


Abstract
Background: Idiopathic intracranial hypertension (IIH) is a rare condition typically affecting women with obesity who are of child-bearing age. Patients commonly present with headaches, visual disturbances, pulsatile tinnitus and papilledema. The association between IIH and obesity has been well established in the literature, suggesting that weight loss may contribute to improving IIH. For patients with severe obesity for whom conservative management is not successful, bariatric surgery is an effective modality for weight loss. We aimed to systematically review the literature to determine the efficacy of bariatric surgery in the treatment of IIH
Methods: We conducted a comprehensive search of MEDLINE, Embase, Scopus, the Cochrane Library and Web of Science (limited to studies in humans published in English between January 1946 and July 2015).
Results: Twelve primary studies (n = 39 patients) were included in the systematic review. All patients had a preoperative diagnosis of IIH. Preoperative body mass index (BMI) was 47.4 ± 3.6 kg/m2; BMI improved to 33.7 ± 2.1 kg/m2 and 33.9 ± 11.6 kg/m2 at 6 and 12 months postoperatively, respectively. Lumbar puncture opening pressures decreased from 34.4 ± 6.9 cm H2O to 14.0 ± 3.6 cm H2O after surgery. Common symptoms of IIH improved after bariatric surgery: headaches (100% preoperatively v. 10% postoperatively), visual complaints (62% v. 44%), tinnitus (56% v. 3%) and papilledema (62% v. 8%).
Conclusion: Bariatric surgery appears to lead to considerable improvement in IIH. Idiopathic intracranial hypertension is not a well-publicized comorbidity of obesity, but its presence may be considered as an indication for bariatric surgery.
Idiopathic intracranial hypertension (IIH), also commonly referred to as pseudotumour cerebri, is a rare condition typically affecting women with obesity who are of child-bearing age.1 Patients with IIH commonly present with headaches, visual disturbances, pulsatile tinnitus, nausea, vomiting, photophobia and neck, shoulder or radicular pain.1,2 Patients with IIH can also present with visual field defects, visual acuity deficits, blind spot enlargement and papilledema on fundoscopy.1 Idiopathic intracranial hypertention is classically diagnosed using the modified Dandy criteria;3 however, it is commonly diagnosed in patients presenting with signs and symptoms associated with increased intracranial pressure, a lumbar puncture opening pressure greater than 25 cm H2O and evidence of normal cerebral anatomy on imaging.4 Patients with IIH require urgent diagnosis and management to prevent further complications, as IIH can ultimately result in permanent loss of vision.1
The association between IIH and obesity has been well established in the literature.5–10 A common theory suggests that obesity causes increased intra-abdominal pressure resulting in increased pleural pressure and cardiac filling pressure. The increased pressures lead to increased venous pressure, decreased venous blood flow from the brain and, ultimately, increased intracranial pressure.8 Although both conservative management with diuretics11,12 and invasive interventions, such as therapeutic lumbar puncture,13 optic nerve sheath fenestration14 and shunt surgery,15–17 are available, these options are not definitive treatments and provide only symptomatic relief for patients.1,2,9,10 Because the link between IIH and obesity has been well established, weight loss has the potential to improve IIH symptoms. Where diet and exercise fail to result in significant weight loss, other methods need to be explored for the treatment of obesity and consequently IIH.
As bariatric surgery remains the only treatment modality that has been proven to be successful for patients with severe obesity for whom conservative management has been unsuccessful, various case reports and case series have identified bariatric surgery as a potential option for patients with IIH.8,18–31 We aimed to systematically review the literature to determine the efficacy of bariatric surgery for the treatment of IIH.
Methods
A comprehensive search of MEDLINE, Embase, Scopus, the Cochrane Library and Web of Science from 1946 to July 2015 was completed. Title searching was restricted to the following keywords and terms: bariatric surgery/gastric bypass/gastric band/sleeve gastrectomy and intracranial hypertension/pseudotumour cerebri. Only studies in humans that were published in English were included.
All cohort studies, case series and case reports were included in this study. Abstracts were selected on the basis of the following inclusion criteria: patients diagnosed with IIH, patients who have undergone bariatric surgery, and studies directly comparing pre- and postoperative outcomes. The full-text articles for all selected abstracts were reviewed thoroughly using the same inclusion criteria by 2 independent reviewers (W.Y.L.S., N.J.S.). Pertinent data were extracted independently by 2 reviewers (W.Y.L.S., N.J.S.) from full-text articles, including the basic demographic characteristics of the patients, the number of patients with symptoms, lumbar puncture opening pressures and pre- and postoperative body mass index (BMI).
Results
Preliminary database searches of the literature yielded 120 articles with 115 potentially relevant articles after duplicates were removed. After titles and abstracts were screened, 33 eligible studies were retained. One additional record was identified through reference searching. Full-text articles were reviewed, and 12 primary studies comprising 39 participants were included in this systematic review (Fig. 1).
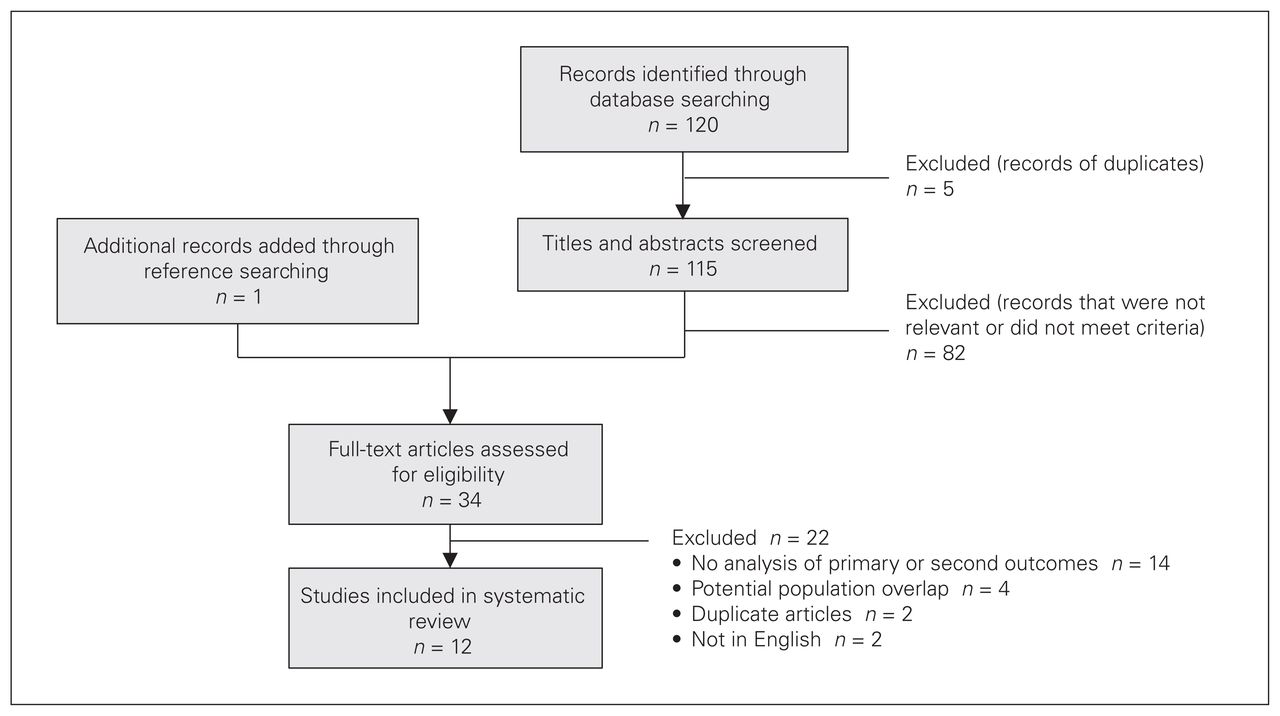
Flow chart of study selection.
Twelve primary studies18–23,25–28,30,31 were included in the systematic review, accounting for a total of 39 participants, all of whom were diagnosed with IIH preoperatively. Of the 39 participants, 38 were female, and the average age of all participants was 32.5 years. The demographic characteristics of the patients in the primary studies are summarized in Table 1. The quality of the primary studies was not evaluated as the available evidence was scarce and case reports had to be included.
Demographic characteristics of the 39 study participants
Signs and symptoms associated with IIH were recorded for all 39 patients preoperatively (Table 2 and Table 3). All 39 patients (100%) had headaches; 24 (62%) had visual symptoms, which included blurring, visual disturbances or ocular pain; and 22 (56%) had pulsatile tinnitus. Preoperative fundoscopy revealed that 24 patients (62%) had papilledema and 22 (56%) had visual field deficits. The mean preoperative lumbar puncture opening pressure was 34.4 ± 6.9 cm H2O.
Summary of major preoperative findings
Summary of major postoperative findings
All patients underwent bariatric surgery. Twenty-nine (74%) underwent Roux-en-Y gastric bypass, 6 (15%) underwent adjustable gastric banding, 3 (8%) underwent sleeve gastrectomy and 1 (3%) had gastric exclusion surgery. Average preoperative BMI was 47.4 ± 3.6 kg/m2. Average BMI at 6 and 12 months postoperatively was 33.7 ± 2.1 kg/m2 and 33.9 ± 11.6 kg/m2, respectively (Table 3).
Postoperatively, 35 patients (90%) reported significant improvement in or resolution of their headaches at follow-up, which varied from 3 months to 3 years (Table 2). Seven patients (29%) reported improvement in or resolution of visual symptoms. All but 1 patient reported resolution of pulsatile tinnitus (96%). Postoperative fundoscopy revealed that 21 patients (88%) had resolved or stabilized papilledema and 4 patients (18%) had resolved or stabilized visual field deficits. Postoperative lumbar punctures were recorded in only 4 patients, with the average opening pressure improving to 14.0 ± 3.6 cm H2O (Table 3).
Discussion
Our systematic review found that bariatric surgery is associated with complete remission or substantial improvement of signs and symptoms associated with IIH. Headaches, which are the most commonly reported symptom of IIH and were seen in all of the patients preoperatively, completely resolved or significantly improved in most of the patients (89.7%). Similarly, 95.5% of patients with pulsatile tinnitus reported complete resolution of this symptom following bariatric surgery, and 87.5% of patients with papilledema found on perioperative fundoscopy experienced resolution, improvement or stabilization following surgery. The results from this study suggest a promising treatment option for IIH. The efficacy of established treatment modalities for IIH such as acetazolamide, optic nerve sheath fenestration and shunt surgery have been studied,32,33 but to our knowledge no direct comparison between bariatric surgery and other treatment modalities has been published in the literature.
The cause of IIH is unknown, but several hypotheses exist.8,13,34–36 A theory linking obesity and IIH suggests that obesity raises intra-abdominal pressure, leading to increased pleural pressure and cardiac filling pressures, which in turn impedes venous return in the brain and ultimately results in increased intracranial pressure.8 Although the definitive cause of IIH has not been identified, obesity (through its effect on intra-abdominal pressure) is thought to be a significant contributing factor.
Several studies have demonstrated that weight loss is an effective treatment for IIH.37–39 Although the ideal treatment for obesity is lifestyle management, the effectiveness of diet and exercise for weight loss in patients with obesity is poor for several reasons, including the complex pathophysiology of obesity management.40–43 The emergence of bariatric surgery for the morbidly obese population has provided these patients with an effective way to lose a substantial amount of weight.44–46
The 2 most commonly performed bariatric procedures are laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy. Owing to the paucity of primary data on bariatric surgery as a treatment for IIH, we elected to include all types of bariatric procedures in this study, including gastric banding. Several studies have alluded to the superiority of laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy over gastric banding because of the greater weight loss and lower rates of complications and revisions with the former procedures.44,47,48 Although our study suggests that bariatric surgery may be an effective treatment for IIH, we recommend laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy as the primary procedures of choice.
There is a lack of prospective studies on IIH that describe its natural history. Although most patients have a protracted course in which symptoms gradually worsen without treatment,49 there have also been cases of severe and rapidly progressive IIH.50 Although bariatric surgery is a sound treatment option for obesity and potentially IIH, its effectiveness for IIH is observed when the patient loses weight and subsequently decreases their intra-abdominal pressure. For patients with more acute presentations of IIH and vision loss, emergent symptomatic relief must be provided in terms of neurosurgical15–17 and ophthalmic techniques14 as suggested by Fridley and colleagues.9 Nonetheless, the improvement in symptoms following bariatric surgery suggests the potential for bariatric surgery to be useful in the treatment of IIH.
With the increasing incidence of obesity worldwide and advances in surgical techniques, the demand for bariatric surgery is increasing.51 Many patients who are eligible for bariatric surgery are unable to receive it because of access and financial barriers.52 As a result, public health systems have to triage patients on the basis of the severity of their obesity and their obesity-related comorbidities. Although there is a strong association between IIH and obesity, IIH is not widely recognized as an indication for bariatric surgery. By improving access to bariatric surgery in patients who are obese and who have IIH, there is potential to target a group that has substantial potential for improvement. Therefore, further research, such as randomized controlled trials and cost–benefit analyses, should be performed not only to establish IIH as an indication for bariatric surgery, but also to compare the efficacy of bariatric surgery with that of the current standard of care for IIH.
Although other reviews on this topic have been published,9,10 to our knowledge this systematic review is the most recent and comprehensive. The conclusions and findings were, not surprisingly, similar across studies. We did not report on 3 additional studies that met our inclusion criteria but were included in the other reviews.8,24,29 Some of the patients in these 3 studies received bariatric surgery from the same surgeon, at the same centre, and over the same time frame as the population from 1 of the studies we included in our review.30 To avoid double counting, we included only the most comprehensive of the 4 studies.30
Limitations
One limitation of this analysis is the lack of high-quality primary studies on the topic of bariatric surgery as a treatment for IIH. Although 12 primary studies were included, the majority18,19,21–23,25–28,31 were case reports and case series. Given that case studies are particularly prone to reporting bias, the effects of bariatric surgery in the treatment of IIH may have been overestimated in our results.
Conclusion
Although the quality of the studies included in this systematic review was limited, bariatric surgery appears to lead to considerable improvement in the symptoms of IIH, including headaches, visual symptoms and papilledema. Although IIH is not a well-recognized comorbidity of obesity, its presence may be considered as patients are being triaged for bariatric surgery. The presence of IIH in a patient with obesity may be an indication for more urgent intervention. Further research, such as randomized controlled trials and cost–benefit analyses, should be undertaken to determine the efficacy, safety and feasibility of bariatric surgery in severely obese patients with IIH.
Footnotes
Competing interests: D. Birch is a consultant for Ethicon and Covidien. He has received educational grants from Ethicon, Covidien and Stryker and teaching honoraria from Cook Surgery and Bard Davol. S. Karmali is a consultant for Gore Medical and Ethicon. No other competing interests were declared.
Contributors: W. Sun, N. Switzer, R. Gill, C. de Gara, D. Birch, A. Nataraj and S. Karmali designed the study. W. Sun and X. Shi acquired the data, which W. Sun, J. Dang, X. Shi and A. Nataraj analyzed. W. Sun, J. Dang, R. Gill and S. Karmali wrote the article, which N. Switzer, J. Dang, R. Gill, X. Shi, C. de Gara and D. Birch critically reviewed. All authors provided final approval for publication.
- Accepted July 24, 2019.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.