


Case report
A 21-year-old man sustained a blunt abdominal trauma in a motor vehicle collision. The patient was tachycardic and hypotensive at presentation and reported abdominal pain and left lower extremity pain. Chest and pelvic radiographs showed no anomaly, but a plain radiograph of the left lower extremity showed an open left tibial plateau fracture. The patient was sent for computed tomography (CT) scanning.
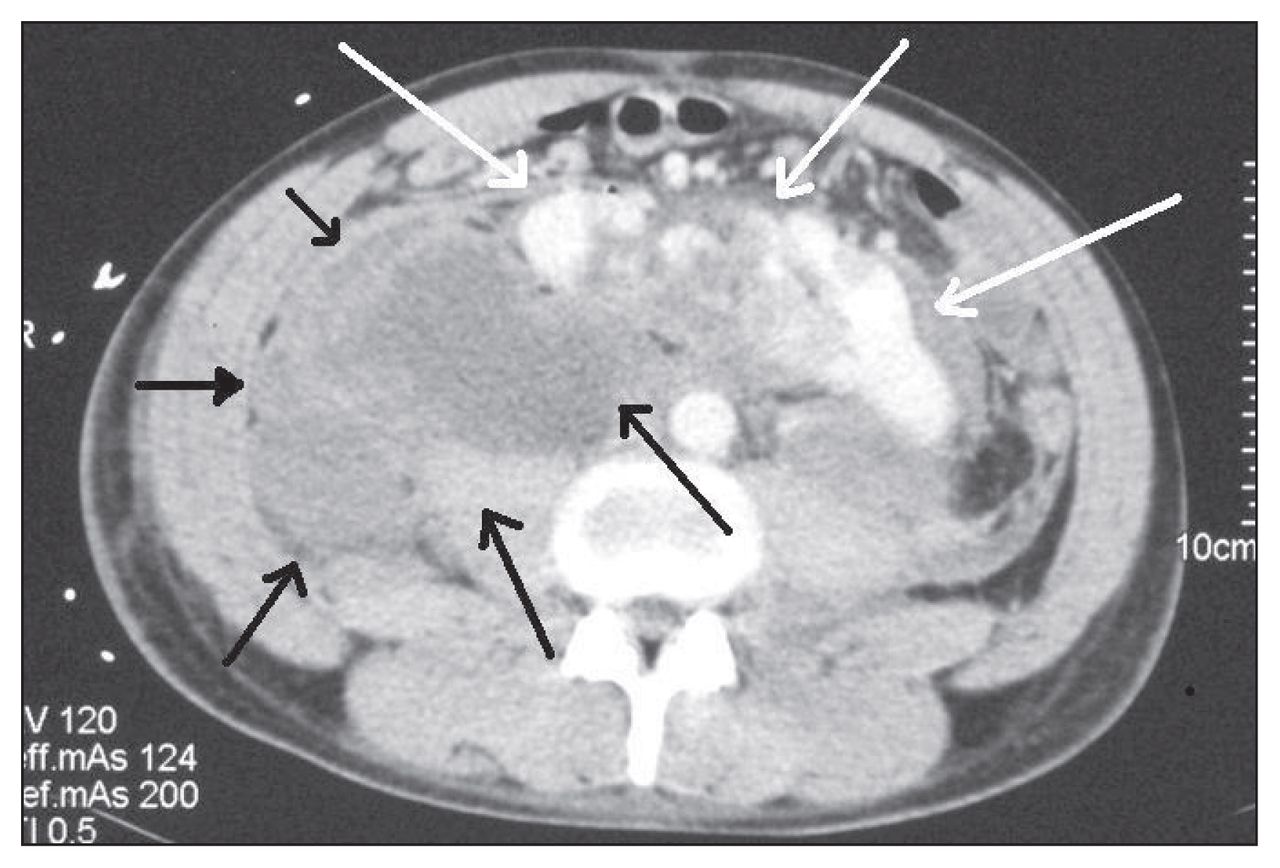
Findings on CT included a retroperitoneal hematoma adjacent to a horseshoe kidney. The right side of the kidney was found at the midline, and it was partially devascularized. There was active extravasation of the intravenous contrast at the right common iliac artery, just below the aortic bifurcation, close to the right pole of the horseshoe kidney (Fig. 1). We decided to proceed with a diagnostic angiography for the suspected iliac artery injury.

Initial computed tomography scan showing a fractured horseshoe kidney (white arrows) and a contused midportion (black arrow). A hematoma is starting to form in the retroperitoneum (striped black arrow).
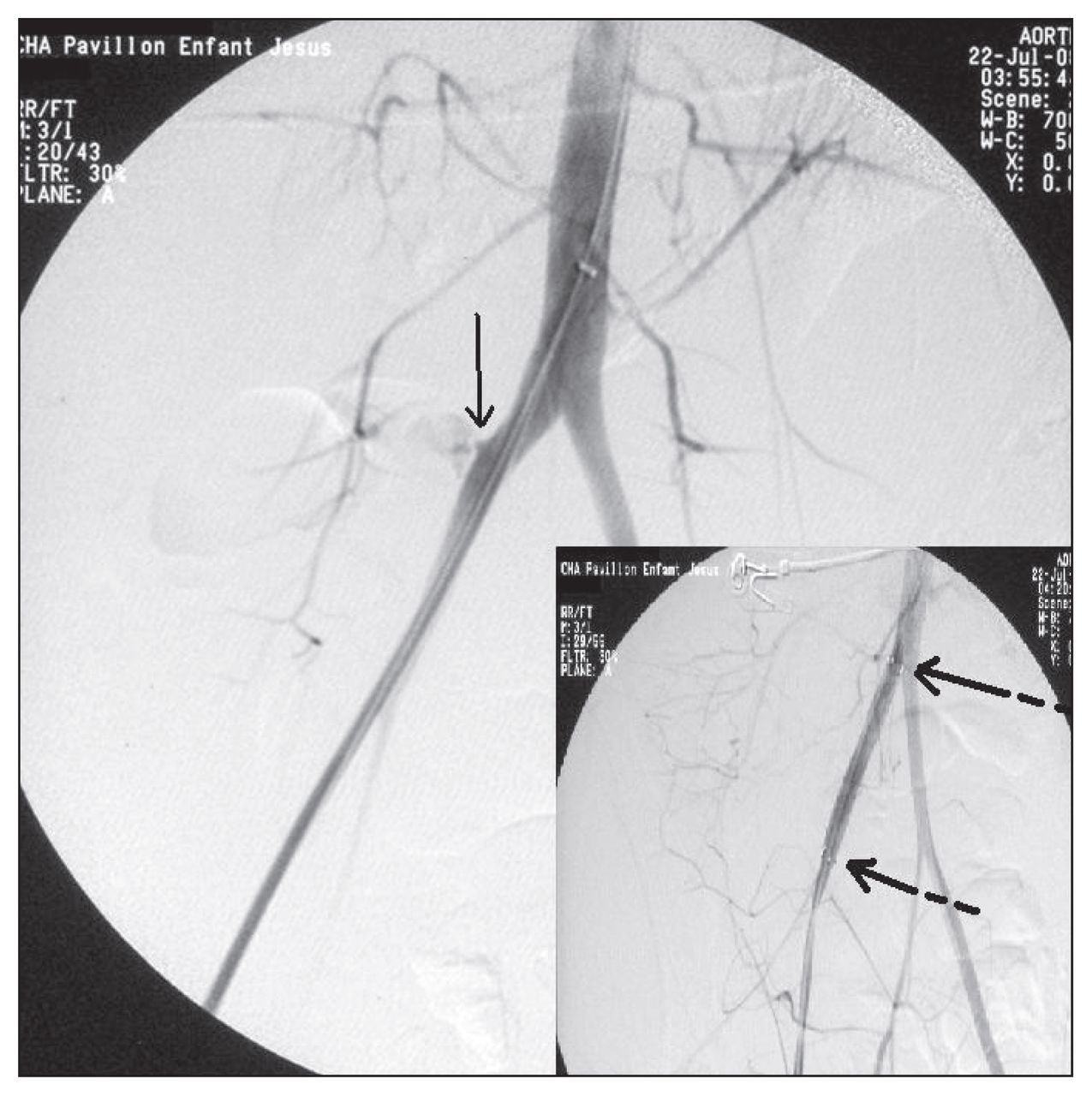
The angiogram showed that the kidney was vascularized by a renal artery originating from the aorta on each side, a single artery originating from the aorta supplied the isthmus, and an additional right polar artery was avulsed from the right common iliac artery and actively bleeding (Fig. 1). The injury was treated by placement of a covered stent (10-mm diameter, 6-cm length, Fluency Plus, self-expandable) through a right femoral access (Fig. 2). The patient’s hemodynamics improved and he was transferred to the intensive care unit (ICU). He received a total of 8 L of crystalloids, 8 units of packed red blood cells and 500 mL of fresh frozen plasma. The patient received daily acetylsalicylic acid afterwards.

Angiogram showing active bleeding from the avulsed renal artery arising from the right common iliac artery (left, solid arrow) and effective stenting of the artery with correction of the bleeding (extremities of the stent indicated by the 2 striped arrows on the right).
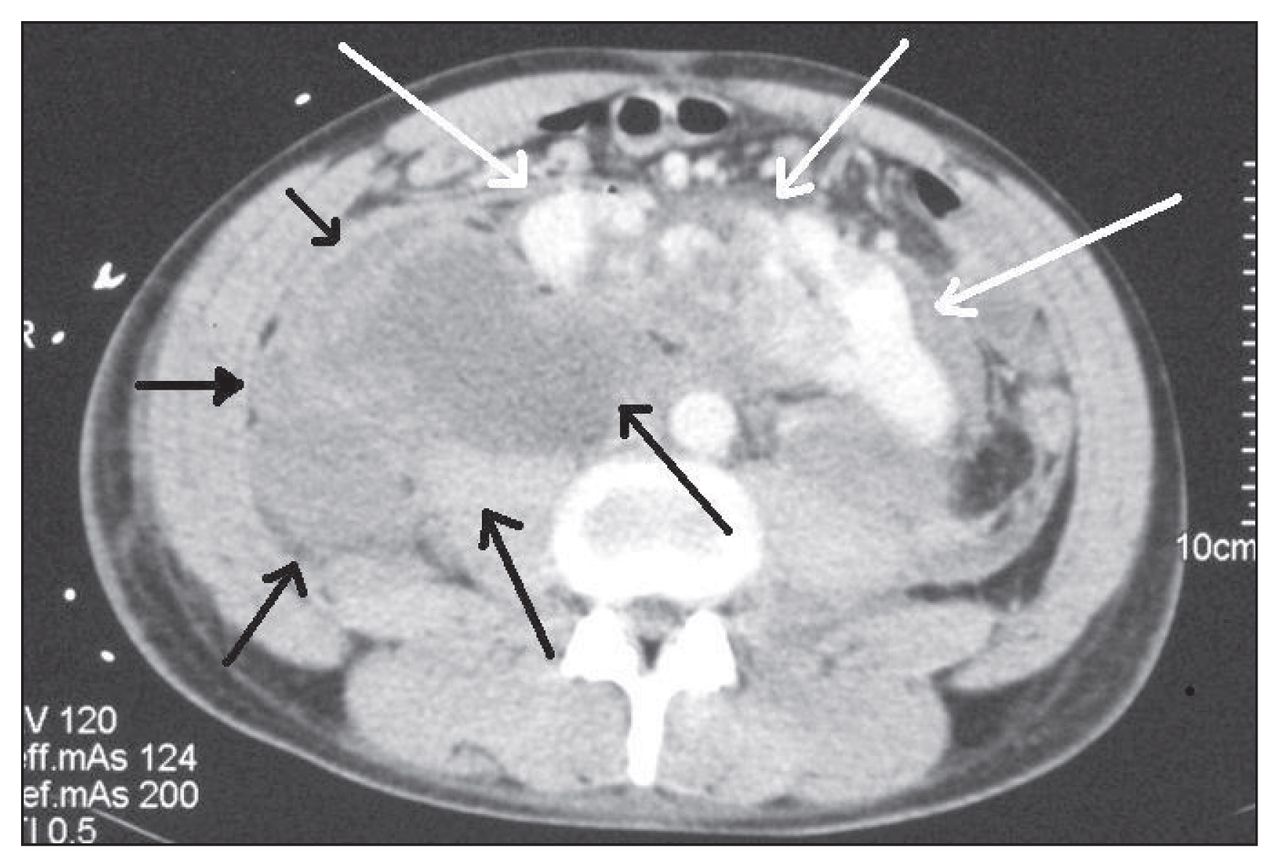
Internal fixation of the tibia fracture occurred the same day. Over the course of the next 5 days in the ICU, a transient elevation in serum creatinine without oliguria developed and resolved within 3 days, with return to a normal creatinine level. The patient showed no signs of hemorrhage and was discharged to the ward. From days 8 to 11 postinjury, he experienced progressive abdominal pain, ileus, shortness of breath, fever and oliguria. Sepsis was excluded with repeated cultures, including CT-guided aspiration of the hematoma. Additional CT imaging showed increasing volume of the retroperitoneal hematoma from liquefaction and swelling in the retroperitoneum, without additional signs of active bleeding (Fig. 3). His hemoglobin level remained stable. Anuria developed on day 11, which could not be explained by sepsis, systemic inflammatory response syndrome (SIRS), nephrotoxicity or shock. A large palpable mass that appeared tensed, corresponding to the retroperitoneal hematoma, could be easily felt and was painful on physical examination. Serum creatinine peaked to 631 μmol/L. The patient was brought to the operating room for laparotomy.
Coputed tomography scan with intravenous contrast showing the limits of the massive retroperitoneal hematoma (black arrows) and the injured horseshoe kidney (white arrows).
We found a very large retroperitoneal hematoma under pressure, and more than 3 L of clots were expelled from the perirenal space. Upon relieving the kidney, the coloration of the kidney improved and urine output resumed within the hour. The serum creatinine level returned to a normal value within 9 days. The patient did not require continuous renal replacement therapy or dialysis. We concluded that the systemic inflammatory response and renal failure were secondary to a compartment syndrome of the retroperitoneum caused by the large hematoma. The patient’s condition steadily improved, and he was eventually discharged home with normal renal function.
Discussion
The horseshoe kidney is a rare anomaly with an overall prevalence of 0.2%,1 with a higher prevalence in male patients. Two distinct kidneys are joined together by an isthmus almost always situated anterior to the aorta. Since its migration is often incomplete, the horseshoe kidney usually lies lower in the retroperitoneum. Vascularization is multiple and quite variable. In particular, the isthmus and adjacent parenchyma blood supply can come from the aorta or the renal, inferior mesenteric, common, internal, external iliac or sacral arteries.1
Blunt injury to the common iliac artery without associated pelvic fracture is uncommon.2 Rapid deceleration may cause avulsion of small arteries such as in our patient’s case with avulsion of a renal artery arising from the common iliac artery. Recent cases with a similar mechanism of injury were described with endovascular treatment by embolization3 or surgical management,4 but there was no complication related to the retroperitoneal hematoma.3,4
Endovascular treatment is emerging as interesting therapy in the trauma setting.2 We believe that in the case presented here, subclinical backbleeding from the lacerated polar artery stump of the right side of the horseshoe kidney contributed to the slow accumulation of blood in the retroperitoneum and the expansion of the size of the hematoma, leading to increased pressure and compartment syndrome in the retroperitoneum. To our knowledge, this is the first description of a retroperitoneal compartment syndrome affecting a horseshoe kidney in a traumatic arterial laceration treated with this approach. The kidney responded favourably and quickly to decompression of the compartment. Compartment syndromes of the renal space have been described in renal allograft compartments and are known to negatively affect the outcome of the surgery.5 In our patient’s case we had a similar demonstration, but it was traumatic. This complication should be considered in similar cases.
Footnotes
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.