


Abstract
Background: The incidence of hip fractures is increasing within the aging population. We investigated the overall rate of in-hospital mortality following hip fracture and how this mortality rate compares across academic and community hospitals.
Methods: We reviewed prospectively collected data from 17 hospitals in southern Ontario as part of a project to evaluate a new streamlined clinical care pathway developed for acute care of elderly patients with hip fractures. We collected demographic data, prefracture living status, acute care mortality and time to surgery, and we compared these data between community and academic hospitals.
Results: Between March 2007 and February 2008, 2178 consecutive patients were admitted with a hip fracture to 13 community and 4 academic hospitals. The mean age was 79 years and 72% were women. The overall in-hospital mortality rate was 5.0%, with no difference between patients treated in academic versus community hospitals (p = 0.56). We found a greater rate of acute care in-hospital mortality for patients admitted from dependent-living facilities compared with those who were living independently (risk ratio 0.63, 95% confidence interval 0.42–0.96).
Conclusion: Acute care in-hospital mortality following hip fractures remains high and is consistent across academic and community hospitals. With the rising incidence of hip fractures, we need to improve the models of care for these patients to reduce mortality and to maximize functional outcomes while maintaining efficient use of limited health care resources.
The incidence of hip fractures is increasing as the mean age of the population increases. This translates into a substantial burden on the health care system. The worldwide prevalence of hip fractures was estimated to be 1.26 million in 1990 and is predicted to rise to 6.3 million in 2050 owing to the aging population.1,2 In Canada, the direct health care cost of hip fracture care was estimated to be Can$650 million annually and is expected to rise to $2.4 billion annually by 2040.3 Hip fractures represent 67% of all lower limb fractures in Canadian hospitals among patients aged 65 years and older.4 Similarly, the incidence of hip fracture increases from 3% among women aged 65–74 years to 12.6% among women aged 80 years and older,5 while in white men the incidence ranges from 1%–2% among those aged 60 years and older.6,7 Thus, streamlining the care of patients with hip fractures to utilize health care resources efficiently is a major public health issue.
Hip fractures are associated with high morbidity and mortality despite advances in surgical and regional anesthesia techniques.8 Up to 50% of patients do not regain their prefracture functional status, as judged by their ability to walk and their need for ambulatory aids at home.9,10 Upwards of 25% of patients require a dependent residence or long-term care facility for a year or more after fracture.10,11 Similarly, mortality rates following hip fractures are high.12–16 At 1-month follow-up, reported mortality rates range from 6% to 9%,14,16,17 rising to 13%–19% at 3 months14,16–18 and 26%–33% at 1 year.11,13,14,16
Our primary objective in this study was to determine the overall rate of acute care and in-hospital mortality following hip fracture and how this mortality rate compares across academic and community hospitals in southern Ontario.
Methods
We reviewed data that were prospectively collected between March 2007 and February 2008 as part of a project designed to evaluate the introduction of a streamlined care pathway for patients with a unilateral hip fracture. All patients were taken to the operating room as soon as possible after being medically cleared for surgery, with the goal of less than 48 hours. The pathway suggests that patients should be transferred to inpatient rehabilitation by postoperative day 5 if they are medically stable, regardless of weight-bearing or cognitive status. A comprehensive 7- to 10-day assessment and treatment program is then used to determine the patient’s ability to return to their prefracture community settings after a 28-day stay at inpatient rehabilitation. The Community Care Access Centre provides support to transition these patients to return to the community after discharge.19 Alternatively, patients who require longer stays are transferred to a more appropriate care setting, such as complex continuing care or specialized geriatric services.
The original study collected data from 17 randomly selected hospitals across southern Ontario (4 academic and 13 community hospitals). The data set includes only patients aged 55 years and older with a femoral neck or intertrochanteric hip fracture.
Data collection
Data were collected prospectively in each hospital by an independent assessor and sent to our data monitoring team on a monthly basis. The data were stratified into 2 groups according to patient prehospitalization residential status (independent living [own home or retirement home] or long-term care facility [LTC] such as a nursing home). The data collected included time from admission to surgery, discharge destination and acute care in-hospital mortality. Time from admission to surgery was categorized as either less than or more than 48 hours. This cut point was selected because some studies have suggested that surgery performed less than 48 hours after admission to hospital is associated with a lower risk of mortality.14,20–22
Statistical analyses
We compared categorical data between groups using the Fisher exact test. We calculated risk ratios to evaluate the mortality rate among patients admitted from an independent living facility and those admitted from an LTC facility. A risk ratio less than 1 with a 95% confidence interval (CI) that does not cross the null value of 1 indicates a lower mortality rate among those admitted from an independent living facility. We analyzed the data using SPSS (version 12). All reported p values are 2-tailed with an α of 0.05.
Results
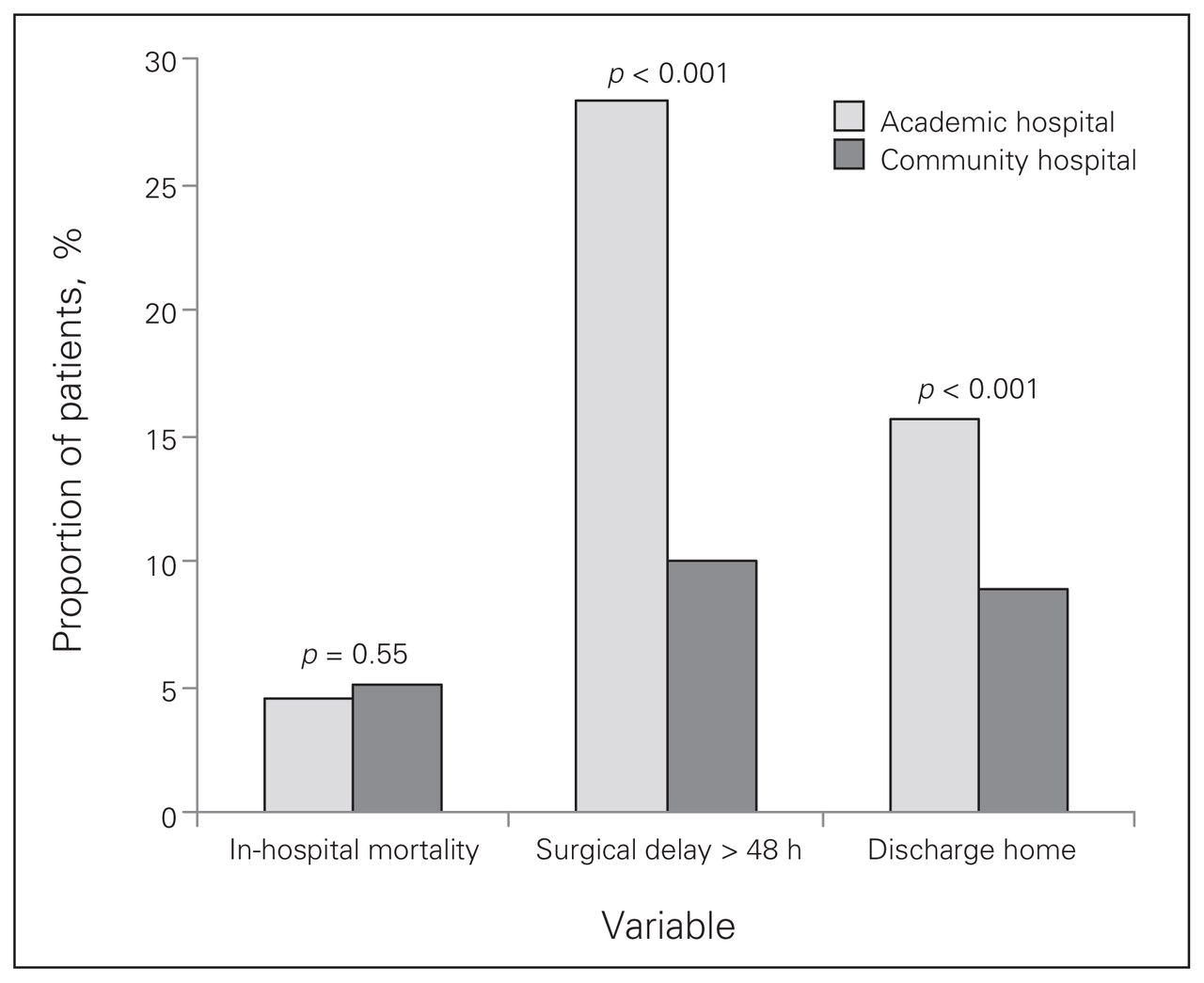
Over the 12-month study period, 2178 patients were admitted with a hip fracture to the participating 4 academic and 13 community hospitals. All patients were included in this analysis. In all, 473 patients (22%) received treatment in an academic hospital, and 1705 (78%) received treatment in a community hospital. The mean age was 79 years, and 72% were of patients were women. In total, 1767 patients (81%) were admitted from independent living, and 411 patients (19%) were admitted from an LTC facility. The overall in-hospital mortality rate was 5% (108/2178). There was no significant difference in the in-hospital mortality rate between patients admitted to academic hospitals (21/473, 4.4%) and those admitted to a community hospital (87/1705, 5.1%; p = 0.56). The mortality rate for patients admitted from an LTC facility was 7% (29/411), compared with 4% among patients admitted from independent living (79/1767; p = 0.038). The relative risk of death for patients admitted from independent living compared with those admitted from an LTC facility was 0.63 (95% CI 0.42–0.96).
In the community hospitals, 90% (1535/1705) of patients underwent surgery in less than 48 hours from the time of admission, compared with only 71% (339/411) of patients in academic hospitals (p < 0.001).
Overall, only 10% (225/2178) of the study population were discharged to independent living after surgery. Of these, 96% (216/225) were living independently before surgery. A comparison of discharge destination by hospital type showed that fewer patients from academic hospitals required referral to an LTC facility or an in-patient rehabilitation centre (399/473, 84%) compared with patients from community hospitals (1554/1705, 91%; p = 0.001).
Figure 1 shows the in-hospital mortality, timing to surgery and discharge destination by hospital type.

In-hospital mortality, surgical delay and percentage of patients discharged home from academic and community hospitals following hip fracture.
Discussion
This study reviews the timing to surgery, mortality rates and discharge destinations of 2178 consecutive patients with hip fractures from 17 hospitals in southwestern Ontario between March 2007 and February 2008. We found an overall rate of acute care mortality of 5.0%, with no significant difference between community and academic hospitals. Patients who were living independently at the time of injury had a significantly lower risk of acute care in-hospital mortality than those living in an LTC facility. This is consistent with what others have reported previously.11,17,23
In-hospital mortality has been reported to range from 4% to 10% and has consistently been shown to be significantly greater in men than women.13,24–29 In Ontario, the overall in-hospital mortality rate was estimated to be about 7%, and it was significantly higher among men than women.22,30 This higher mortality rate among men appears to be a constant finding at 1 month, 3 months, 6 months and 12 months following surgery, even after adjustment for relevant potential confounding variables.20,31 Our mortality rate of 5.0% is on the lower end of the reported rates and may reflect the benefit of our model of care, which emphasized early mobilization and assessment of patient needs. This included a comprehensive geriatric assessment and delirium-prevention strategies.
Some studies discriminate between mortality rates based on whether the fracture is intracapsular (femoral neck) or extracapsular (intertrochanteric). A few studies have reported an increased mortality rate for intertrochanteric fractures compared with femoral neck fractures,32,33 whereas another showed a higher mortality rate in patients with femoral neck fractures.34 However, most studies have shown no difference;15,16,25,35 therefore, we collapsed all types of hip fractures into 1 group.
Interestingly, we found that a high percentage of patients required referral to in-patient rehabilitation or an LTC facility, which increases the cost of caring for patients with hip fractures compared with patients discharged to independent living.36 Of the 1767 hip fracture patients who were admitted from independent living, only 216 (12%) patients were discharged directly back to independent living from acute care. The high rate of patient referral to LTC and in-patient rehabilitation facilities may be related to a lack of unified criteria and indications for referral to these health care facilities.
Comorbidity and mortality following hip fracture
There are many conflicting data about the association between comorbidity and mortality following hip fracture. Factors such as reduced mental status, dementia, low physical ability before injury, chronic heart or pulmonary diseases and diabetes have been suggested to predict greater mortality following hip fracture.25,32,35 Other studies suggest that an American Society of Anesthesiologist classification score of 3 or 4 is associated with a higher mortality rate.33 In a prospective study, Cornwall and colleagues34 followed 537 patients with hip fractures and showed that only greater patient age and preinjury physical disability were independently associated with increased mortality following hip fracture. Patient-level comorbidity data were not available in this study. Most of the reports mentioned above were retrospective and did not have a control group.
Other authors have used control groups of a general population without hip fracture to compare mortality rates and identify predictive factors for increased mortality.35 Katelaris and Cumming37 compared the mortality rate in hip fracture patients with that in a matched control group without hip fractures and concluded that, although the mortality rate was significantly higher in the fracture group, the difference was not explained by prefracture comorbidity. Similarly, other controlled studies have found that preoperative comorbidity is not a predictor of mortality after hip fracture.15,38
Hospital model of treatment
Different hospital models of care have been examined for their effect on mortality following hip fracture. A hospitalist system, in which a dedicated hospital-based physician provides total medical care to fracture patients, was tested against routine care; this study found no benefit of a hospitalist system on in-hospital or 1-year mortality.23,39 Other reports have shown a substantial reduction in 30-day mortality, from 22% to 7%, after implementation of a specialized team responsible for the complete care of patients with hip fractures in hospital.40 However, it should be noted that a 22% mortality rate is substantially higher than any other reports in the literature and is higher than our 5% mortality rate.
Studies comparing medical care at academic and community hospitals in the United States have reported that mortality rates for hip fracture patients are lower in academic hospitals.41,42 In Ontario, one report found that care of patients with hip fractures in academic hospitals was associated with significantly lower in-hospital mortality rates compared with nonacademic hospitals.22 We found an absolute risk reduction in mortality of 0.7% for those treated in the academic hospitals; however, this was not statistically significant.
Timing of surgery and mortality
Many studies consider a delay in surgical treatment of more than 2 days to be a predictive factor for poorer functional outcomes and to also increase short- and long-term mortality rates following hip fracture.14,20–22 Other studies have reported no association between a delay in surgical treatment and mortality rates.23,39,43,44 A recent systematic review and meta-analysis concluded that an operative delay of more than 48 hours is associated with increased short- and mid-term mortality rates following hip fracture.45 They further suggested that the studies reviewed may be limited by the potential for residual confounding. Furthermore, a delay in surgery may have substantial effects on length of hospital stay, time to mobilization and, therefore, total cost of care.23,29,39,44 We did not have patient-level data that would allow us to compare mortality rates by timing of surgery.
We acknowledge that this study has several limitations. Our comparisons between groups were not adjusted for potentially confounding factors such as age, sex or comorbidity. Individual patient-level data were not available to allow us to perform this analysis. Our study has several advantages including a large, consecutive series of patients from 17 health care centres ranging from high-volume academic centres to general community centres. Because we have a large sample size and we included all patients with hip fractures during the study period, we feel there is limited selection bias in our study. Moreover, with our large sample size, these potentially confounding variables such as age and sex are likely to be balanced between hospital types.
Conclusion
We found an overall in-hospital mortality rate of 5.0%, with no difference between community and academic hospitals. The relative risk of in-hospital mortality was significantly greater for those admitted from an LTC facility compared with those who were living independently. With the rising incidence of hip fractures, improved models of care for these patients will be critical for maximizing functional outcomes while maintaining efficient use of limited health care resources.
Footnotes
Competing interests: None declared.
Contributors: All authors helped design the article and approved it for publication. Dr. Alzahrani acquired the data, Dr. Gandhi analyzed it, and they wrote the article together. Drs. Alzahrani, Davis and Mahomed reviewed the article.
- Accepted October 11, 2009.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.