


Abstract
Background: Theory suggests the uptake of a medical innovation is influenced by how potential adopters perceive innovation characteristics and by characteristics of potential adopters. Innovation adoption is slow among the first 20% of individuals in a target group and then accelerates. The Quality Initiative in Rectal Cancer (QIRC) trial assessed if rectal cancer surgery outcomes could be improved through surgeon participation in the QIRC strategy. We tested if traditional uptake of innovation concepts applied to surgeons in the experimental arm of the trial.
Methods: The QIRC strategy included workshops, access to opinion leaders, intra-operative demonstrations, postoperative questionnaires, and audit and feedback. For intraoperative demonstrations, a participating surgeon invited an outside surgeon to demonstrate optimal rectal surgery techniques. We used surgeon timing in a demonstration to differentiate early and late adopters of the QIRC strategy. Surgeons completed surveys on perceptions of the strategy and personal characteristics.
Results: Nineteen of 56 surgeons (34%) requested an operative demonstration on their first case of rectal surgery. Early and late adopters had similar perceptions of the QIRC strategy and similar characteristics. Late adopters were less likely than early adopters to perceive an advantage for the surgical techniques promoted by the trial (p = 0.023).
Conclusion: Most traditional diffusion of innovation concepts did not apply to surgeons in the QIRC trial, with the exception of the importance of perceptions of comparative advantage.
Researchers suggest that the uptake of a medical innovation depends on how potential adopters perceive the characteristics of the innovation, the characteristics of the potential adopters and contextual factors that act as barriers or facilitators to the diffusion of the innovation.1 Characteristics of an innovation that can reportedly influence uptake (e.g., use of a new drug) are comparative advantage, compatibility with adopter values, complexity of use and ability to observe or trial use of the innovation.2,3 Characteristics that can reportedly differentiate early and late adopters, respectively, include higher resource levels, a cosmopolitan nature, higher education levels and a more positive attitude.4 Other research suggests that the rate of innovation adoption is slow among the first 20% of individuals in a target group and then accelerates.4–6 Figure 1 presents a typical diffusion of innovation curve.6

Classic diffusion of an innovation curve.1
There is a remarkable paucity of quantitative data supporting the above concepts on clinical innovation adoption in the medical realm. Most papers commenting on the uptake of medical innovations are theoretical or rely on survey or qualitative data.5,7–11 Such studies do not correlate survey or interview results with actual rates of innovation uptake. We could find only 1 relevant medical study with quantitative data that measured rates of uptake of a medical innovation among individual physicians concurrently with diffusion of innovation factors.12
The Quality Initiative in Rectal Cancer (QIRC) trial tested if patient outcomes could be improved at the hospital level by encouraging surgeons to adopt the QIRC strategy.13 The QIRC strategy was designed to ensure that surgeons provide high-quality total mesorectal excision surgery. Total mesorectal excision is superior to traditional methods of rectal surgery, but it is more technically challenging.14 The QIRC strategy interventions included a workshop, access to opinion leaders, intraoperative demonstrations, a postoperative questionnaire, and audit and feedback.
While the QIRC trial was negative — results were similar in both arms of the trial — we tested if traditional uptake of innovation concepts applied to surgeons in the experimental arm of the trial. For experimental arm surgeons, we used the timing of surgeon participation in an intraoperative demonstration to differentiate early and late adopters of the QIRC strategy. We assessed the rate of innovation uptake as well as relevant surgeon perceptions and characteristics. In accordance with traditional uptake of innovation concepts, we hypothesized that uptake of the QIRC strategy would accelerate only after 20% of surgeons had adopted the innovation and that early and late adopters of the QIRC strategy would have different perceptions and characteristics.
Methods
The QIRC trial
We have reported the methods and primary results of the QIRC trial previously.13,15 Briefly, we cluster-randomized 16 Ontario hospitals and their respective groups of surgeons to the QIRC strategy (i.e., 8 experimental arm sites with 56 surgeons) versus no intervention (i.e., 8 control arm sites with 49 surgeons). The primary study outcomes were rates of permanent colostomy and local tumour recurrence. The trial was closed after 1015 patients were enrolled.
The QIRC strategy involved 5 interventions: workshops, intraoperative demonstrations, access to opinion leaders, postoperative questionnaires, and audit and feedback. Workshops reviewed surgical techniques and principles of quality improvement. During the workshops, participating surgeons selected a local opinion leader using a validated methodology.16 For the intraoperative demonstrations, a participating surgeon could invite another surgeon to the operating room to demonstrate total mesorectal excision techniques. The postoperative questionnaire was designed to prompt surgeons to re-examine key intraoperative steps of total mesorectal excision. Hospitals were the unit of study randomization. It is thus important to emphasize that individual surgeons in the experimental arm were free to use any or none of the QIRC strategy interventions. In addition, patients in control arm hospitals received no interventions, and thus data from this group are not relevant to the current assessment of innovation uptake.
Study groups: defining early and late adopters of the QIRC strategy in the intervention arm
For the 56 experimental arm surgeons, we used participation in an intraoperative demonstration to differentiate early and late adopters of the QIRC strategy. While we considered all 5 of the strategy interventions important, we hypothesized that a request for an intraoperative demonstration required the greatest change in traditional practice. Such a demonstration involved the entry of an outside surgeon (i.e., operative demonstrator) being invited into the home operating theatre of a participating surgeon. The participating surgeon and support staff in the operating room would all be aware that the operative demonstrator was in attendance to demonstrate a potentially improved method of rectal surgery. By extension, this raised the possibility that the provision of rectal surgery to date by the respective surgeon could be perceived as suboptimal. For statistical robustness, we decided a priori that early and late adopters would be divided into 2 approximately equal-sized groups based on the timing of requests for a demonstration.
Data sources
Study team notes and completion of patient accrual
The study team recorded surgeon consent rates, timing and participation in workshops, intraoperative demonstrations and completion of postoperative questionnaires. Data on the number and timing of rectal cancer surgeries performed by all surgeons and on the number and timing of requests for an intraoperative demonstration were available.
Surgeon survey
At the completion of patient accrual, experimental arm surgeons were mailed a survey related to the QIRC trial. The survey was pilot tested for readability and comprehensiveness by surgeons from hospitals not involved in the QIRC trial. We used the Dillman method of repeated requests to maximize survey response rates among surgeons.17 Respondents were given the option to identify themselves or to remain anonymous. Subjective responses were scored on a 5-point Likert scale.
Study end points
Participation rates
We calculated rates of consent and participation in workshops, postoperative questionnaires and operative demonstrations. We measured rates of participation in the intra-operative demonstrations overall (i.e., x% of surgeons requested a demonstration) and by time (e.g., x% of surgeons requested a demonstration by their third case of rectal cancer surgery). We did not measure participation in the opinion leader or in the audit and feedback intervention, since all sites selected an opinion leader and feedback was mailed to all surgeons.
Surgeon perceptions of total mesorectal excision and the QIRC strategy
From the surveys, we gathered data on the following surgeon perceptions: 1) comparative advantage of total mesorectal excision versus traditional techniques and of the QIRC strategy interventions versus other continuing education initiatives, and of the surgical techniques promoted by the QIRC strategy versus pretrial techniques; 2) compatibility with values of total mesorectal excision with a desire to cure patients; and 3) complexity of total mesorectal excision as a surgical technique and of participation in the overall QIRC strategy and the intraoperative demonstration intervention. These are the key perceptions thought to drive adoption of innovation.1–4
Surgeon characteristics
We collected data on the following surgeon characteristics: year of graduation; resource levels (i.e., hours of operating room and endoscopy time); cosmopolitan nature (i.e., attendance at regional and national or international surgical meetings); willingness to adopt other surgical innovations (i.e., laparoscopic surgery for colon surgery); and positive attitude (i.e., attitude to health care in Ontario and the direction of colorectal cancer surgery care in Ontario). Such characteristics have been found in other areas to predict rates of adoption of an innovation.1,4,6
Statistical analyses
We used descriptive and univariate (unadjusted) analyses of study end points. We used the Mann–Whitney U and Fisher exact tests for continuous and categorical variables, respectively. The criterion for statistical significance was set at α = 0.05. Since these analyses were primarily exploratory to generate hypotheses, we did not adjust the overall level for multiple testing. Five-point Likert scale survey responses were categorized as negative (score of 1 or 2), neutral (score of 3) or positive (score of 4 or 5) to assist with interpretation and analyses. We performed sensitivity analyses by repeating relevant analyses after excluding data from surgeons who began working at study hospitals after the initiation of the trial, since we surmised that such surgeons would be less likely to participate in all aspects of the study. All analyses were performed using SPSS version 16. The Ethics Review Board of the Hamilton Health Sciences Centre/McMaster University approved the protocol.
Results
Overall participation rates
The consent rate for the trial was 96 of 105 (91%) surgeons for both arms of the trial, and 51 of 56 (91%) and 45 of 49 (92%) in the experimental and control arms, respectively. Consenting surgeons treated 97% of the study population. At the 8 experimental arm sites, 39 of 56 (70%) surgeons attended a workshop, 40 of 56 (71%) surgeons requested an operative demonstration, and 44 of 56 (79%) surgeons completed at least 1 postoperative questionnaire. The 40 surgeons who requested an operative demonstration treated 86% of the patients accrued in the experimental arm.
Uptake of operative demonstrations and defining early and late adopters of the QIRC strategy
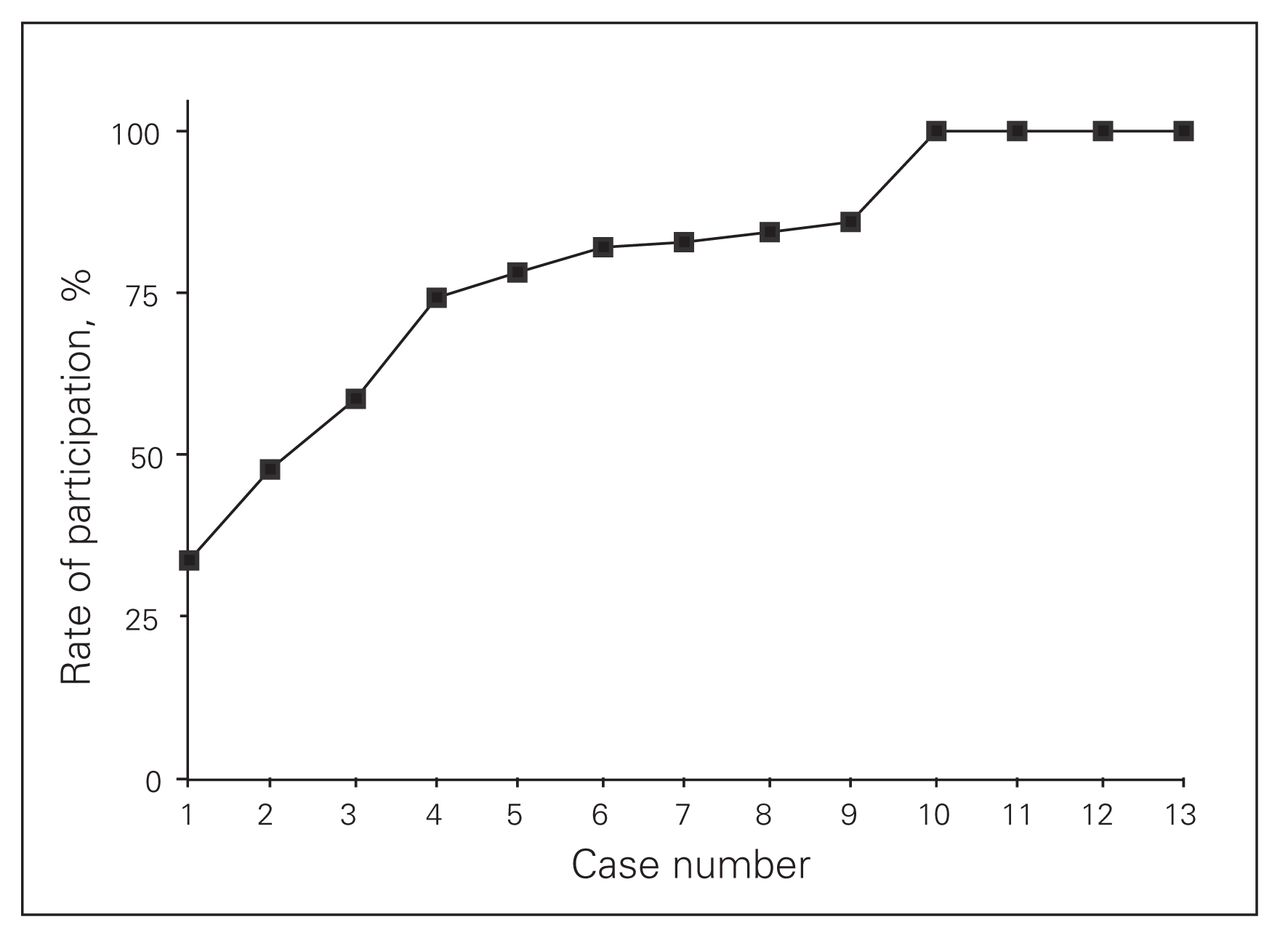
The curve for uptake over time for the operative demonstrations is presented in Figure 2. Nineteen of 56 (34%) surgeons requested an operative demonstration on their first case of rectal cancer surgery after site randomization. By the fourth case (i.e., the fourth potential opportunity for participation), 75% of surgeons had requested an operative demonstration, and by the tenth case the participation rate was 100%.

Curve for uptake over time for the operative demonstrations.
Among the 56 experimental arm surgeons, early adopters requested an operative demonstration on their first or second case of rectal cancer surgery. Thus, late adopters requested an operative demonstration only after their second case of rectal cancer surgery or not at all. This followed our a priori decision to create 2 approximately equal-sized groups based on timing of participation in the operative demonstration intervention. The resulting 27 early and 29 late adopters performed 52% and 48% of all cases in the experimental arm, respectively.
Comparing early and late adopters of the QIRC strategy
QIRC strategy participation rates
For the 56 experimental arm surgeons, there were marked differences in rates of participation for the 27 early versus 29 late adopters. The participation rates for early and late adopters, respectively, were 100% and 83% (p = 0.024) for trial consent, 89% and 52% (p = 0.003) for the workshops, 100% and 45% (p < 0.001) for intraoperative demonstrations, and 89% and 69% (p = 0.07) for completion of a postoperative questionnaire (Table 1).
Percentage of participation in QIRC strategy interventions for early and late adopters
Survey participation rates
Thirty-three of 56 (59%) surgeons returned a completed survey, and 2 of them wished to remain anonymous. We therefore compared survey results for 18 early and 13 late adopters of the operative demonstration. These 31 surgeons performed 65% of all experimental arm cases.
Perceptions of total mesorectal excision and the QIRC strategy
There were few differences between early and late adopters in their perceptions of total mesorectal excision surgery or the QIRC strategy (Table 2). For comparative advantage, 83% and 69% of early and late adopters, respectively, rated the QIRC strategy as more effective than other continuing medical education activities (p = 0.30), and 78% and 80%, respectively, perceived an advantage of total mesorectal excision versus traditional surgical techniques (p = 0.31). The 1 difference in perceived comparative advantage was that 18% and 62% of early and late adopters, respectively, reported no improvement with the techniques promoted in the QIRC trial versus the respective surgeon’s pretrial techniques (p = 0.023). For compatibility with values, 90% of respondents overall indicated that total mesorectal excision was more compatible than traditional techniques for achieving cure. For complexity, 90% of surgeons found their personal involvement in the QIRC trial to be not at all burdensome.
Surgeon perceptions of total mesorectal excision and the QIRC strategy*
Surgeon characteristics
There were no differences between early and late adopters in median year of graduation, resource levels (i.e., hours of operating room and endoscopy time), cosmopolitan nature (i.e., frequency of attendance at regional, national or international meetings), willingness to adopt other surgical innovations (i.e., laparoscopic surgery for colon surgery) and positive attitude (i.e., attitude to health care in Ontario and attitude to the direction of colorectal cancer surgery care in Ontario; Table 3). For example, 56% and 62% of early and late adopters, respectively, had attempted a laparoscopic colon resection (p = 0.74), while 56% and 85% had a positive opinion on the current direction of colorectal cancer surgery in Ontario.
Surgeon characteristics
Discussion
Our results from a substudy of a randomized surgical trial do not support traditional diffusion of innovation concepts. The rate of uptake of the operative demonstrations — a proxy for the entire QRC strategy — occurred more quickly than expected. Instead of uptake accelerating only after a 20% adoption rate threshold, a remarkable 34% of surgeons requested a demonstration at the first opportunity. In addition, early and late adopters had similar perceptions of the QIRC strategy and similar surgeon characteristics. These observations, if corroborated in other surgical areas, have important implications for stakeholders interested in the appropriate uptake of surgical innovations or new techniques. Overall, surgeons should not be viewed as a source of resistance to innovation uptake, and traditional characteristics differentiating individual adoption patterns in other areas may not apply to surgeons.
Early and late adopters of the operative demonstrations had similar perceptions of the QIRC strategy and of total mesorectal excision surgery, with 1 exception: late adopters were more likely than early adopters to perceive no advantage for the surgical techniques promoted by the strategy compared with their pretrial techniques (62% v. 18%, p = 0.023). Early and late adopters did feel that total mesorectal excision techniques were superior to traditional techniques. Thus, on average, late adopters likely accepted the advantage of total mesorectal excision techniques, but were confident they were already optimally providing such techniques before the QIRC trial. It is logical that late adopters of an innovation would perceive relatively less advantage than early adopters for the techniques promoted by the QIRC strategy. These findings also mesh with those from a survey study of laparoscopic surgeons in the Netherlands.11 Participants were asked to provide responses on factors that influenced their adoption of laparoscopic techniques for various procedures. Additional benefit was the strongest predictor of uptake, with technical factors playing a minor role.
Of note, rates of local recurrence and permanent colostomy — the primary outcomes of the QIRC trial —did not vary between early and late adopters. This was expected given similar outcomes in both arms of the overall QIRC trial; participation in the QIRC strategy did not lead to improved patient outcomes; thus, one would not expect that early or late adoption of a noneffective intervention would result in improved patient outcomes.
Our findings on surgeon perceptions of the QIRC strategy have implications for quality improvement efforts.18 We hypothesize that in the face of persistent quality gaps stakeholders may wish to target clinician perceptions of the comparative advantage of the intended practice change. The production and effective presentation of high-quality evidence demonstrating the advantage of specific practice changes may be an efficient initial focus of quality improvement. As well, if clinicians perceive a comparative advantage for a particular practice and there is still slow adoption, then related quality gaps should not be attributed to recalcitrant clinicians, but rather to other barriers to optimal care.
Most research on factors driving the uptake of medical innovations involves surveys or qualitative interviews.7–11 Results are not correlated with the actual uptake rate of an innovation, or quantitative data, as was done in the present study. In the 1 study we could identify that measured diffusion rates among individual clinicians, the uptake of a new antibiotic (i.e., tetracycline) among family physicians was rapid and followed a curve remarkably similar to the uptake curve seen in the present study.12 Both studies provide limited evidence that rapid medical practice change can occur. The paucity of rigorous diffusion of innovation studies that contain quantitative data precludes a conclusion that this is the norm for adoption of clinical innovation. We encourage related research.
Limitations
There are limitations to the present study. First, some may not consider participation in an intraoperative demonstration as the uptake of a medical innovation. However, as discussed, a request for an intraoperative demonstration required a marked change in traditional surgeon practice and was completely voluntary. In addition, our a priori rules to identify early and late adopters based on timing of an operative demonstration did result in 2 groups with significantly different rates of participation in other parts of the QIRC trial, including trial consent, attendance at workshops and completion of postoperative questionnaires. Second, the study relied on data from a small number of surgeons and survey responses. But the hospitals involved in the QIRC trial treat an estimated 25% of all patients with rectal cancer in Ontario (population 13 million), and the 31 surgeons who completed study surveys performed 65% of the cases in the experimental arm.15 Thus, survey responses likely represent perceptions and characteristics among a large percentage of surgeons treating rectal cancer patients in Ontario. As well, it is important to reiterate that there is an incredible paucity of quantitative data correlating the uptake of clinical innovations with the personal characteristics or perceptions of the involved clinicians. Finally, we did not account for multiple testing. But as discussed in the Methods section, we considered the present study to be mainly hypothesis-generating. We believe that sharing our results with the wider community is important given the current lack of quantitative data on the diffusion of surgical innovations.
Conclusion
Overall, traditional diffusion of innovation concepts did not apply to surgeons in the QIRC trial, with the exception of perceptions of comparative advantage. Our findings should be quantitatively tested in other clinical areas and among other physician groups.
Acknowledgements
We gratefully acknowledge the expertise and time that our operative demonstrators provided during the course of the trial. We also thank the generous support of the surgeons, administrative staff and departments at our participating hospitals, including Credit Valley Hospital, Humber River Regional Hospital — Mississauga Site, Joseph Brant Memorial Hospital, Niagara Health System — Niagara Falls Site, Niagara Health System — St. Catharines Site, North Bay General Hospital, North York General Hospital, Rouge Valley Health System —Centenary Site, St. Joseph’s Health Centre — Sudbury Site, The Scar-borough Hospital — Grace Site, Southlake Regional Hospital, Thunder Bay Regional Health Sciences Centre, Toronto East General Hospital, Trillium Health Centre — Mississauga Site, William Osler Hospital —Brampton and Etobicoke Sites.
Footnotes
Competing interests: None declared.
Contributors: M. Simunovic, A. Coates, A. Smith, C.H. Goldsmith, L. Thabane and M.N. Levine designed the study. M. Simunovic, A. Coates, C.H. Goldsmith and L. Thabane acquired the data. Data analysis and interpretation was done by M. Simunovic, A. Coates, C.H. Goldsmith, L. Thabane and M.N. Levine, who also wrote the article. All authors reviewed and approved the final version for publication.
Funding: Canadian Institutes of Health Information (MCT-50013).
- Accepted December 19, 2012.
In this issue

{kind=link}
{kind=link}
Article tools





