


Pathologic fractures can occur in multiple myeloma, but bilateral fractures are rare.1,2 We report the case of a man who presented with bilateral fracture of the upper end of the humerus, and whose subsequent work-up revealed an advanced stage of multiple myeloma.
Case report
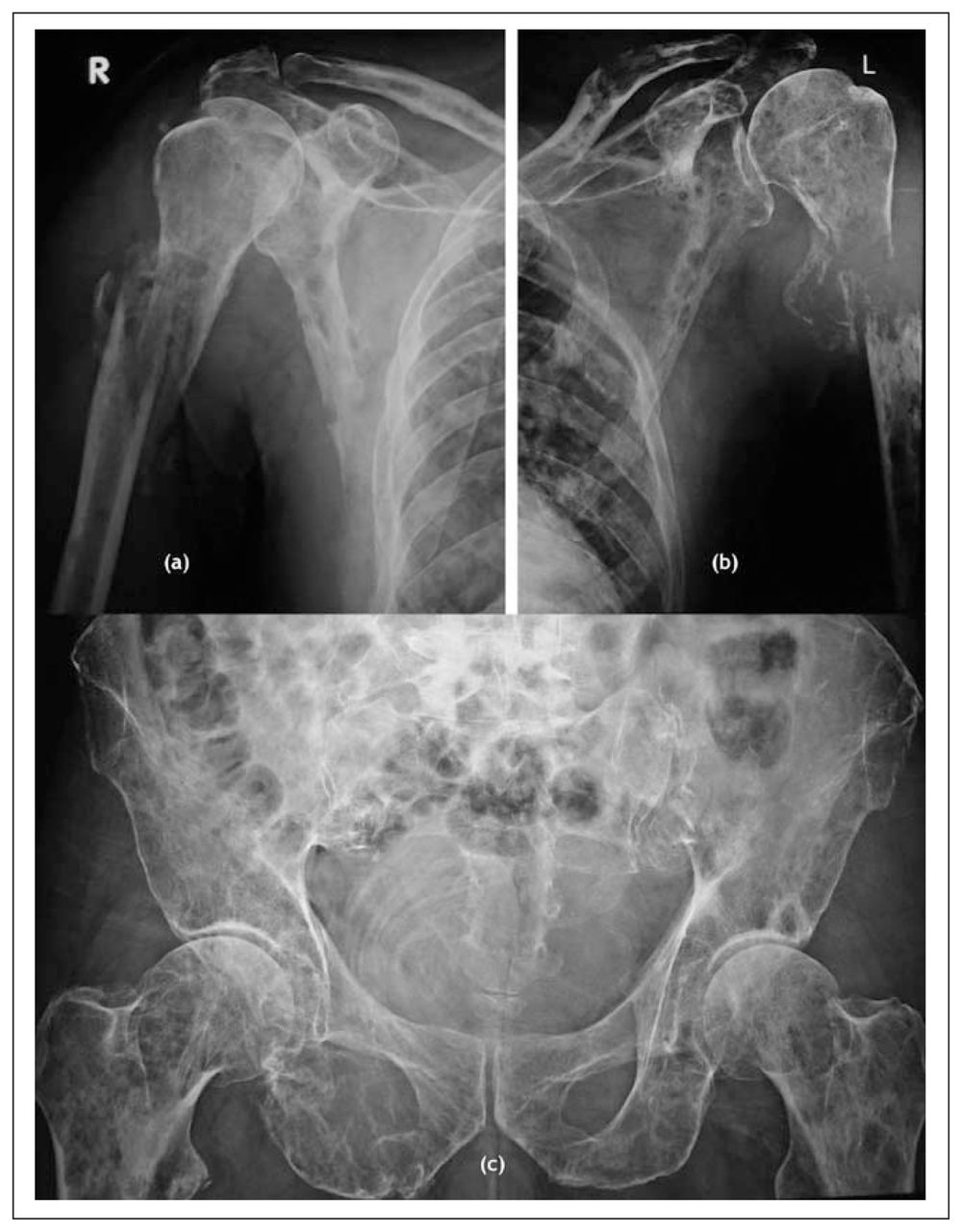
A 49-year-old man presented with complaints of bilateral shoulder pain and inability to use both upper limbs for 1 week. There was no history of significant trauma or pain. On examination, the proximal humeral region was tender and swollen bilaterally, and both hip joints were also tender. Radiographs revealed destruction of the upper ends of both humeri, with pathologic fracture (Fig. 1a, b) and multiple punched out lesions in proximal femora and pelvic bones, along with fracture of superior and inferior right pubic rami (Fig. 1c). A provisional diagnosis of multiple myeloma or metastases was considered, and both the upper limbs were splinted. The patient also had severe pallor, and tenderness was noted in the lower dorsal spine and pelvic bones. A chest radiograph appeared normal. Skeletal survey revealed lytic areas in the skull, clavicles, scapulae, ribs and spine, with collapse of the 12th thoracic vertebra (Fig. 2a, b). Laboratory tests gave the following values: hemoglobin 65 g/L, total leukocyte count 6.4 × 109/L (54% granulocytes, 42% lymphocytes, 2% monocytes and 2% eosinophils), platelets 240 × 109/L, erythrocyte sedimentation rate 108 mm/1st h, C-reactive protein 10.6 mg/L, β2 microglobulin 11.8 mg/L, serum urea 28.6 mmol/L, serum creatinine 229.8 μmol/L, serum calcium 3.6 mmol/L and serum alkaline phosphatase 192 U/L, total protein 76 (normal 62–84) g/L and serum albumin 31 (normal 36–55) g/L. Serum protein electrophoresis revealed an M band pattern and an IgA level of 9.46 (normal range 0.7–4) g/L. Urinalysis showed presence of Bence Jones proteins and a monoclonal spike of free κ light chains on electrophoresis.

Lytic lesions and destruction of the bilateral upper end of the humerus (a). Multiple lytic lesions are also seen in the clavicles and scapulae (b) and in the pelvis and proximal femora (c).

Radiograph of the cervical spine (left) showing lytic lesions (arrows) and of the dorsolumbar spine (right) showing collapse of the 12th thoracic vertebra (arrow).
Examination of a bone marrow aspirate showed moderately hypercellular marrow with megaloblastic reaction. Myeloma cells and intermediate plasma cells constituted 90% of all marrow cells. Other cells of myeloid series were depressed. A diagnosis of stage IIIB myeloma was made according to the Salmon–Durie staging system.
Normocalcemia was restored with the help of fluids, biphosphonate, corticosteroids and diuretics. The patient was given 3 units of supplemental blood to improve the hemoglobin level. A bilateral U cast was applied for the proximal humeral fractures, and a chemotherapy regimen of vincristine, doxorubicin and dexamethasone was begun. Three days later, a severe pulmonary infection developed, and the patient died 7 days after hospital admission.
Discussion
Multiple myeloma is the most common malignant primary bone tumour, characterized by uncontrolled proliferation of a clone of plasma cells within the bone marrow. It is usually found in persons older than 55 years of age, and men are more commonly affected.
Bone pain, especially back pain, is a presenting symptom of myeloma in 60% of cases.3 Presentation of the disease as bilateral, simultaneous, spontaneous fractures is extremely rare and has been reported by few authors.1,2 To our knowledge, multiple myeloma presenting as bilateral proximal humeral fracture has not been reported before.
Myeloma lesions are sharply defined, small, lytic areas of bone destruction with no reactive bone formation. The most common sites include the vertebrae, ribs, skull, pelvis and proximal long bones.3
Urinalysis shows the presence of Bence Jones proteins in about 49% of cases.4 In 83% of multiple myeloma cases, serum electrophoresis produces a single band called a monoclonal spike or M band. Urinary electrophoresis shows a spike in 75% of cases. Bone marrow shows abundant plasma cells in contrast to normal marrow, which contains less than 4% plasma cells. In the present case, bone marrow examination demonstrated 90% plasma cells.
In the early stages of the disease, scintigraphy may be helpful for areas that are not well visualized on plain radiography. Computed tomography can accurately depict the soft-tissue extent of the disease and aid in biopsy needle placement for histologic diagnosis. Magnetic resonance imaging can identify the lesions in up to 50% of asymptomatic patients.4
Chemotherapy is indicated for the management of symptomatic myeloma. The regimens generally used are melphalan and prednisone or vincristine, doxorubicin and dexamethasone. Autologous stem cell therapy achieves higher remission in young patients with low β2-microglobulin levels.3 Biphosphonates are also useful in cases of hypercalcemia and for the prevention of skeletal-related events.2 Thalidomide and bortezomib have an important role in cases of relapse and drug resistance.5 Survival with conventional therapy ranges from 1 to 10 years.3 High levels of β2-microglobulin and C-reactive protein and low levels of albumin have been associated with a poorer outcome.3 In this case, all these indicators suggested a poor prognosis.
In patients presenting with bilateral pathologic fractures, metastases should also be ruled out. This can be done easily by radiographic and laboratory examinations, but a biopsy may be required in difficult cases.
Footnotes
Competing interests: None declared.
- Accepted October 4, 2007.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.