


Abstract
Background: Emergency general surgery (EGS) services are gaining popularity in Canada as systems-based approaches to surgical emergencies. Despite the high volume, acuity and complexity of the patient populations served by EGS services, little has been reported about the services’ structure, processes, case mix or outcomes. This study begins a national surveillance effort to define and advance surgical quality in an important and diverse surgical population.
Methods: A national cross-sectional study of EGS services was conducted during a 24-hour period in January 2017 at 14 hospitals across 7 Canadian provinces recruited through the Canadian Association of General Surgeons Acute Care Committee. Patients admitted to the EGS service, new consultations and off-service patients being followed by the EGS service during the study period were included. Patient demographic information and data on operations, procedures and complications were collected.
Results: Twelve sites reported resident coverage. Most services did not include trauma. Ten sites had protected operating room time. Overall, 393 patient encounters occurred during the study period (195/386 [50.5%] operative and 191/386 [49.5%] nonoperative), with a mean of 3.8 operations per service. The patient population was complex, with 136 patients (34.6%) having more than 3 comorbidities. There was a wide case mix, including gallbladder disease (69 cases [17.8%]) and appendiceal disease (31 [8.0%]) as well as complex emergencies, such as obstruction (56 [14.5%]) and perforation (23 [5.9%]).
Conclusion: The characteristics and case mix of these Canadian EGS services are heterogeneous, but all services are busy and provide comprehensive operative and nonoperative care to acutely ill patients with high levels of comorbidity.
General surgical emergencies are common. They may account for 25%–50% of a general surgeon’s overall workload and 7% of all hospital admissions.1,2 In 2006, the Institute of Medicine declared nontrauma surgical emergencies as one of the main stressors on emergency departments in the United States.3 Patients facing surgical emergencies are often critically ill with numerous comorbidities. Timely, comprehensive intervention can prevent devastating long-term complications.3 Traditionally, on-call surgeons have been required to balance emergency surgical care with a busy elective subspecialty service, including rounds with elective patients, visiting patients within clinic and daytime subspecialty operating.
In Canada, there has been a trend toward consolidating emergency general surgery (EGS) into dedicated services.1,2 Emergency general surgery services have been implemented with the intent of providing a dedicated hospital-based service specifically for the care of general surgical emergencies.4,5 This allows comprehensive care to be provided while also creating stronger platforms for quality improvement and optimization of resource use. There are limited data on the overall case mix of these novel EGS services and their varied structures, processes and outcomes.6–8 The emergence of EGS systems represents an opportunity to understand and improve processes of care that serve this complex, resource-intensive surgical population. More research is required on the true acuity, complexity and diversity of EGS services and systems, as well as on the roles these services play in supporting surgical rescue within acute care health systems.
This study captures a snapshot at a single point in time of both the case mix and workflow during a typical day in EGS across Canada. We hypothesized that Canadian EGS services face highly acute, complex, diverse case mixes and that service models have evolved in unique ways in response to specific requirements within their local environments. Shared insights about case mix and service delivery will inform the next generation of developments in quality improvement and health system design.
Methods
Design
The Canadian Association of General Surgeons formed the Acute Care Committee from a group of surgeons providing trauma and EGS care across Canada. This inclusive committee outlined a road map for multicentre EGS research, starting with an environmental scan of EGS services across the country. Such a study creates a strong foundation for future clinical and systems studies in EGS, characterizes future participating sites, identifies opportunities for collaboration, helps to disseminate best practices and serves as a gap analysis to identify new research directions. Many members of the committee are EGS site leaders, which was an advantage for study design, institutional review and data acquisition. The protocol for this cross-sectional study was approved by the ethics review board at the study lead site (Vancouver General Hospital) and subsequently at each of the participating hospitals.
Service structure
A survey of EGS service leaders was used to characterize the structure of different services at each of 14 hospitals across 7 provinces in Canada (Fig. 1). Site leads were asked to complete a database sheet to describe key features of their EGS services. Examples of structural features include the use of a “surgeon of the week” model, the presence of a dedicated EGS service, the availability of protected operating room time for EGS cases and the ability to use EGS operating room time for elective cases. Site leads were also asked whether all general and subspecialty surgeons participated and about the involvement of resident coverage, the inclusion of trauma patients and the existence of a formalized handover process between surgeons at shift change.
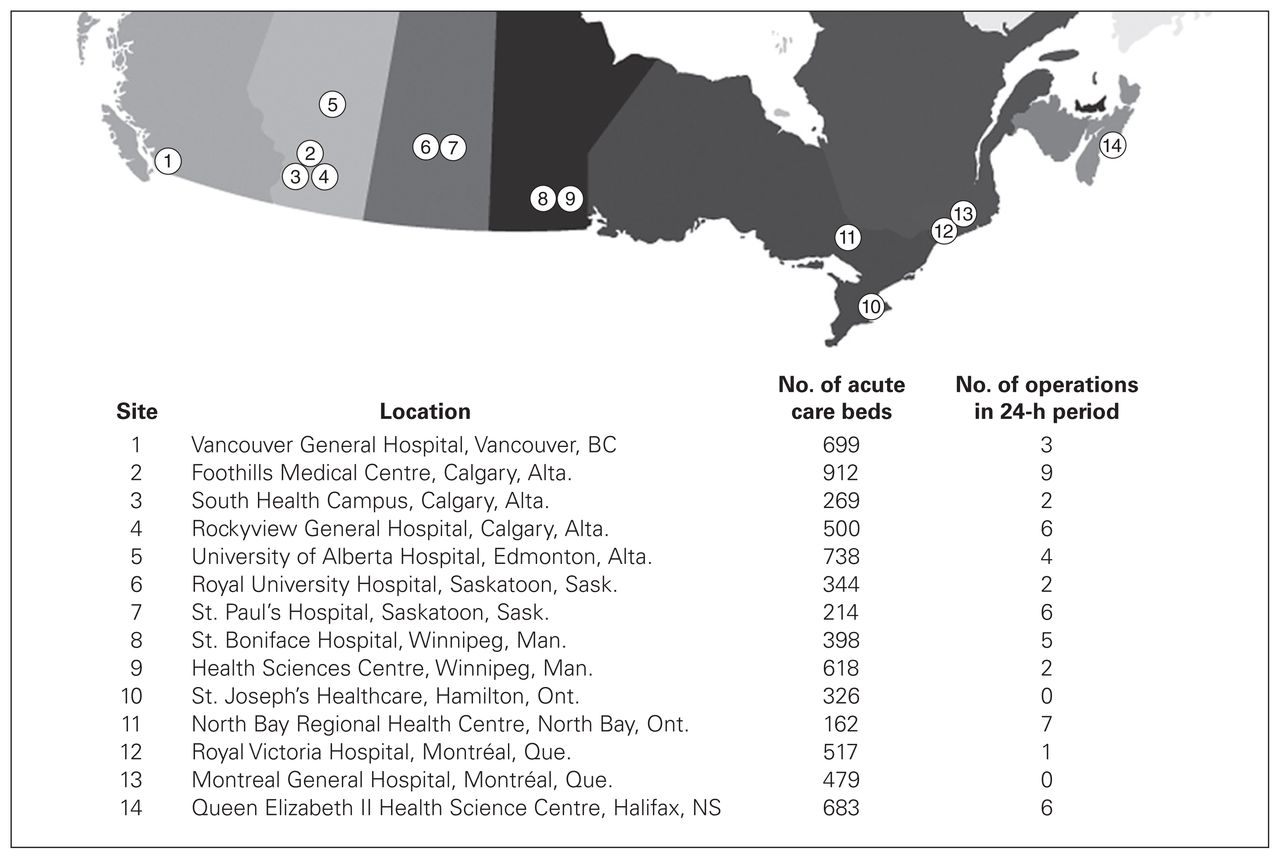
Participating sites.
Case mix
Patients assessed by EGS services at participating sites on Jan. 10, 2017, formed the study cohort, and the EGS teams on call from 7 am on Jan. 10, 2017, to 7 am on Jan. 11, 2017, were briefed about the protocol. Patients currently admitted to the EGS service, new consultations and offservice patients (admitted to the hospital but not under the direct care of an EGS service) being following by the EGS service during the 24-hour study period were included in the study. Trauma patients and patients discharged from the EGS service before 7 am on Jan. 10, 2017, were excluded.
Participating sites collected data using standardized case report forms and a summary sheet (Appendix 1, available at canjsurg.ca/013517-a1). Data were collected by study personnel at each site under the supervision of the site lead (coauthors of this paper), and the primary author or the site lead entered the data. Patient demographic information such as age, sex, comorbidities and previous operations was collected, as were all operative and procedural data, and data on intraoperative and postoperative complications. Data were verified with the site leads individually, and all perceived discrepancies and questions were resolved in a second round of communication with all sites.
Data analysis
Site leads tabulated data from the case report forms and summary sheets, and these were merged in Microsoft Excel version 15.18. Subsequently, basic statistics were conducted and condensed into tables.
Results
Service structure
Emergency general surgery services across Canada reported using different structural models for the delivery of care (Table 1). All participating sites had a dedicated EGS service with a “surgeon of the week” model, whereby 1 surgeon suspends his or her elective practice for an entire week to focus on EGS patients during the day, sharing overnight call responsibilities. Ten sites (71%) had protected operating room time, and 6 (43%) were permitted to use protected time for elective cases. In contrast to the situation in the US, where trauma and EGS are often combined in single services,9,10 only 4 Canadian sites (29%) included trauma patients under the scope of EGS services. Twelve sites (86%) reported resident coverage, and all had a formal handover process.
Description of emergency general surgery service structures and processes across Canada
Case mix
A total of 393 patients were assessed across the 14 sites during the study period. The EGS service was newly consulted to assess 112 patients, of whom 76 (67.8%) were admitted by the EGS service within the 24-hour period (Table 2). Of patients previously admitted to the EGS service, 40 (13.0%) were cared for in an intensive care unit setting, and 10 (3.2%) had open abdomens. Emergency general surgery teams operated in 53 cases during the study period, 28 (53%) of which were completed laparoscopically. When considering all patients on the EGS census, 195 cases (50.5%) were operative (Table 3). Of the operative cases, 88 (44.9%) were laparoscopic, with a conversion rate of 5.7%. There was 1 intraoperative complication across all sites. A total of 109 (57.1%) of the nonoperative cases were managed with antibiotic regimens.
Cohorts of emergency general surgery patients, by hospital service
Summary of operative and nonoperative management of emergency general surgery patients by hospital service*
The mean patient age was 59.1 (standard deviation 4.9) years, and 186 (47.3%) were female. Most patients assessed by the EGS service had complex conditions: 207 (52.7%) had 1–3 comorbidities, and 136 (34.6%) had more than 3 comorbid conditions (Table 4). In addition, there was a wide range of presenting problems and final diagnoses evaluated and managed by EGS teams (Table 5). The most common diagnoses were gallbladder disease (69 patients [17.8%]), gastric/intestinal obstruction (56 [14.5%]) and appendiceal disease (31 [8.0%]). The diagnoses that most increased the average length of stay in hospital were neoplasms, pancreatic disease and intestinal obstruction.
Age, sex and comorbidity status of emergency general surgery patients, by hospital service
Case mix and resource use as reflected by duration of hospital stay at the time of the study
Discussion
This study represents a unique snapshot of the complex care that is provided on an average day at EGS services across 14 Canadian hospitals. Consequently, it provides a novel perspective of a large, complex, resource-intensive patient population, for which limited reporting exists within the literature.1,9
The development of EGS services in Canada emerged organically as a way to address the growing complexity of EGS. Implementing these services has highlighted aims to improve access to care, patient outcomes and safety, while enhancing efficiency of service delivery, surgeon satisfaction and educational opportunities.11 As shown by the variation in models adopted at the 14 participating sites, hospitals have created services structured to meet these objectives based on their local context. The number of surgeons within a department, diversity in the continuum of learners at a site, proximity of tertiary trauma care, and executive administration and financial support are a few potential factors that can affect the organization of an EGS service. The unpredictable pace of emergency surgery has made protected operating room time an important part of delivering timely, safe care. However, our findings suggest that there remains a gap in providing allocated time to emergency general surgeons. Furthermore, autonomy in deciding how unused resources are assigned is lacking.
Most studies on EGS have focused on processes and outcomes for appendicitis and cholecystitis.8,12–14 Although these conditions account for a substantial part of the activity of EGS services, they do not reflect the breadth, intensity or resource consumption of a modern EGS practice. In our national EGS sample, appendicitis and cholecystitis together accounted for only 26% of patients and only 10% of hospital stays. In contrast, cancer accounted for close to 23% of hospital days and, therefore, a considerable portion of EGS service activity.
Our findings confirm that Canadian EGS services are complex. EGS service team members not only provide operative care but also manage complicated nonoperative cases. Nationally, 49% of patients were managed nonoperatively, with the Montreal General Hospital site having the highest number of patients receiving nonoperative care. Although these patients often require several resource-intensive days in hospital, their care is not well documented in the EGS literature. The present study shows an opportunity for research that aims to understand and improve the processes and outcomes of care for EGS patients managed nonoperatively.
The complexity of EGS may, in part, be reflected by the extent of comorbidities and the frequent need for critical care. At 1 service, 72% patients had more than 3 comorbid conditions. The fact that all of these patients had been considered for, or had undergone, major emergency operations is evidence that EGS services bear the responsibilities not only of assessment, diagnosis and resuscitation but also of preoperative optimization, operative intervention and postoperative care. This care is delivered to vulnerable patients with complex medical conditions over rapid time frames. Furthermore, the fact that 13.0% of patients in our study were cared for in the intensive care unit shows the critical status of many EGS patients. This intersection of aggressive surgical care and patients with complex medical conditions is a daily reality on modern EGS services. Consequently, these services provide an opportunity for multicentre quality improvement, guideline development and promotion of best practices. There is an urgent need for the next generation of EGS research to explore the intricacies of service delivery more fully.
The implications of a national EGS research network are far-reaching. Our study shows that EGS patient populations are large, complex and resource intensive, and that the structures and processes of EGS care are variable. A national EGS research network will be able to share experiences and define best practices and will serve as a forum to make these experiences and best practices more universal. The network has already defined a research and quality-improvement road map, with the next series of studies underway. Future studies will focus on processes of care, complex operative care, determinants of complications and death, benchmarks of quality and surgical education in EGS. It is hoped that ultimately this work will lead to a national EGS database and research strategy dedicated to analyzing diversity in the Canadian EGS experience. With that national initiative, the structure, processes and outcomes of EGS service delivery can be optimized.
Strengths and limitations
This study was a one-time snapshot of 24 hours of care by EGS services at major Canadian hospitals. It was an observational project that did not capture every hospital with or without a formalized EGS service (mostly owing to difficulty in identifying these services and engaging them in a national study) and therefore could not provide a comprehensive view of Canadian EGS practice. However, despite its methodological limitations, the study is proof of the concept that it is possible to bring emerging EGS services and patient-level insights into a national research network. The fact that the study was completed rapidly shows that national collaboration on research protocol development, coordination of ethics review board applications, creation of data-sharing agreements, and shared data analysis, interpretation and reporting are highly feasible.
Conclusion
Canadian EGS services are at the centre of Canadian acute care. They are busy intake services for extremely vulnerable patients with a spectrum of complex, life-threatening conditions including abdominal sepsis, intestinal obstruction and cancer. Emergency general surgery services optimize perioperative and operative care along rapid timelines and often use nonoperative approaches as well. They act as rescue services, supporting patient care on other services, and frequently provide care in intensive care units. Ongoing national research collaborations will continue to shed light on the structures, processes and outcomes of these important new services and will identify new opportunities to improve patient care and system performance.
Acknowledgements
The authors thank the Canadian Association of General Surgeons Acute Care Committee for participating in this study and volunteering their hospital data and research staff to help make this project possible. The authors acknowledge Jillian Aquino for her design and creation of the figure.
Footnotes
Competing interests: None declared.
Contributors: K. DeGirolamo, K. D’Souza, S. Apte, C.G. Ball and S.M. Hameed designed the study. All authors acquired the data, which K. DeGirolamo, K. D’Souza, S. Apte, C.G. Ball and S.M. Hameed analyzed. K. DeGirolamo, K. D’Souza, S. Apte, C.G. Ball and S.M. Hameed wrote the article, which all authors reviewed and approved for publication.
- Accepted November 17, 2017.
In this issue

{kind=link}
Article tools





