


Abstract
Background: Liver resection (LR) is the only curative therapy for hepatic malignancy. Despite this, the rates of LR across Canada are unknown. We sought to determine the rate and regional variation of LR in Canada, its provinces and census divisions for the period 1995–2004.
Methods: We obtained discharge data for 1995–2004 from all provinces but Quebec from the Canadian Institute for Health Information, and we searched for LR by residential site. Then we calculated rates and variations in rates.
Results: The national age- and sex-adjusted rate of LR per 100 000 people aged 18 years and older increased from 3.22 in 1995 to 5.86 in 2004. There was a high degree of variation across provinces and census divisions.
Conclusion: Liver resection volumes are increasing in Canada. Significant regional variation exists for LR in Canada, likely reflecting a variety of important supply–demand issues.
The birth of modern hepatic resectional surgery came in 1952 when Lortat-Jacob described the first true anatomic right hepatectomy.1,2 In the years that followed, surgeons struggled with the technical demand and resource-intensive nature of liver resections (LRs), resulting in poor patient outcomes. In 1977, Foster and Berman2 reported an operative mortality of 13%, and an even higher mortality of more than 20% for major liver resections (hepatectomy, extended hepatectomy).
In the modern era, outcomes following hepatic resection have improved dramatically, with current mortality cited to be less than 6% at high-volume centres.3–10 As a result, more patients are considered as candidates for hepatic resection, as reflected by an increased rate and volume of resections performed in the United States in recent years.3,4 Improved outcomes are likely a result of general improvements in operative and anesthetic techniques, better patient selection and the emergence of hepatobiliary surgery as a distinct area of specialization.11
Despite research demonstrating regional variation in surgical procedures both in North America and Europe,12–16 little has been published with respect to hepatic resection in Canada. Regional variation may be a reflection of differences in quality of care, as it may represent a lack of uniformity in physician decision-making or disparities in patient access to care.
We sought to determine the rate of hepatic resection in Canada from 1995 to 2004. Our findings are compared to recent data showing increases in the rate of LR in the United States.3,4 We determined geographic variation through a comparison of rates among census divisions (small-area variation) and provinces (large-area variation).
Methods
We identified all patients who underwent hepatic resection in 1995–2004 using International Classification of Diseases, 9th Revision, Clinical Modification 9 and 10 codes (ICD-9 and ICD-10) from the Canadian Institute for Health Information database. This is a national database that contains patient discharge information for all hospitals in Canada, excluding those in the province of Quebec (Quebec does not report data to the Canadian Institute for Health Information).
We used patients’ postal codes to determine their places of residence, and the postal code conversion file was used to identify the patients’ corresponding census divisions. Census divisions are smaller geographic areas within provinces and territories that are useful for assessing small-area variation.
We calculated the hepatic resection rates for each province and census division. The 2 territories were grouped together owing to small population sizes, and we calculated a common rate. Rates are based on the patient’s place of residence, not where the resection was performed. We calculated the age- and sex-adjusted LR rates per 100 000 persons aged 18 years and older by the direct method of standardization that takes into account provincial and territorial population sizes. We used the year 2001 as a reference population for the calculations. The population size for each year as the denominator in our calculations came from Statistics Canada. Statistical measures used to quantify geographic variation of the adjusted LR rates across provinces and census divisions were calculated for each year and included the χ2 test, coefficient of variation (CV) and the extremal quotient (EQ). The CV is the standard deviation of the rates divided by the mean. The EQ is the ratio of the highest to the lowest rate and reflects the range of LR rates for each year.
To determine the extent of small-area variation, we compared rates among census divisions for the year 2004. We calculated and reported CV and EQ values along with a map of Canada that demonstrates census division variation in rates. To create the map, we grouped census divisions into 6 categories based on a rate ratio method where the LR rate for each census division was divided by the national median rate.
We also sought to compare the rates of LR between Canada and the United States. We obtained American LR rates for the years 1988–2000 from a population-based study by Dimick and colleagues.4 The present study and that of Dimick and colleagues are based on nationally representative databases; data from the latter study were obtained from the Nationwide Inpatient Sample (NIS), which is a 20% stratified random sample of all hospital discharges in the United States. Our study is based on data from the Canadian Institute for Health Information, which may be considered a more thorough database since it is a collection of every hospital discharge in Canada (excluding Quebec). Despite this difference, the NIS is the largest all-payer health care database in the United States and is thought to be representative of US health care statistics, making our comparison of national trends valid.
Results
Of the 9912 hepatic resections performed in our study period, the postal code data for provincial assignation were missing for 20 patients, and 6 patients were from outside of Canada. The data for census division assignation were missing for an additional 6 patients. Therefore, we omitted data for these patients from the analysis.
The national age- and sex-adjusted rates for hepatic resection for adults aged 18 years and older for Canada are shown in Figure 1. There was a marked increase from the 1995 rate of 3.22/100 000 to 5.86/100 000 in 2004. Table 1 shows the LR rates for provinces and territories, with the exception of Quebec. Although liver resection rates take into account provincial and territorial population sizes, Figure 2 is provided to demonstrate Canada’s population distribution. Table 2 demonstrates the average annual resection rate for each province and territory over the study period.

Liver resection rates in Canada.
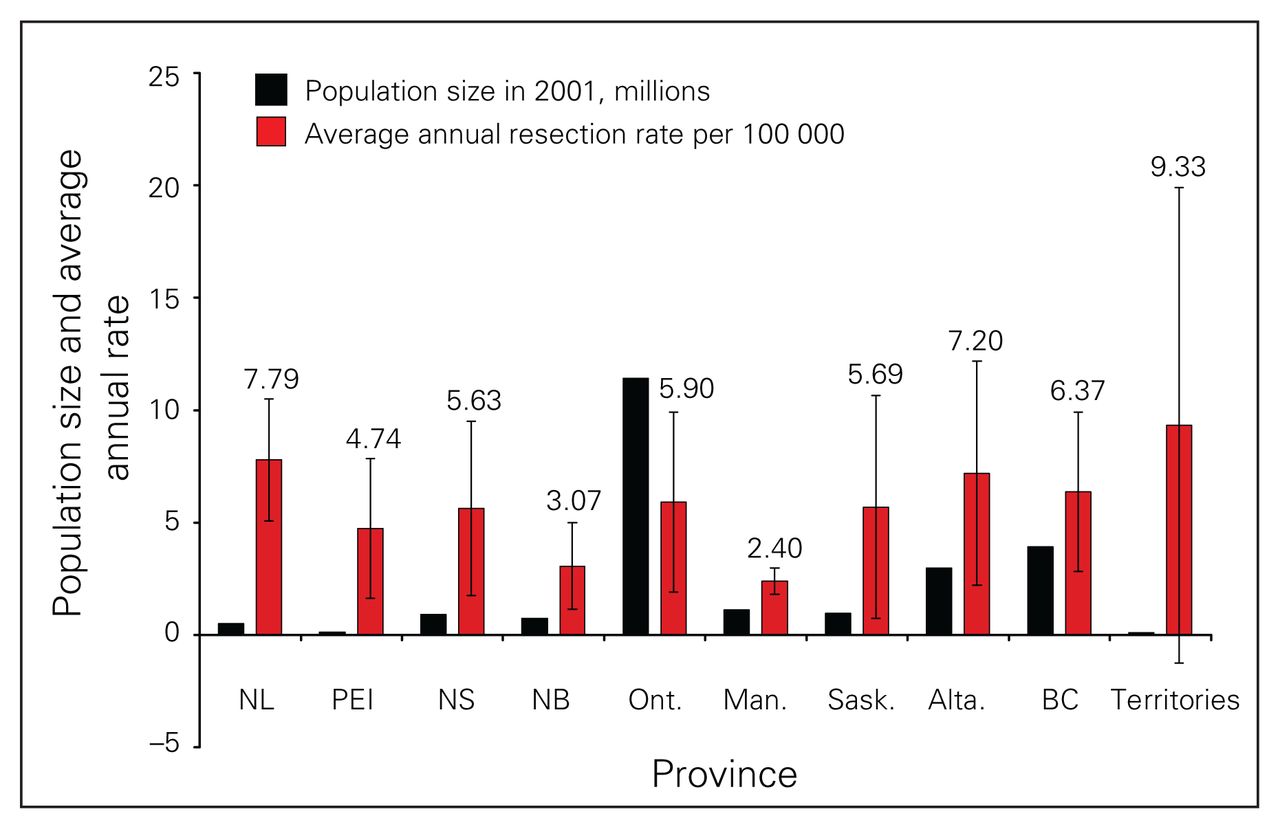
Average annual liver resection rate by province.
Rates of liver resection, by province and territory, for 1995–2004*
Average annual liver resection rates for the provinces and territories
We observed a high degree of variation in provincial rates over the study period. The EQ of greater than 3 for each year indicates a more than 3-fold variation between the highest and lowest rates. Furthermore, the EQ of greater than 3 for the average annual resection rates confirms a high degree of interprovincial variation. The rates for Ontario and British Columbia were close to the national average. The rates for the Territories, Newfound-land and Labrador and Alberta were consistently higher than the national average. The amount of variation throughout the study period varied widely (EQ 3.09–22.85). The right columns in Table 1 show the CV and EQ values for the provinces and territories over the study period. These values demonstrate significant variation among the years within the same region.
Small-area variation is demonstrated on the map of Canada in Figure 3. The map is somewhat distorted geographically because census divisions vary widely in area and sometimes bridge between islands and the mainland. The CV for census divisions was 1.80. The EQ was infinity because the rate in 76 divisions was 0, but the median rate was 3.53 (range 0–94.85). Much of the low-rate census divisions were found in the northern parts of British Columbia, Alberta, Saskatchewan, Manitoba and Ontario, which are remote from centres performing hepatic resection surgery.

Map of Canada showing the rates of liver resection by census division for 2004 (province of Quebec excluded). Variation is demonstrated by separating rates into groups based on a rate ratio method around the median.
Discussion
Our study provides information on the prevalence of hepatic resection in Canada across provinces (excluding Quebec), territories and census divisions. During our study period, the rate of LR in Canada increased by about 80%. We do not believe that the omission of Quebec from our analysis impacted our results since there is no evidence that rates in Quebec would be significantly disproportionate to those in the rest of Canada.
The rate of hepatic resection is rising in both Canada and the United States3 owing to a number of factors. First, rising rates are likely a reflection of improving perioperative mortality, now documented to be less than 6% at high-volume centres,3–10 which has led to more patients being considered as candidates for LR. Second, multiple studies have demonstrated the efficacy of modern neoadjuvant chemotherapeutic regimens in increasing resectability rates in patients with metastatic colorectal cancer (potentially curative resection rate 13.5%–38% in patients who otherwise would not have undergone LR).17–19 Such neoadjuvant therapies have increased the patient pool for resection.
From 1988 to 2000 in the United States, the rate of LR per 100 000 adults increased by 21% from 2.8 to 3.4.4 To properly evaluate LR trends between Canada and the Unites States, we compared rates for the years 1995–2000, a period of crossover between our study and that of Dimick and colleagues.4 In this period, the rate of LR increased by 34% in Canada compared with a decrease of 3% in the United States. Further, in the year 2000, Canadian surgeons performed 26% more hepatic resections, adjusted for population size, than did American surgeons.4 The higher rates for LR in Canada are in sharp contrast to other types of procedures such as various cardiac procedures, including cardiac catheterization and coronary artery bypass grafting, for which rates are much higher in the United States.20,21 This paradoxical finding needs further study, but we may speculate that it arises out of differing supply and demand dynamics for hepatic and cardiovascular disease between Canada and the United States.
We have demonstrated substantial regional variation in the rates of LR across Canada. To make sense of this population variation, we must interpret the data from the perspective of supply and demand dynamics. Varying demand for LR across regions, stemming from fluctuations in the prevalence of disease in different parts of Canada, is likely a major contributor to LR variation. Recent US data indicate that the most common indication for LR is now metastatic colorectal cancer.4 Indeed, the Territories and Newfoundland and Labrador, regions that have high rates of LR, rank among the most populous areas in Canada for colon cancer with age-standardized incidence rates of 40.2 and 33.2 per 100 000 men, respectively.22
Procedure demand also relates to the clinical thinking of referring oncologists and of the surgeons themselves. Although difficult to assess, there may be differing views on the appropriateness of LR for the same patient between different referring physicians and operating surgeons, and this variation in clinical thinking may also differ regionally. Perhaps some patients receive LR inappropriately when they have only a very remote chance of cure. Graham and colleagues21 previously discussed the concept of whether societal investment is best targeted to sick individuals (i.e., clinical interventions) as opposed to sick populations (i.e., population-based health promotion interventions). Even though the truth likely lies somewhere in between these spectral ends, physicians must recognize the impact of individual patient decisions on a society that is stressed for finances and resources. For carotid endarterectomies, the use of a surgical audit to provide surgeons with feedback on their performance and an educational system to update surgeons on new clinical practice guidelines improved levels of procedural appropriateness and reduced complication rates.23 Perhaps more initiatives such as those should be implemented to reduce heterogeneity in clinical decision-making among referring physicians and surgeons alike.
The distribution of surgeons and available operating rooms also contributes to procedural variation by altering “supply.” For example, an otherwise low-rate region based on low patient demand could produce spuriously high rates if it was overserviced with health-related infrastructure and vice versa. The observation that many low-rate census divisions lie in the northern parts of mainland provinces points to disparities in patients’ access to care. The influence of “supply” has been established in the liver transplant literature where rates of transplantation have been shown to be consistently higher in provider compared with non-provider regions in Canada.24 Distributing procedural supply based on regional patient need is vital to ensure that Canadian health care delivery is equitable.
The finding of significant variation among the years within provinces and territories points to the possibility that regional variation can be explained by chance alone. A limitation of this study that should be acknowledged is that we cannot make definitive conclusions regarding causation based on administrative data.
To summarize, we have demonstrated rising rates of LR across Canada and considerable interprovincial and inter-regional variation in the population rates of this procedure. The finding of significant variation points to a need for further evaluation because the factors underling regional variation, including the various supply and demand factors discussed in this paper, are currently poorly understood. The quality of care for patients with surgical liver disease will be uncertain unless these possibilities are further explored.
Acknowledgement
The authors thank Isabelle You, MSc, for assistance with data acquisition and analysis. Dr. Dixon is supported through a Population Health Investigator award from the Alberta Heritage Foundation for Medical Research (AHFMR) and a New Investigator award from the Canadian Institutes of Health Research. This study was funded through an Establishment Grant from the AHFMR. Dr. Ghali is funded by a Government of Canada Research Chair in Health Services Research and by a Senior Health Scholar Award from AHFMR.
Footnotes
Presented in poster form at the American Hepato Pancreato Biliary Association meeting, Mar. 27–30, 2008, in Fort Lauderdale, Fla.
Competing interests: None declared.
Contributors: Drs. Ghali and Dixon designed the study and reviewed the article. Dr. Dixon acquired the data, which he analyzed with Drs. McColl and Brar. All authors wrote the article and approved its publication.
- Accepted February 2, 2009.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.