


Rupture of an aortic aneurysm into the lung characterized by hemoptysis and hoarseness is difficult to diagnose. The most common differential diagnosis is lung cancer invading the aorta.
We report on a patient who had rupture of an aortic arch aneurysm into the left upper lung accompanied by formation of a pseudoaneurysm. The condition was misdiagnosed as left lung cancer invading the aorta. The patient underwent simultaneous left upper lobectomy, aneurysmectomy and surgical repair with the use of extracorporeal circulation.
Case report
A 65-year-old woman was admitted to hospital because of a 7-day history of hemoptysis. Eight months earlier, she had presented to another hospital with productive cough, hemosputum and hoarseness. She was treated with antibiotics and nonsteroidal anti-inflammatory drugs, but her bloody sputum and hoarseness did not resolve.
Computed tomography (CT) of the chest showed a well-defined mass in the left upper lobe of the lung, which was invading the side wall of the aortic arch, and aortic arch rupture into the mass with the formation of a hematoma (Fig. 1). The mass in the left upper lobe appeared significantly larger than it had on CT 4 and 8 months earlier (Fig. 2).
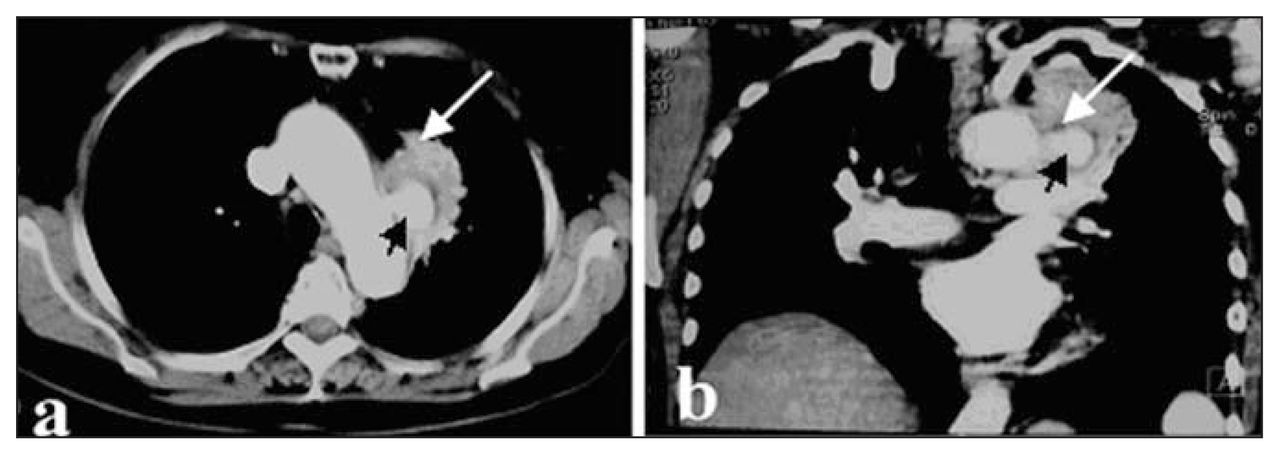
Contrast-enhanced CT scan in (a) cross-section CT and (b) the coronal plane, shows aortic arch bleeding (4 × 4 × 3 cm, black arrow) encapsulated within a mass (10 × 9 × 8 cm, white arrow) in the superior lobe of the left lung.

Contrast-enhanced CT scan (a) 8 months earlier and (b) 4 months earlier reveals a mass in the upper lobe of the left lung adhering to aortic tissue (arrows).
Findings on physical examination were normal except that respiratory sounds in the left lung were low. Results of sputum cultures were negative. The electrocardiogram showed sinus rhythm. On bronchoscopy, the tracheal cavity and bronchial lumen appeared normal, but there was left vocal cord paralysis. We considered a diagnosis of lung cancer of the left upper lobe invading the wall of the aorta. She had no history of smoking, other significant pulmonary disease, trauma or anticoagulation therapy.
The patient first underwent a left upper lobectomy. Aneurysmectomy and surgical repair under extracorporeal circulation revealed a mass measuring 10 × 9 × 8 cm abutting the wall of the aortic arch and descending aorta, a 1.5-cm long rupture in the anterior wall of the aortic arch and aortic aneurysm rupture into left upper lung with formation of a pseudoaneurysm. Histologically, tissue specimens from the left upper capsular space and the aortic wall comprised hemorrhage, necrotic tissue and fibroplasia. These findings confirmed rupture of an aortic arch aneurysm into the lung with formation of a pseudoaneurysm in the left upper lobe of the lung. The patient had an uncomplicated postoperative course. On follow-up 10 months later, a reconstructed CT scan documented complete exclusion of the aneurysm and a normal-sized aorta.
Discussion
Reports of patients with an aneurysm rupturing into the lung and presenting with hemoptysis are few. Other symptoms have been reported to typically include chest or back pain, cough and dyspnea. An aortic aneurysm or dissection that ruptures into the lung parenchyma or erodes into a bronchus can lead to acute, massive hemoptysis, but presentation with hemosputum and hoarseness is rare. Hemoptysis occurs in more than 50% of lung cancer cases and can be the result of direct invasion of the bronchial arteries, tumour manipulation during diagnostic fiberoptic bronchoscopy or distal ischemia and avascular necrosis. Direct aortic invasion by an infectious process has also been described as a cause of hemoptysis.1
Aortic arch aneurysms are most often asymptomatic but can present with symptoms caused by compression or acute aneurysm expansion, such as upper chest or shoulder pain and hoarseness. Therefore, it is difficult to distinguish between a lung cancer invading the aorta and rupture of an aortic arch aneurysm extending into the lung. In this case, the aortic arch aneurysm was misdiagnosed as lung carcinoma. We were surprised to find that the hemoptysis was actually caused by the aortic aneurysm rupturing into the lung. Our case is unique in that the aneurysm had ruptured through fibrous adhesions into the visceral pleura and lung; the blood lodged in the lung parenchyma instead of the pleural space. The fibrous tissue attachment between the lung and aorta was the result of an old adhesive pleuritis for which pathological evidence was supplied by the specimen studies. Unfortunately, angiography performed preoperatively could not identify the aortic arch aneurysm in the left upper lobe. The correct diagnosis was made by exploratory thoracotomy.
Aortic aneurysms are at an increased risk of rupture, embolization or thrombosis and should be considered for surgical repair. The surgical death rate in patients with ruptured thoracic aneurysms is high compared with that in patients who undergo elective resection.2 In a large retrospective analysis of treatment of thoracic aortic aneurysm in patients with concomitant coronary artery disease, early and long-term results demonstrated the best outcomes in patients treated surgically.3 These data suggest that aneurysmectomy with or without left pneumonectomy or lobectomy is an effective method for treating aneurysms of the thoracic aorta.
Footnotes
Competing interests: None declared.
- Accepted May 30, 2007.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.