


Presentation
A 50-year-old man presented with a slowly enlarging, painless lump in his left groin, which he had first noticed several months earlier. One of the patient’s prior radiographs is provided in Figure 1. The radiographs of his pelvis and left hip, performed for investigation of the groin mass, are shown in Figure 2. For further investigation of the abnormality seen on the radiograph, we obtained computed tomography (Fig. 3) and magnetic resonance imaging (MRI) scans. A coronal short-tau inversion recovery (STIR) image from the MRI is shown in Figure 4.

Radiograph of the left knee of a 50-year-old man, performed several years before the development of the groin mass.

Radiographs showing an anteroposterior view of the pelvis and lateral view of the left hip.

Computed tomography scan showing a transverse image of the pelvis.
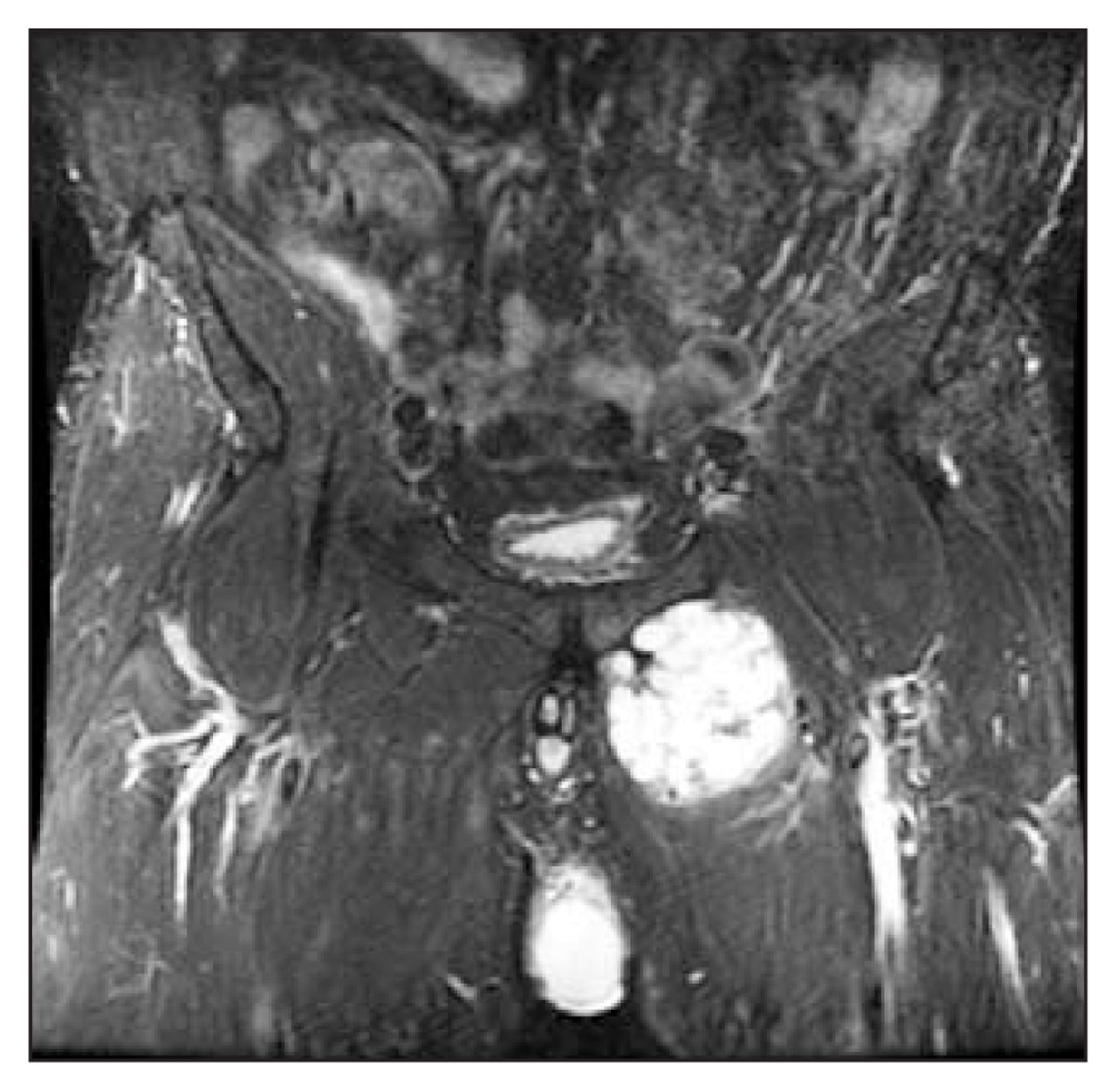
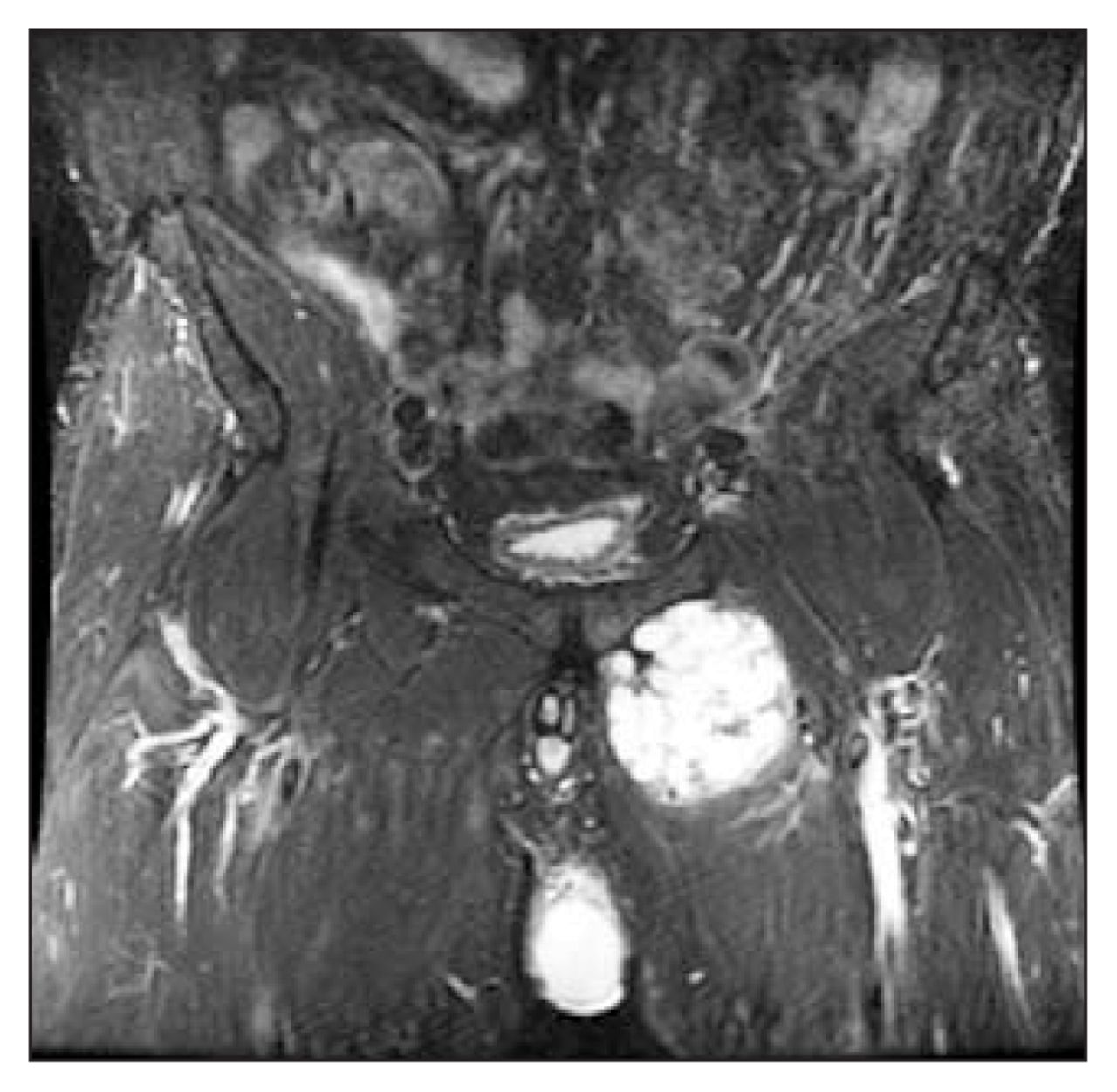
Coronal short-tau inversion recovery (STIR) image of the pelvis from magnetic resonance imaging.
What is the most likely diagnosis?
Diagnosis
Chondrosarcoma arising from an osteochondroma in a patient with hereditary multiple exostoses (osteochondromatosis)
The radiograph of the knee (Fig. 1) shows the typical appearances of hereditary multiple exostoses: there is undertubulation of the distal femur (called the “Erlenmeyer flask” deformity), and multiple osteochondromas are shown arising from the femur, tibia and fibula.
On the pelvic radiograph (Fig. 2), ill-defined, ring-and-arc–like calcification is projected over the left ischium. This is also visible on the lateral view of the left hip. Although a small, sessile osteochondroma is visible below the lesser trochanter of the femur, no definite osteochondroma can be identified arising from the ischium or pubic rami. The CT scan shows a 6-cm mass containing dense, predominantly central calcification (Fig. 3). On MRI (Fig. 4), the mass shows the typical characteristics of a cartilaginous neoplasm: predominantly high signal on the STIR image, with areas of low signal corresponding to septations and calcification. The lesion abuts the superior pubic ramus.
At surgery, we found the mass to be arising from the superior pubic ramus. Histological analysis of the resected specimen revealed low-grade chondrosarcoma.
Hereditary multiple exostoses (HME) is an uncommon skeletal disorder that is inherited as an autosomal dominant condition, with variable penetrance.1 The reported prevalence of HME is between 0.9 and 2.0 per 100 000; however, in some isolated populations such as the Ojibway in Manitoba the prevalence is as high as 1310 per 100 000 people.2 Patients usually present in childhood with a deformity or other complications related to osteochondromas such as inflammation in an associated adventitial bursa, nerve or vascular compression, stalk fracture or infarction of the cartilaginous cap.3,4 The osteochondromas found in patients with HME may arise from any bone that forms by enchondral ossification, but they are most commonly located around the knee, in the proximal femur and in the proximal humerus.5 Although radiographs often depict osteochondromas of the long bones well, when these lesions involve flat bones such as the pelvis, it can be difficult to identify continuity with the underlying bone.6
Enlargement of osteochondromas rarely continues beyond skeletal maturity, and the presence of an enlarging mass in an adult patient with HME should raise concerns about malignant transformation of an osteochondroma.7 In older literature, the risk of malignant degeneration in HME has been reported to be as high as 25%; however, more recent studies suggest a lifetime risk of less than 5%.8,9 Degeneration to chondrosarcoma is the typical pattern, although osteosarcoma and malignant fibrous histiocytoma have been reported rarely.7 Osteochondromas arising from the pelvic and shoulder girdles are more likely to undergo sarcomatous transformation.6
Footnotes
Inquiries about this section should be directed to the section editor, Dr. Peter L. Munk, peter.munk{at}vch.ca. New cases may be submitted for consideration online at http://mc.manuscriptcentral.com/cjs.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.