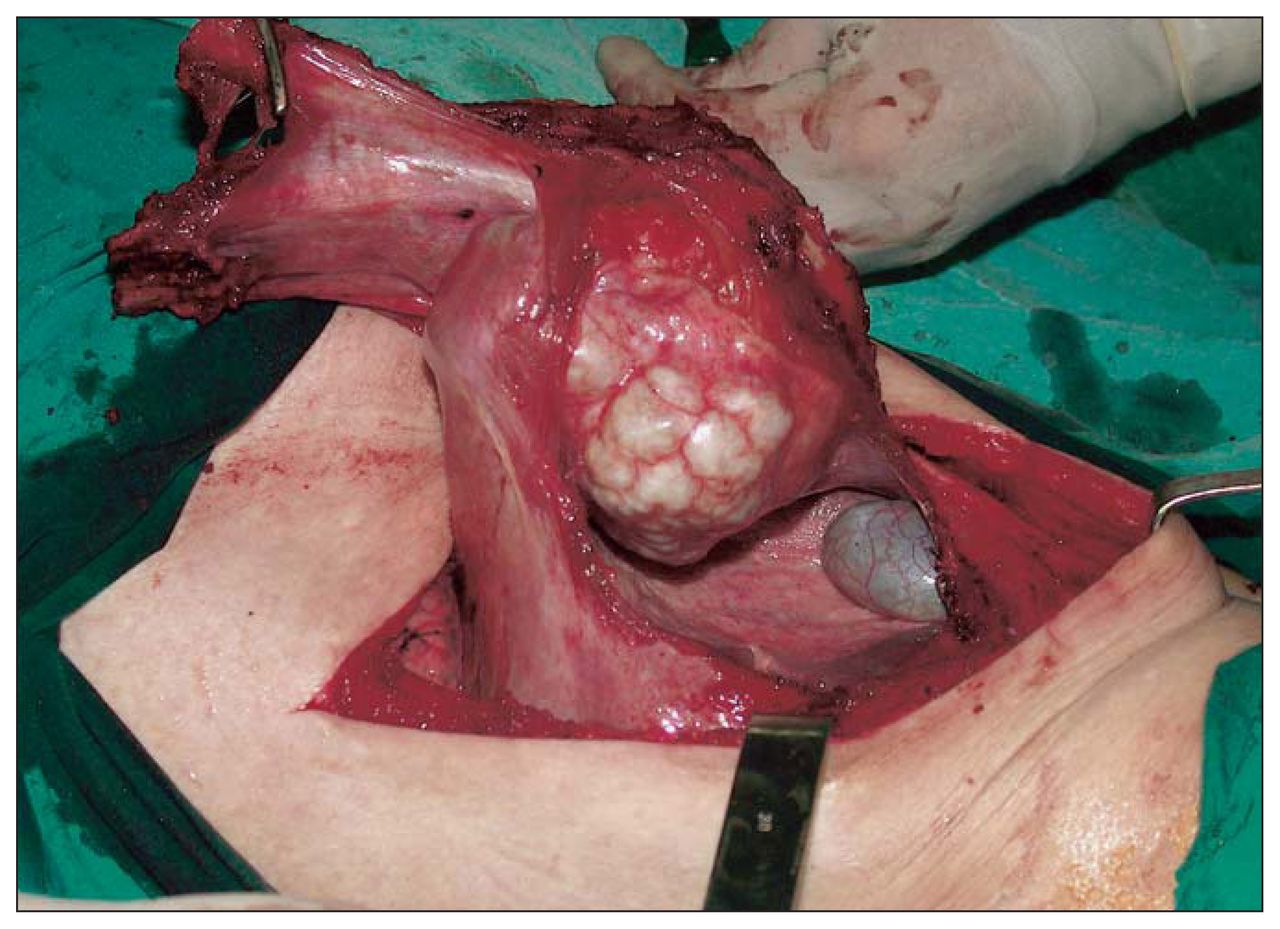
Operative view showing en bloc resection of the tumour along with the right hemidiaphragm and the chest wall.
A polytetrafluoroethylene (PTFE) 2-layer mesh (2 mm) graft was used to reconstruct the diaphragmatic defect measuring 15 × 10 cm. The reconstruction of the chest wall defect of 20 × 15 cm was achieved by using a Mersilene mesh and methylmetacrylate (MMMM) sandwich graft prepared by the surgeon (Fig. 2),3 establishing immediate chest wall stability and functional correction for the chest wall defect. Functional capacity of the lungs was also restored by this procedure. A chest tube was inserted into the thoracic cavity and a Hemovac drain placed beneath the skin covering the chest wall defect. The patient was discharged on postoperative day 6 without any complications. Pathological examination of the lesion revealed a myxoid chondrosarcoma. The patient was well, without recurrence, 4 years postoperatively.
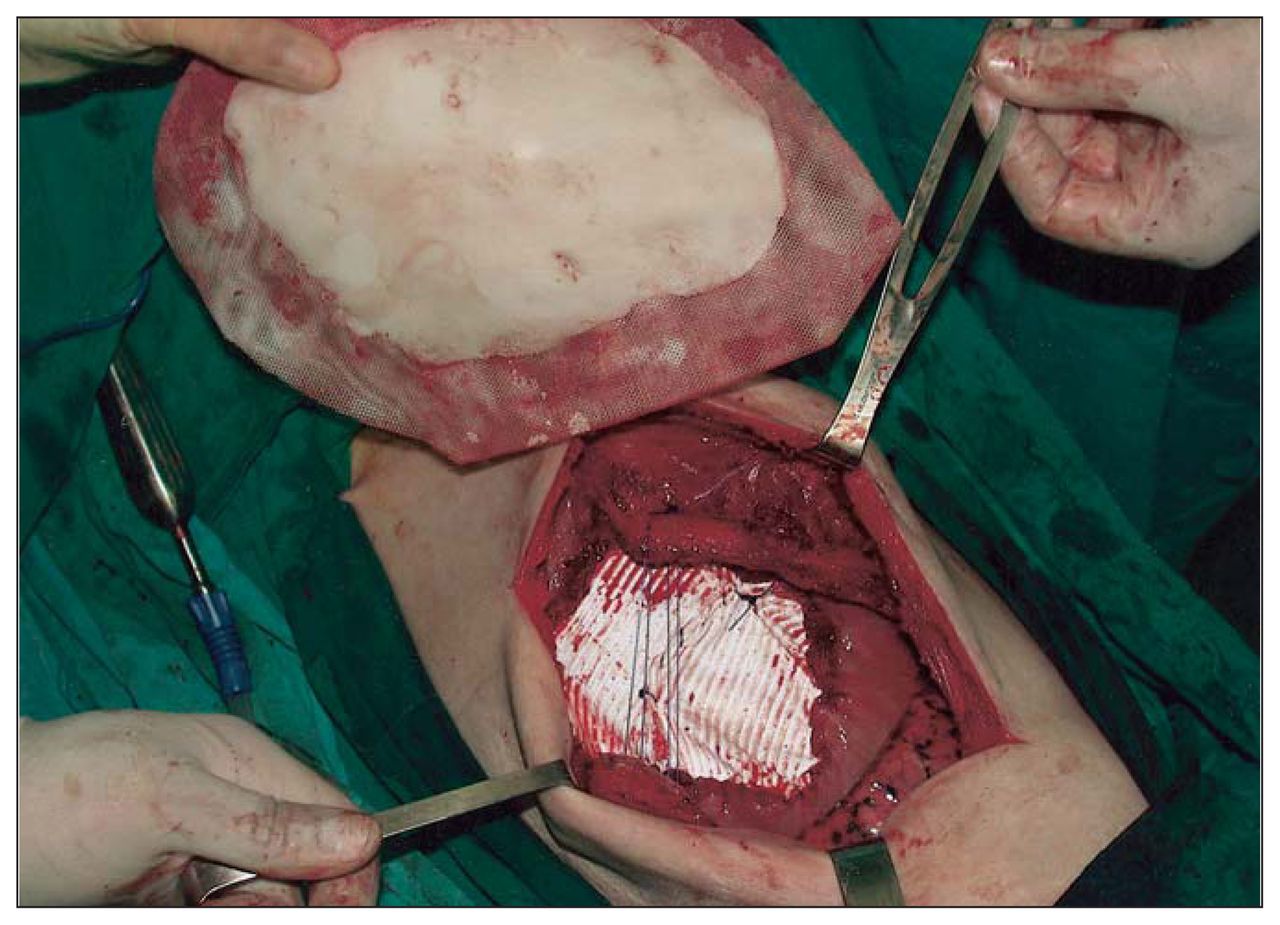
Operative view of the reconstruction process with insertion of 2-layer polytetrafluoroethylene mesh to fill the defect in the right hemidiaphragm and a Mersilene mesh and methylmetacrylate sandwich graft to close the chest wall.
Discussion
Primary tumours of the chest wall are uncommon lesions, comprising only 2% of all primary tumours. Chondrosarcoma is the most common malignant tumour of the chest wall.1 In primary chest wall tumours, the single most important factor that predicts a good outcome is complete resection of the tumour initially to prevent local recurrence and subsequent metastasis.2,3 Extensive resection of the chest wall with tumour-free margins may cause instability resulting in flail chest.4 The defect must be closed to facilitate ventilation. In our patient, the surgery proved to be curative and did not cause any instability of the chest wall or any other surgical complications such as infection, giving the patient a disease-free life 4 years postoperatively.
Our patient had a giant chest wall tumour in which the extensive defect mandated the reconstruction of both chest wall and diaphragm. Synthetic mesh is useful for reconstruction when both chest wall and diaphragm have been partially resected.4,5 MMMM sandwich graft is cheap, rigid, easily shaped and resistant to infection and provides enough stability to guard against flail chest. In this case, MMMM and PTFE grafts were effective for simultaneous reconstruction of the defects caused by excision of the primary chest wall tumour, which had also invaded the diaphragm.
Footnotes
Competing interests: None declared.
- Accepted July 3, 2007.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.