


Abstract
Background: Barriers exist in implementing enhanced recovery after surgery (ERAS), which aims to decrease postoperative complication rates and length of stay, because perioperative care is varied and compliance from a multidisciplinary team is critical to success. The objectives of this project were to evaluate the effectiveness of the National Surgical Quality Improvement Program (NSQIP) database as a tool for the ongoing assessment of outcomes associated with ERAS and to evaluate ERAS as a quality-improvement strategy at a hospital-wide level.
Methods: Adult patients who underwent an elective colorectal procedure at The Ottawa Hospital between March 2010 and September 2015 were included. Information on demographic characteristics, functional status, medical background, procedure details and hospital length of stay (LOS) was abstracted from the NSQIP database. We compared data on outcomes (LOS, postoperative complications, unplanned return visits to the emergency department and 30-day mortality) before and after ERAS.
Results: We analyzed data for 609 patients (318 [52.2%] colon resection, 291 [47.8%] rectal resection; 190 [31.2%] before ERAS, 419 [68.8%] after ERAS). Significantly more patients were discharged within 5 days of surgery after ERAS than before (43.5% v. 29.1%, p < 0.05), and LOS more than 10 days was also reduced (23.7% v. 24.9%, p < 0.001). Implementation of ERAS was associated with an absolute reduction of 12% in postoperative complications and a significant reduction in surgical site infections among patients who underwent open procedures (p = 0.04).
Conclusion: The introduction of an ERAS program for monitoring standardized perioperative care facilitates a data-driven approach to guide implementation of practice guidelines and establish the sustainability of ERAS protocols and data collection processes.
Enhanced recovery after surgery (ERAS) refers to goal-directed, multimodal perioperative interventions that, when implemented together, aim to decrease perioperative stress, improve pain management, alleviate gastrointestinal dysfunction and minimize postoperative complications.1–7 Enhanced recovery after surgery programs have also been shown to reduce the surgical patient’s length of stay (LOS).8–11 The benefits of ERAS are well-documented and supported in research settings, and an increasing number of academic and community hospitals across Canada are transitioning to standardizing perioperative care according to ERAS guidelines. However, the process of implementing ERAS programs represents a current weakness in reproducing the outcomes described in the literature. Several barriers are encountered in implementing ERAS programs given that perioperative care is varied and that compliance from a multidisciplinary team is critical to the success of the program.12 The ongoing assessment of performance and outcomes is therefore critical to the success of ERAS uptake. However, measuring improved outcomes outside the context of a clinical trial is challenging. This emphasizes the value of access to reliable data to guide efforts in the implementation and uptake of ERAS guidelines.
The Council of Academic Hospitals of Ontario funded an ERAS implementation program that was put into practice at 15 academic hospitals in Ontario. The implementation was based on an ERAS guideline developed by the Best Practice in General Surgery Group at the University of Toronto. As part of this initiative, the group develops clinical practice guidelines, which can be accessed by stakeholders and surgeons via a free online platform of knowledge translation for successful implementation of ERAS parameters.7 The Best Practice in General Surgery Group provides an “off-the-shelf” model to facilitate quality improvement.13 In other words, the group’s ERAS guidelines were created so that they are easily and immediately accessible online and do not require special modifications to be successfully implemented within individual hospitals. The American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) is another widely recognized quality-improvement program. It is a leading, nationally validated, risk-adjusted database containing information on surgical outcome measures that can be collected for all surgical cases.14 The NSQIP collects surgical data on 135 clinical variables, including preoperative risk factors, intraoperative variables, and 30-day postoperative mortality and morbidity outcomes for patients undergoing major surgical procedures.15 Participating sites can track surgical complications through the ACS NSQIP database to evaluate the quality of their surgical programs and use collected data to measurably improve surgical outcomes.16–18 The ACS NSQIP database is therefore a useful tool for data collection, monitoring and analysis for quality improvement of surgical outcomes. The NSQIP is currently implemented in 61 hospitals across Canada, with 28 of these in Ontario.
Given the increasing uptake of ERAS in hospitals across Ontario, we questioned whether the ACS NSQIP database offers potential as an accessible, reliable and comprehensive tool to monitor and evaluate various outcomes in the setting of ERAS. The primary objective of the present study was to compare postoperative outcomes including LOS and complications for patients undergoing elective colorectal procedures before and after implementation of ERAS using surgical outcome data collected in the ACS NSQIP. Secondary objectives included showing the feasibility of the use of the ACS NSQIP and identifying challenges and opportunities associated with ERAS.
Methods
Study design
This study was an observational quality-improvement project conducted at The Ottawa Hospital (TOH). The hospital has been participating in the ACS NSQIP since 2010, with 100% of data on colorectal cases collected since March 2014. A total of 934 patients are included in the data set through September 2015. Preoperative through 30-day postoperative data are collected and entered online on the Web-based ACS NSQIP platform on an ongoing basis.
Setting
The design of the present study capitalized on the participation of TOH Department of General Surgery with both ERAS guidelines and the ACS NSQIP database. The ACS NSQIP database was introduced to TOH campuses in March 2010. As part of the ERAS initiative funded by the Council of Academic Hospitals of Ontario, TOH implemented a hospital-wide ERAS program beginning in September 2013 for all patients undergoing colorectal surgery. The interventions outlined in the council’s ERAS clinical pathway for colorectal surgery include preoperative information and counselling, reduced fasting duration, mechanical bowel preparation, prevention of surgical site infection, thromboprophylaxis, intraoperative fluid management, avoidance of prophylactic abdominal drains, avoidance of prophylactic nasogastric tubes, early mobilization, postoperative fluid management, early enteral feeding, use of chewing gum to reduce postoperative ileus and multimodal pain control (e.g., thoracic epidural anesthesia, lidocaine infusion, nonsteroidal anti-inflammatory drugs, acetaminophen and gabapentin). These guidelines are summarized in detail in Supplementary Table S1, Appendix 1 (available at canjsurg.ca/003518-a1). Data for this study reflect the period of introduction of the ACS NSQIP database, in March 2010, and a 2-year period after implementation of ERAS, collected with the ACS NSQIP database from September 2013 to September 2015.
Patient selection
Given that all the patients were treated according to the standard of care at TOH as well as the minimal risk to patient confidentiality, this study was considered a quality-improvement project under the Ottawa Health Science Network Research Ethics Board, which approved the study protocol to be conducted with waived consent. All adult (age ≥ 18 yr) patients who underwent an elective colorectal procedure (e.g., left or right hemicolectomy, total colectomy, sigmoid colon resection, segmental colon resection) between March 2010 and September 2015 were included. Patients who had an emergency admission and surgery were excluded, given that they were unable to benefit from the preoperative teaching and preparation components central to the ERAS program. Patients who underwent pelvic exenteration were also excluded, on the basis that this surgery involves extensive multivisceral resection and recovery may not be comparable to that with other procedures. Given that transanal excision is often performed as a day procedure, patients who underwent this procedure were also excluded from analysis.
Data sources and outcome variables
Patients were identified through the institution’s Performance Metrics (Health Records). Information on the included patients’ demographic characteristics, functional status, medical background, procedure details and hospital stay was abstracted from the ACS NSQIP database. We defined duration of hospital LOS as the total number of days spent in hospital from the surgery date until the discharge date. All categories were defined by ACS NSQIP standard definitions. We defined the occurrence of complications as a patient’s having experienced any of the complications recorded by the ACS NSQIP (Supplementary Table S2, Appendix 1). We recorded postoperative outcomes based on ACS NSQIP category, including LOS, postoperative complications (number and severity), unplanned return visits to the emergency department and 30-day mortality rate.
At the outset of implementing ERAS, we targeted an “ideal” LOS of 5 days or less.18 We also noted that patients staying more than 10 days were more likely than those with shorter stays to experience complications or have social issues limiting the ability to be discharged home, as has been previously reported.19 For this reason, we identified 3 categories for LOS: 1–5 days (ideal), 6–10 days and more than 10 days (“extended”). Our objective was to increase the number of patients discharged within 5 days.
Statistical analysis
We used descriptive statistics to describe the demographic, preoperative and operative characteristics of the study population. We used 2-sample t tests to examine differences in the means for continuous variables comparing the pre- and post-ERAS periods, and analyzed for outcomes pertaining to open procedures only and ERAS. We used additional comparisons, including χ2 tests, Wilcoxon rank-sum tests and analysis of variance with post-hoc Tukey honestly significant difference testing, as appropriate. We fit multiple logistic regression models to evaluate the association between ERAS and clinical outcomes, adjusted for potential confounding factors. We calculated the outcomes involving postoperative complications for all types of laparoscopic procedures only. All analyses were carried out with Stata v.15 (StataCorp).
Results
A total of 934 colorectal cases were collected between March 2010 and September 2015, of which 325 were excluded (300 with emergency admission and surgery, 22 with pelvic exenteration and 3 with transanal excision). The remaining 609 cases (318 [52.2%] colon resection and 291 [47.8%] rectal resection) were included in the data set for analysis. A total of 190 patients (31.2%) underwent resection before ERAS, and 419 (68.8%) had resection during or after ERAS. There were no significant differences in baseline demographic or clinical characteristics between the 2 cohorts except for mean surgery duration, which was longer in the post-ERAS group than in the pre-ERAS group (309.0 min v. 281.8 min, p = 0.008) (Table 1).
Baseline demographic and clinical characteristics of patients who underwent colorectal surgery before and after implementation of the enhanced recovery after surgery program
Hospital length of stay
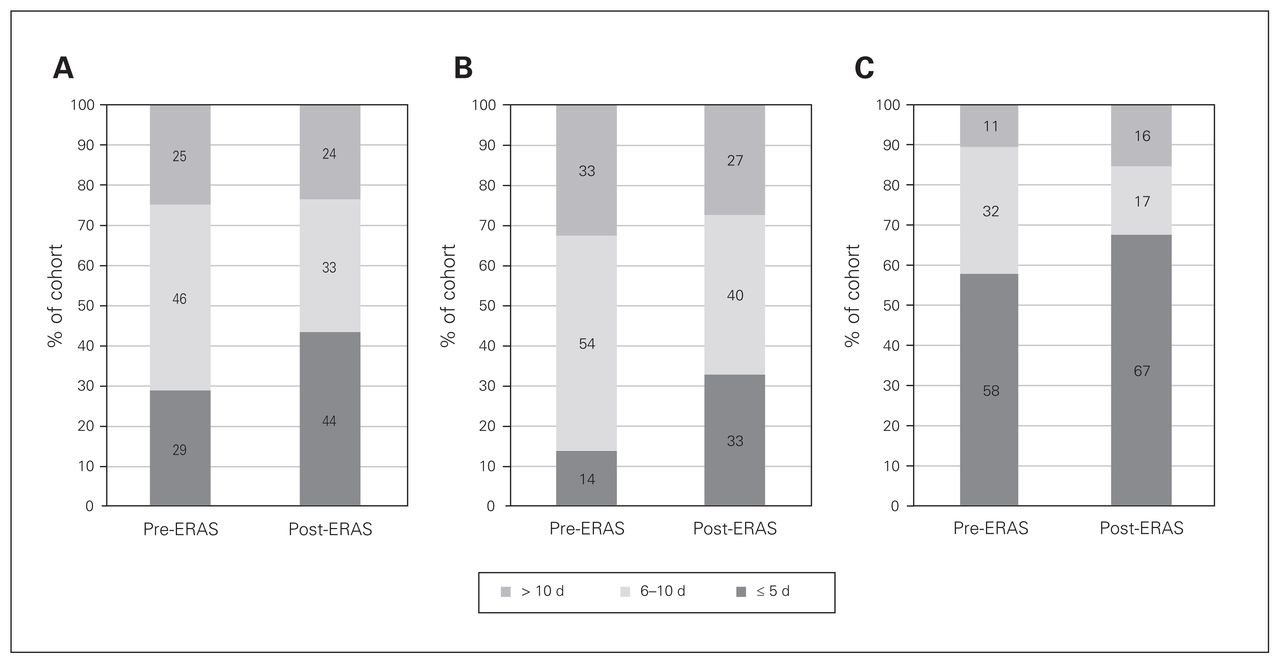
The observed distribution across all LOS categories was significantly different between patients who underwent surgery before and after implementation of ERAS (p = 0.001) (Fig. 1). A median LOS of 7 days (interquartile range 5–10 d) was observed before ERAS, compared to 6 days (interquartile range 4–10 d) during or after ERAS (p = 0.048) (Supplementary Fig. S1, Appendix 1). The proportion of patients discharged between 6 and 10 days was significantly reduced after ERAS (32.8% v. 46.0%, p < 0.001), and the proportion of patients discharged within 5 days of surgery was significantly increased (43.5% v. 29.1%, p < 0.05). Length of stay of more than 10 days was also significantly reduced (23.7% v. 24.9%, p < 0.001). After adjustment for complications, age and sex, ERAS status was associated with reduced odds for LOS 6–10 days (odds ratio 0.44, 95% confidence interval 1.52–3.77) and more than 10 days (odds ratio 0.16, 95% confidence interval 4.53–12.31) compared to the target reference LOS of less than 6 days. Similar findings were reflected for open surgical procedures only (Fig. 1, B), where there was an increase in the proportion of patients discharged within 5 days, from 13.8% in the pre-ERAS group to 32.9% in the post-ERAS group, (p < 0.001). Similarly, the proportion of patients discharged between 6 and 10 days was reduced, from 53.7% before ERAS to 39.8% after ERAS (p < 0.001).
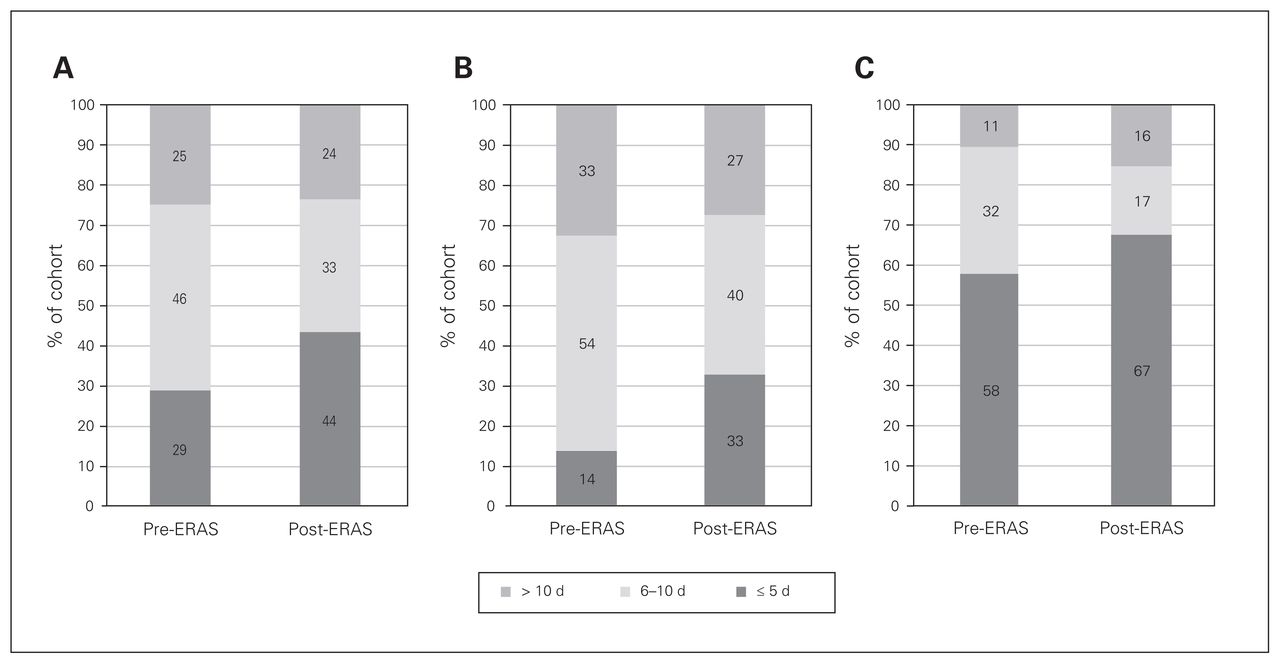
Hospital length of stay among patients who underwent colorectal surgery before and after implementation of the enhanced recovery after surgery (ERAS) program. (A) Entire cohort. (B) Patients who had open procedures. (C) Patients who had laparoscopic procedures.
Postoperative complications
The distribution of complication rates is shown in Table 2. There was a significant absolute reduction of 12% in the proportion of patients in the overall cohort with postoperative complications after ERAS compared to before ERAS (p = 0.004) (Fig. 2, A). Similarly, there was a significant absolute reduction of 10% in the proportion of patients who underwent open procedures and had postoperative surgical site infections after ERAS compared to before ERAS (24.8% v. 34.7%, p = 0.04) (Fig. 2, B). There was no difference in postoperative urinary tract infections before ERAS versus after ERAS among patients who underwent open procedures. Among patients who underwent laparoscopic procedures, there was no statistically significant differences in postoperative complications before ERAS versus after ERAS (Fig. 2, C). A multivariable regression model evaluating outcomes among patients who underwent open procedures showed an absolute reduction of 12% in postoperative complications in the post-ERAS group compared to the pre-ERAS group (p < 0.001).

Postoperative complication rates before and after implementation of the enhanced recovery after surgery (ERAS) program. (A) Entire cohort. (B) Patients who underwent open procedures. (C) Patients who underwent laparoscopic procedures.
Postoperative outcomes before and after implementation of the enhanced recovery after surgery program
Return visits to emergency department and death
There was no significant difference in the number of unplanned return visits to the emergency department after hospital discharge between the pre-ERAS and post-ERAS periods (p = 0.2) (Table 2). Thirty-day mortality was also similar between the 2 periods (p = 0.5).
Discussion
Using ACS NSQIP data, we compared surgical outcome rates before and following implementation of a provincially standardized ERAS program and found a significant reduction in LOS among patients who underwent elective colorectal surgery, with improved overall morbidity when ERAS guidelines were followed. The proportion of patients with LOS of 6–10 days before ERAS was shifted to LOS of 5 days or less in the post-ERAS period. The implementation of ERAS made little impact on patients requiring a LOS beyond 10 days after either open or laparoscopic colorectal surgery. Importantly, we found that there was no significant increase in the number of unplanned return visits to the emergency department related to the reduced LOS in the post-ERAS period.
The implementation of ERAS protocols is widely credited for reducing hospital LOS after colorectal surgery.3,5,7,20–22 Consistent with previous reports,23–25 we observed that, following ERAS, there was an increase in the proportion of patients discharged within 5 days. Although we have attributed the shift toward an earlier discharge to the ERAS program, there are other factors that may have been responsible, at least in part, for this finding, including a shift in the procedures performed or in the demographic characteristics of the patients seen. However, there were no significant differences in body mass index, functional status, preoperative comorbidities or ASA class between our pre-and post-ERAS cohorts. Moreover, the proportion of patients who underwent rectal (as opposed to colon) surgery, had a laparoscopic procedure and recovered with a new ostomy was similar between the 2 periods (34.7% pre-ERAS and 30.8% post-ERAS). Interestingly, the observed reduction in LOS was reflected in patients who underwent open procedures but not laparoscopic procedures. This may suggest that TOH had already been carrying out practices consistent with enhanced recovery, whereas ERAS protocols had more of an impact in standardizing perioperative approaches in open surgical procedures. Given that all the colorectal surgeons at TOH perform both open and laparoscopic procedures, it is unlikely that the observed differences observed are a reflection only of specific surgeons’ preferred approach to perioperative care.
An important observation in this analysis, as well as a primary goal of the ERAS program, was a reduction in rates of surgical site infection among patients undergoing colorectal surgery. Surgical site infections are a common complication after surgical procedures and are associated with increased morbidity and health care costs.26 We found that ERAS was successful in decreasing surgical site infection rates for open procedures. However, the observed reduction was modest, and this is an area that still warrants quality initiatives to achieve desired outcomes.
One unexpected finding in our study was an increased mean duration of surgery of roughly 30 minutes after ERAS. This may be explained by several changes in operating room protocols that were implemented concomitantly with the transition to ERAS, such as preoperative briefing periods, completion of 3-part checklists and closing tray protocols, all of which may have contributed to the increase seen in operating room time. There are several enhanced recovery programs, such as ERAS, that exist and share common elements including patient education and preoperative planning, preoperative carbohydrate loading, improved analgesic techniques to reduce the physical stress of the operation, early oral feeding and mobilization.23,27,28
Before ERAS, information regarding outcomes related to implementation of enhanced recovery programs was limited. Inconsistencies within this research area have also been observed as a result of inadequate data quality and insufficient data quantity.29 This highlights the importance of using an effective and accurate tool to monitor outcomes following the implementation of an ERAS program. Our methodology shows the effectiveness of off-the-shelf, evidence-based perioperative protocols. The protocols for ERAS used for this quality-improvement project at TOH are multidisciplinary, easily accessible (available at www.bestpracticeinsurgery.ca/guidelines/general-surgery), cost-effective and modifiable based on specific hospital preferences or standards.
Finally, our findings support the utility and effectiveness of the ACS NSQIP as a data collection tool for improved surgical outcomes.10,30–32 Furthermore, the NSQIP has been adopted by many hospitals across Canada.18 However, it is important to note that data collected via the NSQIP are only as good as their source of documentation. To address this limitation, we recently introduced an ERAS-NSQIP module to supplement outcome data with compliance data as a method to assess adherence with ERAS. The goal of this module is to track compliance with ERAS guidelines (Supplementary Table S1, Appendix 1) in order to further identify barriers and target potential areas for improvement. We believe that this module is promising to see further improvements in perioperative care. At the same time, however, through the current project, we have realized that quality-improvement efforts such as ERAS rely heavily on point-of-care documentation by engaged members of the team, often nursing. Engagement of our nurses in the development of documentation requirements has been paramount in improving accurate recording of compliance with ERAS metrics. The ERAS-NSQIP platform is a highly valuable tool for implementing and measuring more innovative improvements in perioperative care quality with continuous audit and feedback.
Conclusion
Evidence-based approaches to perioperative care should improve the value of delivery of health care services in Ontario by increasing quality while reducing costs. Improved collection and reporting of how enhanced recovery programs are implemented, resourced and experienced are an important component in the success of these programs. Continuous reassessment of surgical outcomes and collection of process quality indicators is an important step in determining implementation gaps and identifying practice changes that require ongoing support. The introduction of an ERAS-NSQIP module for monitoring standardized perioperative care facilitates a data-driven approach to inform implementation teams where best to focus their efforts and to address barriers to the uptake of and compliance with implementation, in hopes of establishing the sustainability of ERAS protocols and data collection processes. There are several ERAS guidelines and implementation tools available online that are easily adapted to local practices, and their impact can be efficiently monitored through the ACS NSQIP.33,34
Footnotes
Presented at the 2016 Canadian Surgery Forum, Sept. 8–10, 2016, Toronto, Ont.
Competing interests: None declared.
Contributors: J. Trickett, E. Pearsall, M. McKenzie, R. McLeod and R. Auer designed the study. M. Sadiq, M. McGrath, K. Lacelle, M. Szeto, J. Trickett, D. Schramm, E. Pearsall, R. McLeod and R. Auer acquired the data, which L. Gresham, M. Sadiq, G. Gresham, E. Pearsall and R. Auer analyzed. M. Sadiq and R. Auer wrote the article, which all authors reviewed and approved for publication.
- Accepted September 17, 2018.
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.