


Isolated internal iliac artery aneurysms are much more rare than abdominal aortic aneurysms. They represent only 1% of all cases of aortoiliac aneurysmal disease1 and 20% of all solitary iliac artery aneurysms. We report an unusual presentation of a ruptured left internal iliac artery aneurysm causing large-bowel obstruction.
Case report
A 74-year-old man presented with lower abdominal pain and a 1-week history of obstipation, nausea and anorexia. He also complained of chronic lumbar pain radiating posteriorly to both lower limbs. His medical history included coronary artery disease, hypertension, psoriasis, chronic renal failure, glaucoma and lower limb venous insufficiency.
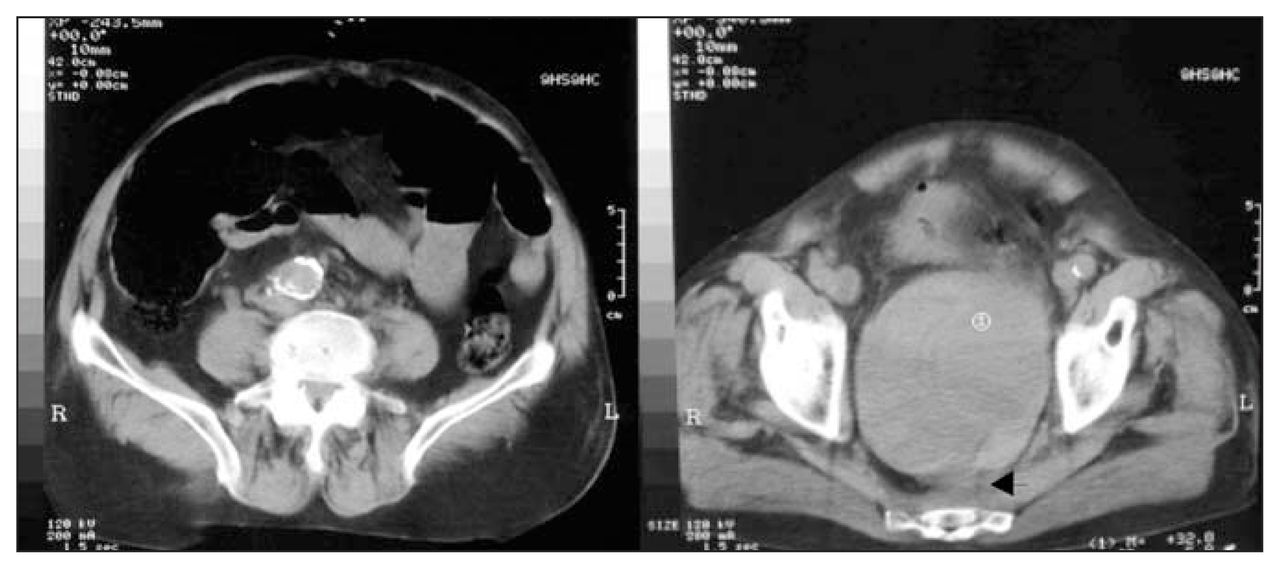
Over the previous 5 days he had been taking antibiotics orally for suspected diverticulitis but showed no improvement. Physical examination revealed severe abdominal distension with no palpable masses, diminished bowel sounds with no murmur and lower quadrant abdominal tenderness. Inspection of the perineal and scrotal region revealed an ecchymosis with no extension toward the back or flank. On digital rectal examination, we palpated an enormous pulsatile mass on the anterior rectal wall. Both lower limbs were edematous. Bilateral femoral and distal pulses were present. The serum creatinine concentration was 550 mmol/L. Plain abdominal radiography revealed a dilated colon and a mass effect in the pelvis (Fig. 1), suggesting large-bowel occlusion. Abdominal and pelvic ultrasonography disclosed a left pelvic mass, 12 cm in dimension, with bilateral hydronephrosis and normal triphasic flow through both external iliac arteries. Computed tomography demonstrated rectosigmoid compression by an enormous aneurysm and confirmed the bilateral hydronephrosis (Fig. 2). The bladder and rectosigmoid were displaced anteriorly and to the right. The infrarenal aorta was not aneurysmal but was severely calcified.

Abdominal radiographs showing distended loops of small and large bowel.

Computed tomography scan shows rectosigmoid compression by an enormous aneurysm. Arrowhead indicates the location of the rectum.
We chose a transperitoneal approach. We found that the right and transverse colon as well as the small bowel were severely dilated but viable. The left common iliac artery and external iliac artery were heavily calcified. We ligated both these arteries before decompressing the aneurysm and performing endoaneurysmorrhaphy. We used femorofemoral bypass to revascularize the left lower limb. The patient’s recovery was spectacular, with resolution of his digestive symptoms and amelioration of his renal failure. The serum creatinine concentration at the time of discharge was 187 mmol/L. Left lower limb edema persisted owing to left iliofemoral thrombophlebitis.
Discussion
Isolated internal iliac artery aneurysms are rare and are usually not diagnosed until they become symptomatic. Typically, they occur in older men and commonly have a degenerative cause. Their intimate relation to multiple structures within the pelvis explains the varying presenting symptoms, which often masquerade as digestive, urologic or lumbar spine diseases. Compression, erosion and rupture in adjacent structures may elicit urinary and digestive symptoms. The most common urologic manifestations relate to ureteral compression causing pain, hematuria, sepsis or renal failure. Symptoms of bladder compression or bladder outlet obstruction occur less frequently. Neurologic symptoms can also occur, owing to compression of femoral, obturator or sciatic nerves,2 resulting in lower limb paresia or paresthesia. Lower limb edema from iliac vein compression or arteriovenous fistula can also occur.3 Iliac artery aneurysms can mimic an ovarian neoplasm as well as prostate cancer.4 Unlike abdominal aortic aneurysms, palpation of an internal iliac artery aneurysm is usually not possible on abdominal examination. However, digital rectal and vaginal examination can reveal a pulsatile mass. Also, perianal and scrotal hematoma can be apparent when rupture has occurred.
Treament selection will depend on the hemodynamic stability of the patient, the need for pelvic decompression and the status of the contralateral internal iliac artery and aorta. The risk of rupture of the internal iliac artery aneurysm persists if both the inflow and outflow vessels are not occluded. Therefore, simple ligation of the origin of the internal iliac artery or filling of the aneurysm with coils is not sufficient to prevent rupture. Transperitoneal, retroperitoneal and endovascular operative approaches have been described. In the our case, the need for rapid decompression of the pelvis to relieve severe bowel obstruction precluded an endovascular approach that would not have resulted in an immediate decrease of aneurysm size. The transabdominal approach allows inspection of the bowel, adequate control of the calcified common and external iliac arteries, evacuation of the thrombus and suturing of the outflow vessels from within the aneurysm. We chose reconstruction through an extra-anatomic plane to reduce the risk of graft infection.
To our knowledge, this is the first reported case of large-bowel obstruction due to an internal iliac artery aneurysm. The patient presented with acute renal failure, chronic right lower limb insufficiency and posterior lower limb pain, all related to his aneurysm. These conditions were all greatly improved at the time of hospital discharge.
Footnotes
Competing interests: None declared.
- Accepted December 17, 2007.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.