


Splenosis is an autotransplantation of splenic tissue to an abnormal localization. It usually occurs after splenic rupture.1,2 Thoracic splenosis usually follows combined spleen and diaphragmatic injury.1,3,4 The average interval between initial trauma and discovery of thoracic splenosis is 21 years.2 We present the case of a patient with 3 intrathoracic masses accompanied by diaphragmatic hernia 25 years after thoracoabdominal trauma.
Case report
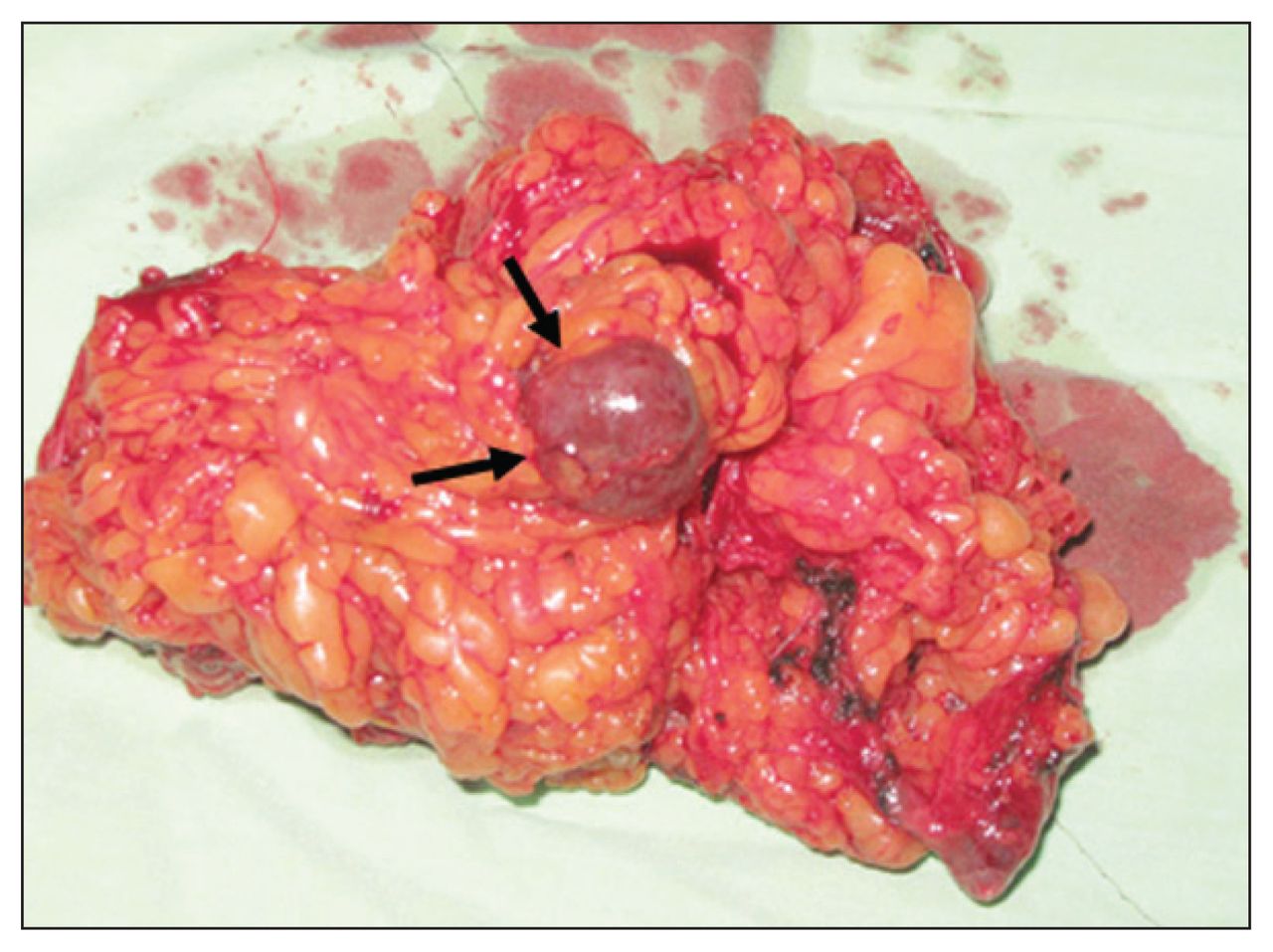
A 37-year-old woman presented with back pain, upper abdominal pain and a cough. She had sustained a gunshot wound to her abdomen 25 years previously. She had undergone surgery owing to the splenic injury, and 20 days later she underwent surgery for left-sided empyema. Physical examination revealed a thoracotomy scar on the left side, median laparatomy scar and decreased respiratory sounds in the left hemithorax. Her routine laboratory test results were normal. A chest radiograph showed a homogeneous mass 10 × 8 cm in size with regular contours in the left hemithorax above the diaphragm. A computed tomography (CT) scan of her thorax showed fatty tissue and a hyperdense lesion measuring 2–3cm (Fig. 1A). Another opaque lesion measuring 1 × 1 cm was located in the interlobar fissure (Fig. 1B). The third lesion was on the left pericardial side (Fig. 1C). We performed an exploratory thoracotomy for hernia repair and biopsy. We resected a piece of the omentum and closed the diaphragmatic defect (1 × 1.5 cm) primarily. In the omental fatty tissue, we discovered a piece (2 × 3 cm) of reddish-purple tissue (Fig. 2). In addition, we removed a similar lesion from the interlobar fissure. We diagnosed ectopic spleen. We did not remove the nodule near the pericardium because the mass was noted during retrospective investigations on the CT scan of her thorax.
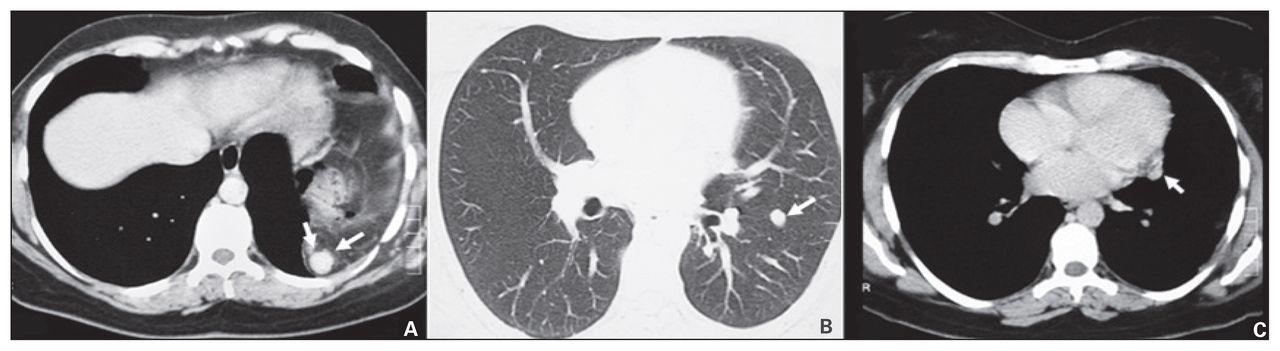
Computed tomography scan of the thorax of a 37-year-old woman showing fatty tissue as well as (A) a hyperdense lesion measuring 2–3 cm, (B) an opaque lesion measuring 1 × 1 cm located in the interlobar fissure and (C) a lesion on the left pericardial side.
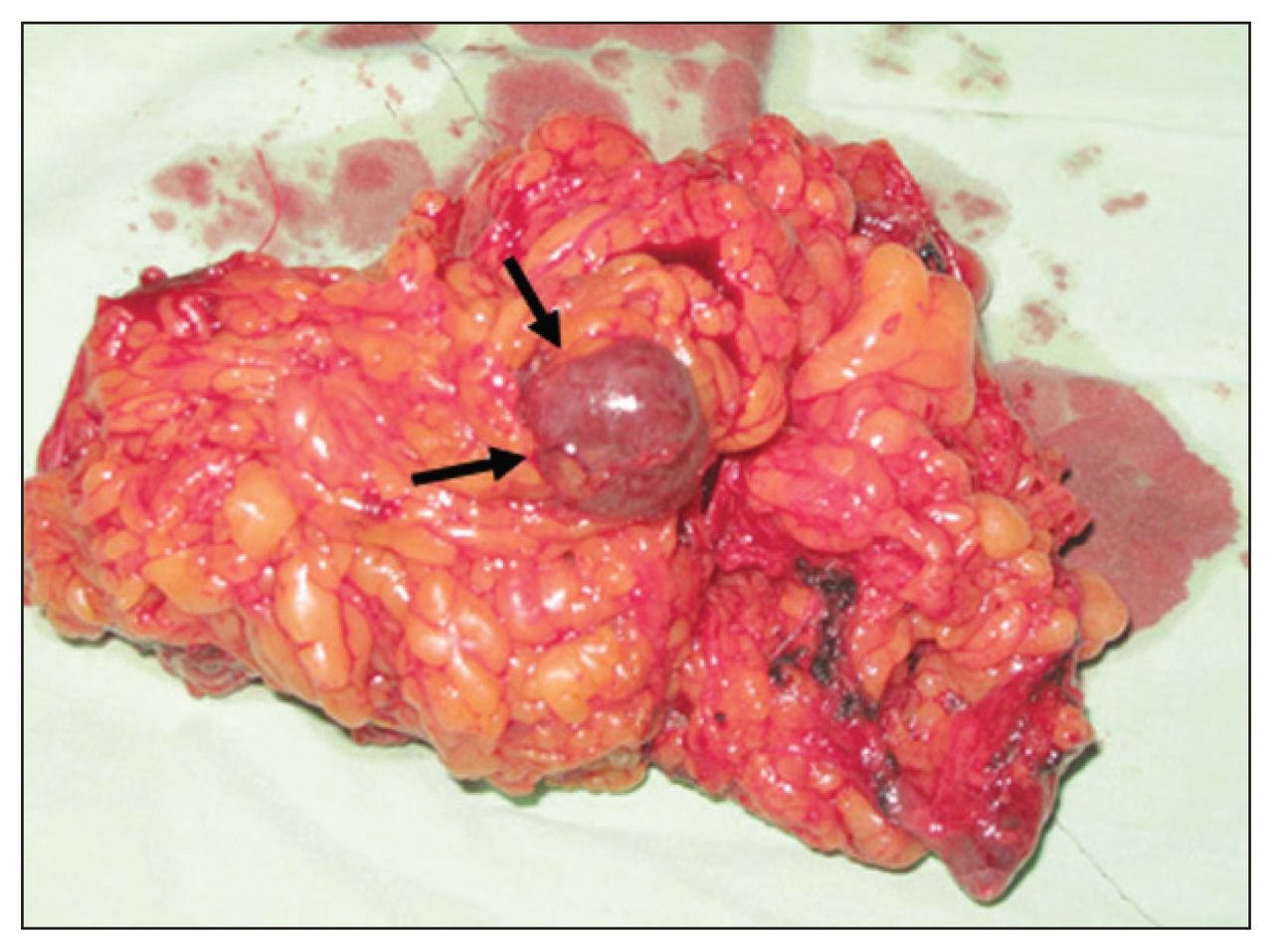
In the omental fatty tissue, we discovered a piece (2 × 3 cm) of reddish-purple tissue.
Discussion
Shaw and Shafi reported the first case of thoracic splenosis in 1937, and since then nearly 30 new cases have been reported in the literature.5 The basic pathogenesis of splenosis involves splenic implant onto the serosal surfaces with the aid of the reticulum cell of the adult spleen, which retains the potential for differentiation into the various splenic elements.4
Abdominal splenoses are usually accompanied by abdominal pain, intestinal obstruction, gastrointestinal bleeding and the recurrence of hematological disorders, but thoracic splenoses are usually asymptomatic and may be recognized as intrathoracic masses many years after a trauma, as was the case in our patient.1
Diagnostic investigations of thoracic splenosis have included CT of the thorax, radionuclide scanning, needle aspirations and needle biopsies.1 We only obtained a CT scan of our patient’s thorax. Initially, we detected only a diaphragmatic hernia and 2 nodules. During thoracotomy, the diaphragmatic defect was smaller than expected. Intra-operatively, the nodule in the omental tissue was similar to splenic tissue.
Intra-abdominal splenosis can be found in the splenic bed, omentum, peritoneal serosa, mesentery, serosal surface of the bowel, liver, diaphragm, pelvis and pelvic organs and subcutaneously at the site of the splenectomy incision.6 In our patient, we observed splenosis in the omental fatty tissue and in the fissure; however, we overlooked the splenosis in the pericardum.
In conclusion, intrathoracic splenosis should be considered in the differential diagnosis when patients present with intrathoracic nodular masses, especially on the left side, accompanied by a history of severe thoracoabdominal injury.
Footnotes
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.