


Abstract
Background: Long-term complications and lack of weight loss have caused a surge in laparoscopic adjustable gastric band (LAGB) removal. This study reviews the trend of LAGB removal and examines outcomes of patients undergoing subsequent revision bariatric surgery at a single tertiary care centre in Canada.
Methods: All LAGB removals performed between January 2008 and December 2016 were reviewed. A subset of patients who underwent revision surgery was then analyzed for patient demographics, weight, body mass index and postoperative complications.
Results: During the study period, 211 patients underwent LAGB removal (87.7% female). Most bands were inserted out of province. Reasons for band removal included dysphagia, band slip and weight recidivism. Fifty-nine patients (28%) underwent revision surgery at a mean of 12.8 ± 9.3 (range 0–55) months after LAGB removal. Mean age was 47 ± 9.7 (range 26–63) years, and mean pre-LAGB weight was 131.0 ± 30.0 kg. Following LAGB, the mean weight decreased to 120.5 ± 26.4 kg, but most regained weight after removal to a mean prerevision weight of 125.1 ± 27.0 kg. The lowest mean weight was achieved 12 months after revision surgery (98.7 ± 30.2 kg). The mean percent total weight loss was not significantly different after revision laparoscopic Roux-en-Y gastric bypass compared with revision laparoscopic sleeve gastrectomy (22.8 ± 9.6% v. 17.5 ± 6.5%, p = 0.179). The overall revision surgery 30-day complication rate was 18.6% and increased to 23.7% long-term. No deaths occurred.
Conclusion: The number of LAGB removals is increasing. Revision bariatric surgery leads to improved weight loss; however, revision surgery is associated with complications.
Obesity increases all-cause mortality.1,2 Managing this challenging and burgeoning disease is demanding. Surgery is the only successful long-term treatment.3 With great enthusiasm, the laparoscopic adjustable gastric band (LAGB), which was first introduced in 1993 and approved by the US Food and Drug Administration in 2001, was rapidly adopted.4,5 Its use peaked in 2008, with 44% of bariatric surgeries being LAGB procedures.6
The operation has a short learning curve, short operative time and length of stay, with many places doing these as day surgeries; it is reversible, does not alter anatomy, and allows the patient to adjust restriction based on band fill volume.3,4 Early results were promising, with low complication rates, good weight loss results and significant comorbidity resolution.8 As with certain novel surgical interventions, the LAGB fell foul of the sign wave of new technology.6 With time, the band’s high long-term complications, including weight recidivism, obstructive symptoms, dysphagia, slippage, esophageal dilation, esophagitis, gastric erosion, and port-site infections have made the band the least favourable weight loss procedure currently. 5,7 Hence, it is not surprising that in 2014 less than 1% of all bariatric surgeries performed in the United States were LAGB procedures.7
It is likely that several hundreds of thousands of LAGBs have been inserted worldwide since its introduction 25 years ago.6 The literature suggests that 50%–80% of these will need to be removed eventually, leading to subsequent revision bariatric surgery in many patients.5,8 Removal of LAGB is associated with higher complication rates than band placement.9 Furthermore, revisional surgery, whether cardiac, orthopedic, or bariatric is associated with higher complications than primary surgeries.10,11
To handle the considerable volume of patients (provincially, nationally, and medical tourists) having undergone previous bariatric procedures, our institution opened a bariatric surgery revision clinic in 2009.12 This study examines our 9-year experience of patients who sought band removal for a variety of reasons and the outcomes of their revision bariatric surgery when applicable.
Methods
A retrospective review of all patients who underwent LAGB removal at a single institution between January 2008 and December 2016 was carried out. Patients who underwent LAGB removal were identified using the hospital’s operating room Virtual Address Extension (VAX) system. Data were also collected from both hospital and clinic records. Charts were reviewed by the primary author (V.F.) for patient demographics, place of band insertion, the length of time the band was in situ, reason for band removal, and whether or not revision surgery was done. The subset of patients who underwent revision surgery was then further analyzed for patient demographics; time interval to revision; and weight at time of band placement, removal, revision and up to 1 year after revision bariatric surgery. Weight loss was calculated based on the American Society for Metabolic and Bariatric Surgery (ASMBS) reporting guidelines (see the weight loss calculations section).13 Both short-term (< 30 days postoperative) and long-term (> 30 days postoperative) complications following revision surgery were noted. The institutional health ethics board approved this study.
All LAGB removals and revision surgeries were carried out by 1 of 5 bariatric surgeons. Prior to revision, a multidisciplinary team of nurses, dietitians, psychiatrists, bariatric physicians and surgeons assessed all patients. If the original LAGB surgery was done at our centre, the patients had previously been assessed and were deemed adequate candidates for bariatric surgery and therefore followed up with the bariatric surgery clinic. However, patients who had their LAGB procedure done elsewhere without adequate preoperative assessment were referred to the Edmonton Revision Bariatric Surgery clinic. While all patients underwent standard preoperative work-up (blood work, chest radiograph, cardiogram), investigations such as barium swallow, manometry and upper endoscopy were individualized to patients’ presentation. Options for revision surgery included redo gastric banding, sleeve gastrectomy and gastric bypass. If possible, these were done laparoscopically. Details of revision surgery techniques at our institution have been published previously.14
Weight loss calculations
Percent total weight loss (%TWL) was calculated as follows: %TWL = [(revision surgery weight) – (postoperative weight)] ÷ (revision surgery weight) × 100. Percent excess body mass index (BMI) loss (%EBMIL) was calculated as follows: %EBMIL = [ΔBMI ÷ (revision surgery BMI – 25)] × 100, where ΔBMI = revision surgery BMI – postoperative BMI.
Statistical analysis
All statistical analysis was done using SPSS for Windows, version 21 (IBM). Continuous variables are reported as means with standard deviations. Data analysis was carried out using χ2 tests for categorical variables and t tests for continuous variables.
Results
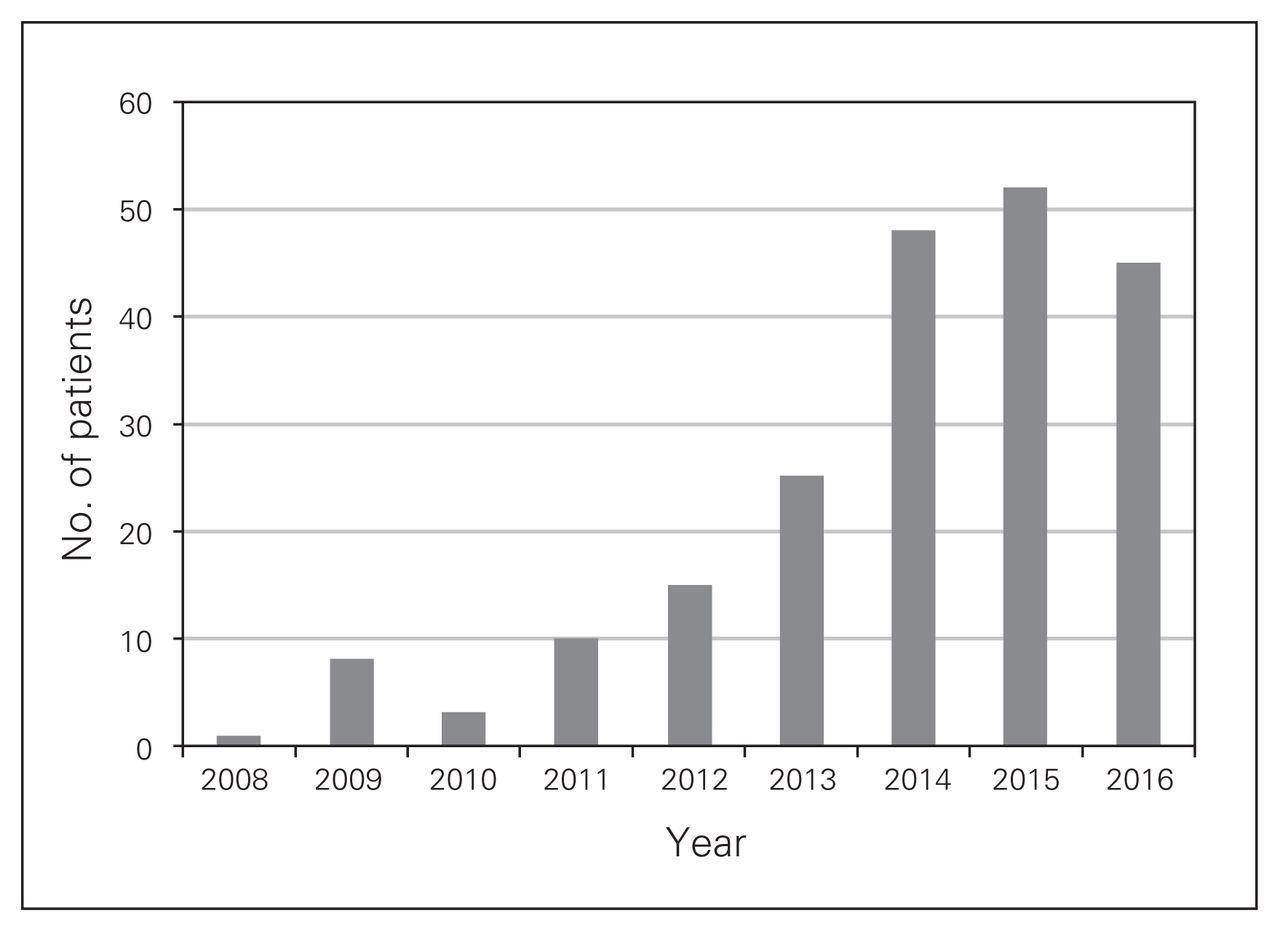
Between January 2008 and December 2016, 211 laparoscopic gastric bands were removed. Of these patients, 185 patients were female (87.7%). The annual number of band removals increased significantly from 2008 to 2016, with the peak in 2015 (Fig. 1). The mean time from band insertion to removal was 4.5 ± 2.6 years (range 2 months to 12 years). Most LAGBs were placed out of province: 82 (38.9%) in Ontario, 65 (30.8%) in Alberta, 29 (13.7%) in Mexico, 8 (3.8%) in a Canadian province other than Ontario or Alberta, 4 (1.9%) in Europe, 1 (0.5%) in the United States and 1 (0.5%) in Africa. For the remaining 21 LAGB removal patients (10.0%), no information regarding location of LAGB insertion was available. It can be assumed that none of these were placed at our institution, as there would have been records to indicate it.
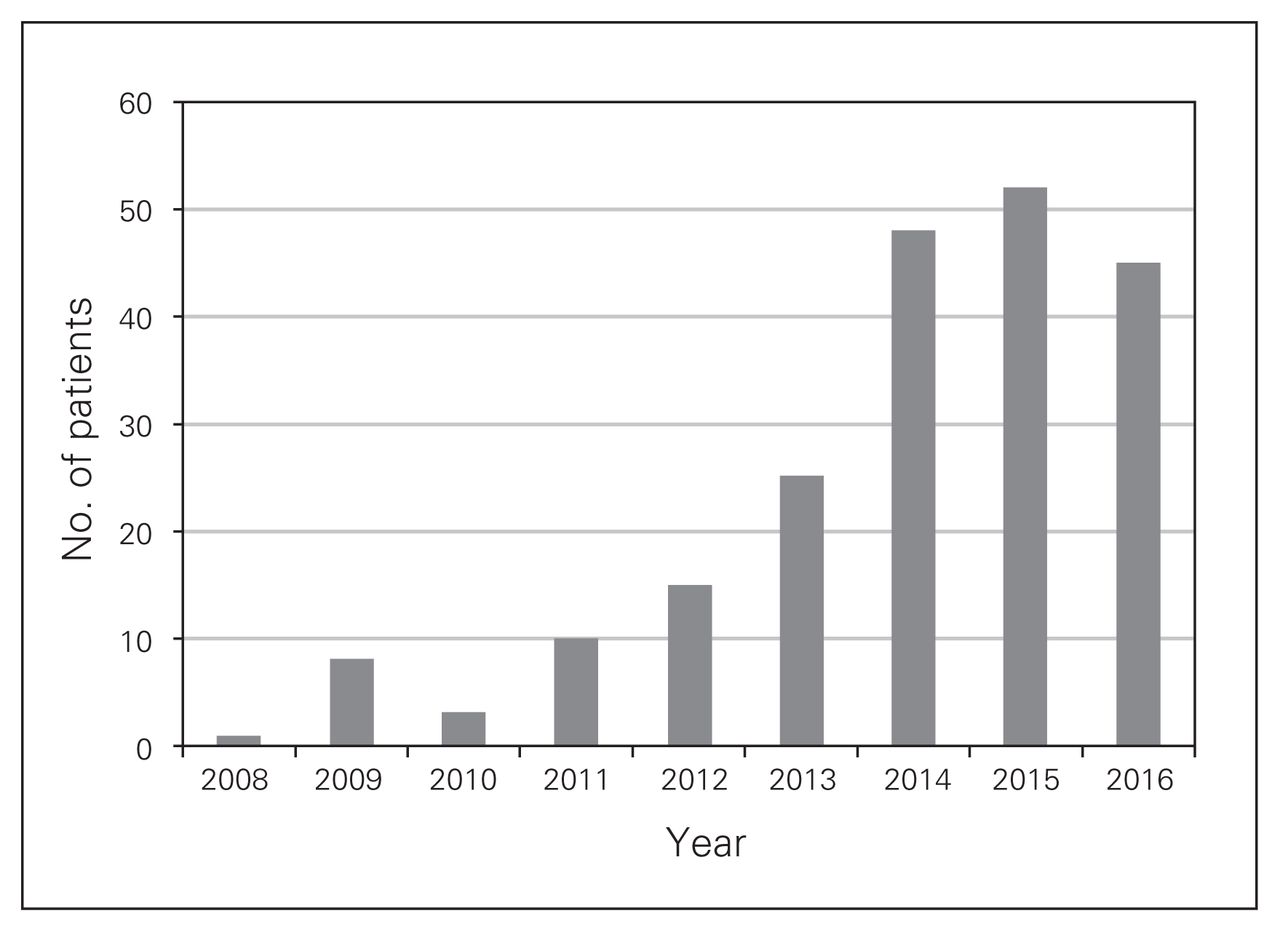
Annual laparoscopic adjustable gastric band removal rates.
The 3 most common reasons for band removal were dysphagia, band slip and weight recidivism (Table 1).
Reasons for LAGB removal
Of these 211 LAGB removal patients, 59 (28%) went on to have revision bariatric surgery. Most patients were female (84.7%). The mean age at revision was 46.6 ± 9.7 (range 26–63) years. The mean time from band removal to revision surgery was 12.8 ± 9.3 (range 0–55) months; 3 patients had 1-stage revision procedures (1 redo LAGB, 1 laparoscopic sleeve gastrectomy [LSG], 1 laparoscopic Roux-en-Y gastric bypass [LRYGB]). Revision surgeries included 30 LSG, 26 LRYGB, 2 open RYGB and 1 LAGB.
The weight and BMI trends for revision surgery patients are shown in Table 2. Although LAGB achieved substantial weight loss initially, most patients regained weight following band removal. Revision surgery achieved the greatest weight loss. At 12 months after revision surgery, neither the mean %TWL (22.8 ± 9.6% v. 17.5 ± 6.5%, p = 0.179) nor the %EBMIL (44.8 ± 13.5 v. 56.4 ± 29.6, p = 0.287) was significantly different for revision LRYGB compared with revision LSG. Only 1 patient regained weight after revision surgery (redo LAGB).
Weight trends for revision surgery patients
The overall 30-day complication rate of revision bariatric surgery was 18.6%; 4 (13.3%) after LSG, 6 (23.1%) after LRYGB, and 1 after open RYGB. None of the patients who underwent a 1-stage procedure in this study had postoperative complications. While the rate of 30-day complications was higher in the revision LRYGB group than the revision LSG group (23.1% v. 13.3%), this was not statistically significant (p = 0.516). Two leaks occurred, both after revision LSG (3%). Three late complications occurred, all in revision LRYGB patients: gastrogastric fistula treated by laparoscopic revision, gastrojejunal anastomotic stricture treated with dilation, and perforated ulcer at gastrojejunal anastomosis treated with laparoscopic omental patch. Including both short- and long-term complications, a total of 14 (23.7%) patients experienced postoperative complications after revision surgery (Table 3). No deaths occurred.
Complications after revision LSG and LRYGB with respective treatment
Discussion
Although gastric banding was a promising treatment for obesity, its high long-term complications and significant failure rate have caused a significant decrease in LAGB insertions.7 This trend is also seen at our institution, where LAGB has been essentially abandoned. With this decline in band insertion comes a steep increase in LAGB removals. At our institution, the rate of band removals increased from 1 per year to more than 50 per year within a 7-year period (Fig. 1). The literature supports this trend.15,16 Vinzens and colleagues reviewed more than 400 LAGB patients in Switzerland; follow-up exceeded 13 years.4 More than 70% of patients had their band removed, and 63% underwent revision bariatric surgery.4
Tammaro and colleagues present their centre’s 10-year experience with LAGB.17 They divided reasons for band removal into unsuccessful results (7.8%) versus long-term complications: pouch/esophageal dilation (11.5%), band slippage (10.7%), reflux (3.1%), band erosion (3%), and band infection (1%). These results are contrary to those of most other studies, which show that insufficient weight loss/weight recidivism was the main reason for band removal.4,10 Our results are similar to those of Tammaro and colleagues, with the most common reason for band removal being dysphagia. Some patients may have had both weight regain/insufficient weight loss and obstructive symptoms, including dysphagia, nausea and vomiting. The interesting combination of obstructive symptoms and weight regain suggests that symptoms are intermittent and are not severe enough to cause weight loss, which would be seen in nonbariatric patients who present with similar symptoms due to primary pathology such as Schatzki rings, reflux esophagitis, esophageal dysmotility or malignancy. We suggest that any patients with persistent symptoms following removal of LAGB should be investigated further with upper endoscopy, fluoroscopy and manometry, especially if revision surgery is being considered.
Among revision patients, LAGB achieved a change in mean weight of 10.5 kg and mean BMI loss of 3.2 kg/m2. This BMI loss was not as high as predicted by studies such as that of Hutter and colleagues,18 who reported a BMI loss of ≥ 7 kg/m2 12 months after LAGB. This suggests that while most of our patients reported obstructive symptoms, they also had insufficient weight loss. The variation in reasons for band removal seen among published studies may be due to interpretation bias, varying practice attitudes regarding gastric bands, and to most studies being retrospective reviews. Removal of LAGB led to significant weight regain in our revision patient cohort. This is in agreement with the results of Lanthaler and colleagues,19 who showed that most patients regain weight following gastric band removal and that almost 3 out of 4 would not proceed with LAGB again.
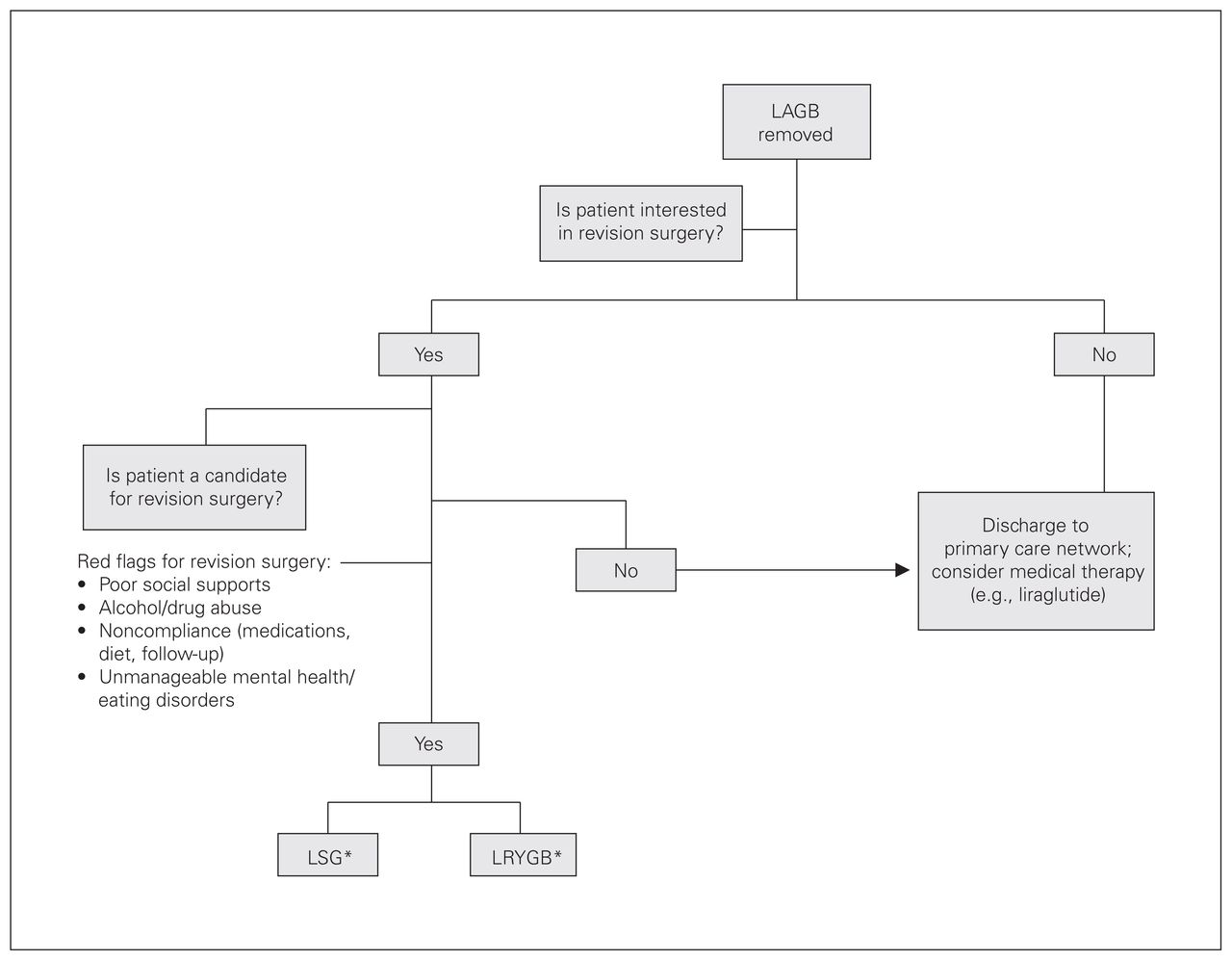
The data presented reflect our common practice to stage revision procedures with mean time to revision surgery of around 1 year. The literature suggests that 1-stage revision is safe.5 But safety is only 1 outcome parameter; appropriateness and chance of long-term success with a definitive revision bariatric procedure must also be factored in. Following band removal, patients may fit in 1 of 3 groups: (i) not interested in revision; (ii) interested in revision, but not a revision candidate owing to red flags;20 and (iii) interested in revision and good revision candidate (Fig. 2). Owing to the retrospective nature of this study, it cannot be said how many of the 211 patients who underwent LAGB removal belonged in each group, but we do know that close to one-third qualified for and underwent revision surgery. We encourage the approach to LAGB removal patients outlined in Figure 2 to guide practitioners in revision decision-making.
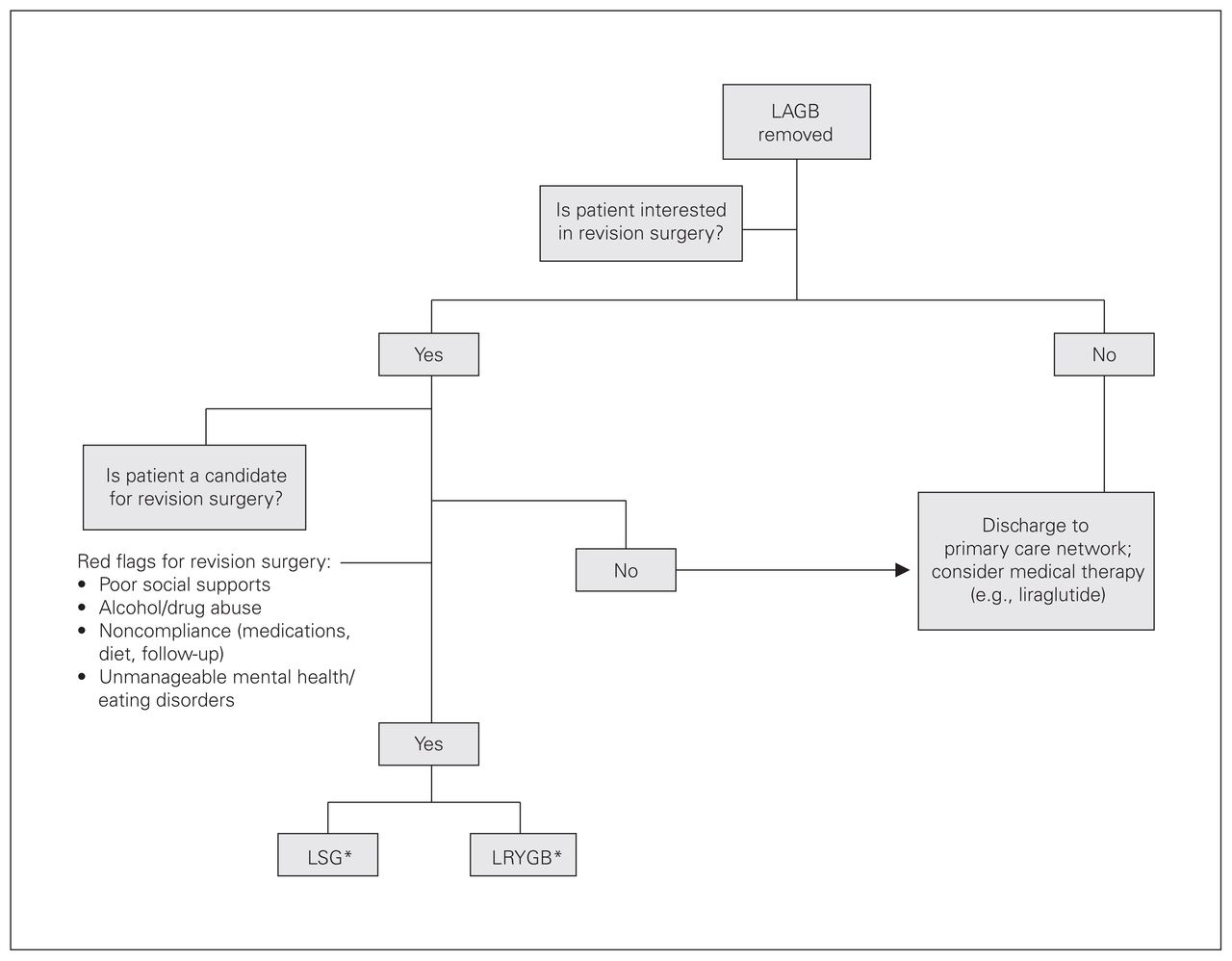
The Edmonton approach to patients after laparoscopic adjustable gastric band (LAGB) removal. *The decsion to proceed with either laparoscopic sleeve gastrectomy (LSG) or laparoscopic Roux-en-Y gastric bypass (LRYGB) is based on patient preference and comorbidities. In our institution, gastroesophageal reflux disease (GERD) is conisdered a contraindication to LSG. Patients with diabetes mellitus (DM) are advised that LRYGB has better resolution rates for DM than LSG.
Our overall 30-day revision surgery complication rate of 18.6% is within the range observed in the literature (4.4%–22.6%).10 The leak rate for revision LSG ranged from 1.2% to 3.5% in previous studies;10 our leak rate of 3% is within this range.
Our findings confirm that revision surgery has higher complication rates than primary bariatric surgery.18 While one can postulate that prior manipulation of tissues affects blood supply and leads to scar tissue surrounding the operative field, the literature is divided. In a recent systematic review and meta-analysis, Sharples and colleagues10 address the outcomes after revision LRYGB and LSG. They included 36 studies with a total of 2617 patients. The overall pooled morbidity was 13.2% (8.9% early and 8.1% late complications). Although not statistically significant, the overall complication rate was lower for LSG than LRYGB (16.5% v. 7.7%), but the leak rate was slightly higher for LSG (2.2% v. 1.8%). No study directly compared 1-stage versus 2-stage complication rates. We agree with Sharples and colleagues that revision bariatric surgery is safe; however, complication rates are higher than for primary bariatric surgery.
Limitations
This study is limited by its retrospective nature and, as some patients had their original LAGB placed outside the province, not all data were available. The study’s sample size is relatively small, which may introduce type II error when comparing the groups of revision LRYGB and LSG. No conclusion can be made regarding a 1-step versus 2-step revision approach, as only 3 patients underwent 1-step procedures. Furthermore, data were not available for patients who chose not to have or did not qualify for revision surgery.
Conclusion
The demand for LAGB removal and revision bariatric surgery has significantly increased. As complication rates of revision bariatric surgery are higher than for primary LSG or LRYGB, patients seeking revision surgery warrant a thorough and coordinated assessment strategy by a specialized bariatric team.
Footnotes
These data were presented at the Canadian Obesity Summit, April 26–28, 2017, Banff, Alta.
Competing interests: None declared.
Contributors: V. Falk, D. Birch and C. de Gara designed the study. V. Falk and C. Sheppard acquired the data, which V. Falk, A. Kanji and S. Karmali analyzed. V. Falk, C. Sheppard and C. de Gara wrote the article, which all authors reviewed and approved for publication.
- Accepted December 17, 2018.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.