


Abstract
Background: In medical and surgical departments around the world, morbidity and mortality conferences (MMC) serve dual roles: they are cornerstones of quality-improvement programs and provide timely opportunities for education within the urgent context of clinical care. Despite the widespread adoption of MMCs, adverse events and preventable errors remain high or incompletely characterized, and opportunities to learn from and adjust to these events are frequently lost. This review examines the published literature on strategies to improve surgical MMCs.
Methods: We searched OVID Medline, PubMed, Embase and CENTRAL. We defined our combination of search terms using a PICO (population, intervention, comparison, outcome) model, focusing on the use of MMCs in general surgery.
Results: The MMC literature focused on 5 themes: educational value, error analysis, case selection and representation, attendance and dissemination. Strategies used to increase educational value included limiting case presentation time to 15–20 minutes, mandatory brief literature reviews, increasing audience interaction, and standardizing presentations using a PowerPoint template or SBAR (situation, background, assessment, recommendation) format. Interventions to improve error analysis included focused discussion on causative factors and taxonomic error analysis. Case selection was improved by using an electronic clinical registry, such as the National Surgery Quality Improvement Program, to better capture incidence of morbidity and mortality. Attendance was improved with teleconferencing. Dissemination strategies included MMC newsletters, incorporating MMCs into plan-do-check-act cycles, and surgeon report cards.
Conclusion: Greater standardization of best practices may increase the quality improvement and educational impact of MMCs and provide a baseline to measure the effect of new MMC format innovations on the clinical and educational performance of surgical systems.
Since the early 1900s, morbidity and mortality conferences (MMCs) have been a refuge for thoughtful reflection and deliberation and a cornerstone of quality improvement efforts.1–3 Often referred to as the “golden hour” of residency training, MMCs have also played a crucial role in surgical education. With the increasing prominence of safety in medical and surgical culture, it is useful to see quality and education as being inextricably linked; this recognition gives the reassessment, and perhaps reimagination of MMCs, with their longstanding emphasis on both quality and education, unprecedented relevance and urgency.4
In general surgery and its subspecialties, adverse events occur in 14% and 30% of scheduled and emergency operations, respectively, thus establishing that high-functioning MMCs may be of particular importance.5–7 Currently, the format and conduct of surgical MMCs are heterogeneous, and a lack of evidence and consensus limits their generalizability and, perhaps, their effectiveness.8–10 In a recent systematic review, Xiong and colleagues8 aimed to describe the current content and process of MMC programs in both medicine and surgery across multiple institutions. Their report summarized the most common features of surgical MMCs: 60% occur weekly, 28% last 1 hour, 60% have residents as presenters, 56% have a faculty member moderator, and most are attended by multidisciplinary health care professionals. Surprisingly, inclusion of a scientific review to contextualize adverse events or support MMC-driven quality improvement was reported as a requirement in only 40% of included studies. Although many studies failed to describe vital components of their MMC process, considerable variability in the structure and content of surgical MMCs was evident.
Several studies suggest that MMCs are not meeting their goals in quality improvement and education.1,2,8,11–14 The vast majority of MMCs lack the fundamental principles necessary to identify the root cause of adverse events and implement systematic preventative change.8,9,15,16 Bal and colleagues16 identified shortcomings in explaining causation of adverse events in 91% of MMC cases, with less than 10% employing a structured method of error analysis. Furthermore, morbidity is notoriously underreported in the current format of MMCs. More concerning, MMCs have also been found to underreport mortality.17,18 Case selection is often nonstandardized, chosen based on interest rather than merit or educational value, and is subject to recall bias.17,19–21 Finally, presentation style may detract from educational value, as the usual didactic approach of an MMC results in passive learning, despite trends in medical education moving toward more active forms of learning.22
We conducted a narrative systematic literature review to identify studies investigating surgical MMC format changes. Currently, several papers present theoretical models for systematic improvement of MMCs, but few actually investigated interventions.14,15,23 The Ottawa MMC model represents one vetted protocol for systematic change and standardization in MMCs, but it is not specific for surgery.24–26 Giesbrecht and Au27 and Benassi and colleagues28 previously conducted systematic reviews investigating strategies used in medicine and surgery to improve the quality of MMCs. Our goal was to build upon their work by identifying MMC interventions aimed at improving both the quality improvement and educational components of MMCs, particularly for general surgery, where a high degree of acuity and complexity can be associated with a high incidence of preventable adverse events.7
Methods
We searched OVID Medline, PubMed, Embase and CENTRAL, and we supplemented our search by reference harvesting from the bibliographies of included studies. We defined our combination of search terms using a PICO (population, intervention, comparison, outcome) model. Population was limited to general surgery and subspecialties with emphasis on emergency general surgery; intervention included all format changes to an existing MMC model; comparison was the prior MMC format of each study; and outcomes included any demonstrated improvement in MMC, such as perceived increase in presentation quality, practice change, or enhanced educational value. We used the following search terms and medical subject headings (MeSH): “morbidity and mortality conference” or “morbidity and mortality rounds” or “morbidity and mortality meeting” and “acute*” or “ACS” or “trauma” or “emergency” or “general surgery” or “surg*.” Expanded search terms pertaining to emergency general surgery were included because of the relatively high incidence of adverse events. No limit in the range of publication date was applied.
After applying our search terms to the 4 identified search engines, we removed all duplicates, and 2 independent reviewers (N.S. and P.S.) screened the remaining papers based on title and abstract. Microsoft Excel and manual editing were used to manage papers and remove duplicates. Papers were removed as “clear misses” if they did not apply an intervention to their MMC, did not pertain to general surgery, were not available in English, or were review articles. Next, 2 reviewers (N.S. and P.S.) performed an in-depth investigation of the full text of all remaining papers using predetermined inclusion and exclusion criteria (Box 1). Disagreements were resolved by discussion. Finally, the research design of each study and their limitations were appraised. Narrative data were then extracted from each paper in a standardized method, including details regarding study design, setting, summary, MMC intervention and outcomes. The reviewers collectively analyzed the extracted data for recurrent themes, common interventions and similar outcomes.
Inclusion and exclusion criteria applied in a systematic review of interventions to improve surgical morbidity and mortality conferences
Inclusion criteria
Stated inclusion of a general surgery service including all subspecialties
Analysis of morbidity and mortality rounds that tested an intervention and included outcomes indicative of quality, such as
Enhanced case selection
Increased participant engagement or satisfaction
Increased effectiveness of dissemination
Reduction in morbidity and/or mortality
Increased identification of systematic and preventable errors
Education of attendees
Exclusion criteria
Inclusion of specific surgical services other than general surgery
Inclusion of exclusively or primarily non-surgical specialties or hospital-wide studies
Descriptive analysis with no intervention to morbidity and mortality protocols
Language other than English
Rounds not limited to morbidity and mortality
Review and opinion articles
Quality improvement of morbidity and mortality rounds was not a primary objective
No description of strategy used to improve morbidity and mortality rounds was provided
Results
Our search captured 279 papers, which included 117 duplicates. Of the remaining 162 papers, 130 were removed as “clear misses,” leaving 32 papers chosen for full review. Only 18 of those papers met the predetermined inclusion and exclusion criteria. An additional 3 papers were identified and included through reference harvesting, resulting in 21 papers included for narrative analysis. These results are summarized in Figure 1.
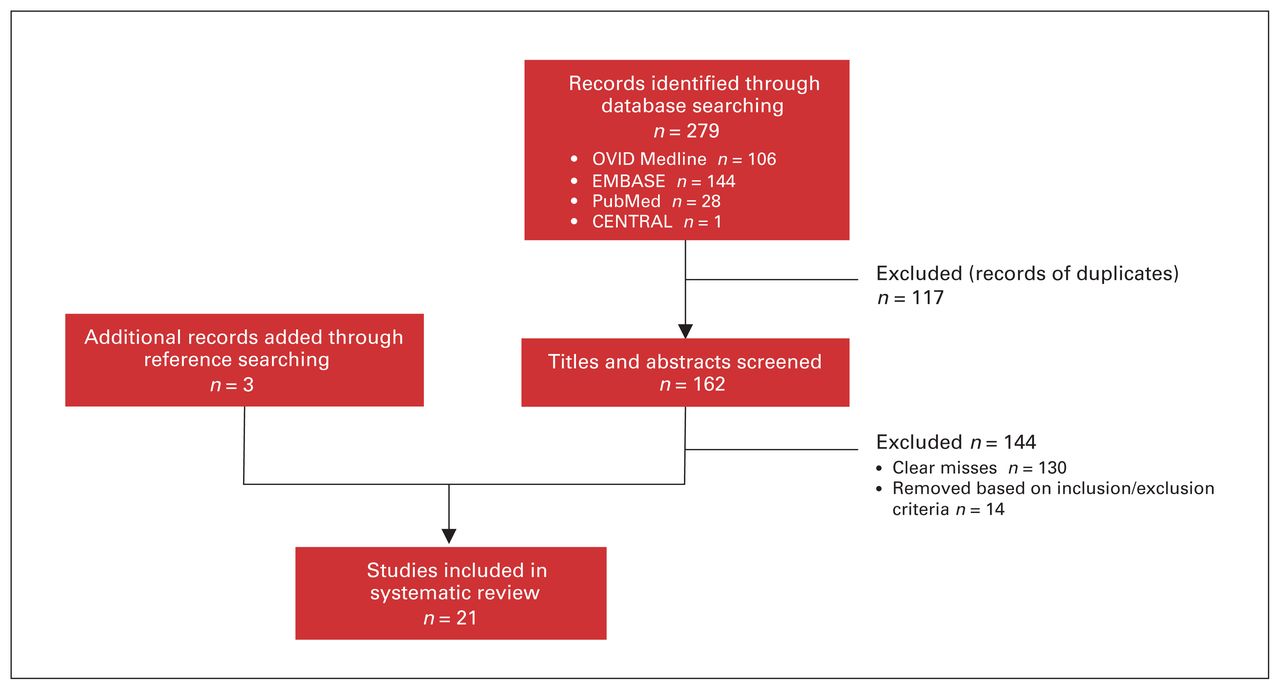
Selection of studies included in the systematic review.
The results of our narrative analysis are included in Table 1. Most of these papers used a single surgical department as their population and were prospective studies. The most frequently used assessment method was self-reported questionnaires, often using a Likert scale. Several studies used a pre- and postintervention questionnaire; unfortunately, some were lacking a preintervention comparison. Narrative analysis of intervention strategies revealed 5 major MMC improvement themes targeted by each intervention strategy: educational value, error analysis, case selection and representation, attendance and dissemination strategies. These results are summarized in Table 2.
Summary of results from a narrative systematic review of studies to improve morbidity and mortality conferences (MMC) in general surgery and subspecialties (part 1 of 3)
Stratification of literature review results into themes, goals, specific interventions and supporting studies
Discussion
Educational value
Most studies included in this narrative systematic review investigated interventions aimed at improving the educational value of MMCs, with the goal of improving resident education and patient safety outcomes. Results were largely determined by self-reported attendee satisfaction and perceived educational value, with few studies empirically testing knowledge obtained. However, clear themes emerged for improving the educational content of MMCs that are consistent with current literature.27,28 Morbidity and mortality conferences should use a standardized presentation format that is succinct, limiting both clinical history and literature review to only pertinent details to ensure ample time for discussion and analysis of the root cause of the adverse event presented. Outcomes associated with this style of MMC included increased presentation quality, increased satisfaction with the MMC, and increased likelihood of identification of remediation strategies. The most commonly used strategies to improve presentation standardization were enforcing a time limit of 15–20 minutes11,29,30 and mandatory brief literature reviews.11,12,29–32 Abu-Zidan and Premadase11 suggest that a 15-minute time restriction focuses debate, deters inappropriate speculation, reduces emotional stress, and maintains audience alertness. Furthermore, Murayama and colleagues30 proposed that shorter presentations allow for greater breadth of complications to be presented, which appeals to a wider audience of surgical residents and faculty.
Other strategies used to standardize presentation format included providing a PowerPoint template29,31 and conforming presentations to an SBAR (situation, background, assessment, recommendation) design12,33 or matrix format. 32,43 Mitchell and colleagues12 found that implementing SBAR not only enhanced presentation quality, but also increased performance on multiple-choice questionnaires based on MMC content. The SBAR format is also relatively easy to implement and requires minimal training. Furthermore, SBAR can be used to quantitatively assess residents’ MMC presentations to facilitate systematic assessment and to provide constructive criticism for teaching residents how to deliver informative MMC presentations. 33 Bhalla and colleagues32 found that matrix format increased learning, enhanced presentation quality and was significantly preferred to the traditional MMC format by attendees.23,43 Matrix format involves a skilled moderator who selects cases, assists residents with their presentation preparation, facilitates discussion at the MMC, and implements quarterly examinations pertaining to the cases presented. While this strategy is effective, it appears labour intensive and requires a talented and dedicated moderator.
Other interventions used to improve MMC educational value aimed to increase audience interaction and enhance continuity. Consistent with the current emphasis on reducing didactic learning in medical education, we found that strategies aimed at increasing audience interaction resulted in increased perceived educational value, improved clinical confidence related to MMC content and enhanced identification of errors.12,30,32,35,36 Methods used to increase audience interaction included MMC moderator–stimulated discussion,12,30,35,36 use of an audience response system32 and questions directed to specific audience members.36 Prince and colleagues36 suggest that direct examination of a presenter is beneficial only if facilitated by a moderator who actively engages the audience and explicitly states the implications of the question(s) being asked. More broadly, the creation of a safe MMC environment by facilitators helps encourage participants to ask questions and to collectively advance their understandings of the clinical problems at hand.44 Consistent with literature on collaborative adult learning, a focus on discussion also capitalizes on the unique opportunity MMCs present for novices and experts to engage together to teach and learn from each other in the moment.2,44 Furthermore, collaboration and small group–based discussion may also improve error analysis.45 In regards to MMC continuity, assigning research questions or evidence-based literature reviews32,39 to residents in order to clarify questions arising from previous MMCs increased perceived continuity. Greco and colleagues39 investigated a pilot intervention that incorporated a clinical librarian in their MMCs. The role of the librarian was to help residents make better use of evidence-based medicine by assisting them with researching unanswered questions arising from MMCs for presentation at the following MMC. Alternatively, Bhalla and colleagues32 assigned residents weekly readings or literature reviews pertaining to the pathophysiology, treatment and complications presented at the MMC.
While research linking the effectiveness of MMCs at improving patient outcomes is limited,46 we can theorize that by enhancing the educational value of MMCs, we are not only establishing better trainee education, but also contributing to quality improvement. It is reasonable to believe that if residents or staff physicians are well educated on patient safety issues, they will be less likely to encounter similar issues in their future careers. It is thus prudent to recognize that discussion regarding strategies to improve MMC educational value, such as standardizing presentation format, increasing audience interaction, and enhancing continuity, also represent strategies to address quality improvement and patient safety issues. Standardizing case presentation has previously been found to be associated with increased perception of MMC effectiveness as a quality-improvement tool.46 Most studies identified in this narrative systematic review used interventions to improve the educational content and value of MMCs, which may be attributable to the dual role of the educational value of MMCs in resident education and quality improvement.
Error analysis
In order to identify patient safety issues and act as an effective quality-improvement tool, all MMCs should include discussion or analysis focused on the root cause of a complication. 44 Berenholtz and colleagues15 suggested that 3 elements are necessary to learn from adverse events: individuals involved in the case must be involved in the error analysis, a structured framework should guide identification of contributing factors, and implementation of future preventative strategies must be assigned as a responsibility to an individual or team. Unfortunately, current analysis is largely retrospective and relies on practitioner experience or insight, with few programs using a structured approach.28 We identified 2 strategies for improving error analysis: focused discussion on causative factors12,29,41 and taxonomic error analysis.35,42 These strategies involve using systematic analysis such that a complication is first identified as being caused by a potential quality issue and then analyzed for the root cause. Cromeens and colleagues42 use a template in their MMCs that includes patient identifiers, event summary, preventability and failure mode categories, discussion points and action items with implementation timelines. They further incorporated a rating of preventability based on MMC discussion with management and achieved through consensus. Similarly, Clarke and colleagues35 suggest categorizing error into taxonomies such as domain, impact, type, cause and prevention. Both systematic strategies improve MMC error analysis by defining causative factors other than human error and surgical disease to affect patient safety outcomes.
While not addressed by the studies included in this narrative systematic review, another limitation of MMC error analysis is that MMCs commonly have a strict focus on systematic issues, such as medication administration, communication and handover, while omitting discussion regarding cognitive psychology, or the biases that contributed to error via flawed clinical reasoning.47 Such omissions mean that our capacity to solve patient safety and quality-improvement problems is limited, as MMC error analysis does not fully address human error in identification and discussion of the root cause of an adverse event. The inclusion of metacognition, or “thinking about thinking,” may further enrich error analysis discussion by addressing this commonly negated facet of error. Katz and Detsky47 recommend that, with considerable internal analysis and self-reflection, experienced clinicians could share personal stories in MMCs that highlight how cognitive bias leads to error, thus normalizing cognitive biases and acknowledging that even the most experienced clinicians are not impervious to them. Identification of both cognitive misstep and system problems is essential in the complete discussion of potential patient safety concerns in order to identify remediation strategies. Typically, MMCs are well-focused on education; however, it is their function in quality improvement that often falls short.48 Hopefully, with inclusion of metacognition in MMC error analysis as well as system problems, using tools such as focused discussion on causative factors and taxonomic error analysis, MMCs can better serve as the cornerstone of quality improvement in surgical departments around the world.
Case selection and representation
Case selection and representation remains an essential part of the MMC. Appropriate representation should identify common and recurrent adverse outcomes that occur in a specific hospital setting. This necessitates the need for accurate data recording. The traditional MMC method of tracking adverse outcomes has been criticized, as it is often performed without standard definition of complications and is largely heterogeneous among institutions. 8 Several studies have shown that MMCs tend to underreport morbidity and mortality.17–21 Hutter and colleagues18 provide several explanations for this phenomenon, such as not reporting patients with primarily nonsurgical problems, lack of patient ownership as patients are transferred among physicians, and not reporting adverse outcomes for fear of punishment.
The National Surgical Quality Improvement Program (NSQIP) has been identified as an alternative to the traditional MMC method of data collection.17–20 It uses 30-day prospective data collection and categorizes complications with standard definitions. Several studies comparing NSQIP and traditional MMC data collection methods found that morbidity was consistently underreported by MMCs not using NSQIP, and in most cases, mortality was also underreported. For example, a study performed at Massachusetts General Hospital revealed that mortality and morbidity rates as reported by MMCs were 0.9% and 6.4%, respectively, whereas, NSQIP reported 1.9% mortality and 28.9% morbidity. Proportions of morbidity categories were also underreported in MMCs compared with NSQIP.18 However, limitations with NSQIP have been identified. Adverse outcomes in patients who are admitted to the general surgery unit but do not undergo surgery are not captured by NSQIP.19 Barriers to implementing NSQIP have also been reported, including preconceived notions of inability for NSQIP data to lead to change, feelings that NSQIP is not relevant to a surgeon’s individual practice, and the financial cost of implementing and maintaining NSQIP.17
Data collection systems other than NSQIP have also been reviewed. A recent retrospective study found morbidity reporting increased by using data collected with a hybrid electronic medical registry (HEMR) compared with traditional MMC methods.34 A paper-based proforma following the NSQIP platform was developed by McVeigh and colleagues,21 which also increased capture of morbidity and mortality. The proforma included patient identifiers as well as check boxes to document complications and was inserted into the patient’s chart. The use of a predefined framework for case selection and standardized data collection methods can help optimize case representation at MMCs and improve capture of local morbidity and mortality; however, the local culture of adverse event reporting will also influence the accuracy of data collection.
Attendance
A combination of retrospective and prospective studies evaluated interventions to increase MMC attendance. Teleconferencing led to increased attendance in settings where multiple medical centres existed in geographic separation and with increased commuting distance.37,38 In addition, a net cost–benefit analysis was positive owing to the significant reduction in travel time with teleconferencing.38 Despite the potential for decreased audience interaction, no difference in learning or perception among faculty, residents and students was demonstrated after implementation of a teleconferencing system.37 Murayama and colleagues30 conducted a prospective study in which they modified the time of their MMC from 6 pm after grand rounds to 7 am before the operating day. The schedule change resulted in increased faculty and resident attendance. Possible explanations include increased energy in the morning, fewer scheduling conflicts, and a new indication of departmental priority. Despite few studies in this area, it appears that improving attendance requires interventions targeted at locally identified challenges.
Dissemination
Dissemination of the MMC content allows for continued learning, continuity and, ultimately, translation of knowledge into quality-improvement initiatives. Three strategies identified to disseminate information from MMCs were post-MMC newsletters,32 incorporating MMC findings into a plan-do-check-act (PDCA) cycle,40 and surgeon report cards.41 Post-MMC newsletters were created by the MMC moderator and reiterated teaching points, clinical pearls and answers to questions asked at the MMC. Bhalla and colleagues32 reported that most residents found newsletters useful and that faculty used portions of the newsletter for their continued education. A PDCA cycle is a decision-making tool designed to facilitate the translation of scientific hypothesis into a management strategy for implementing proposed plans.49 Vogel and colleagues40 incorporated their MMC into the plan, do, and check steps and found a significant decrease in the rate of anastomotic failure in colorectal surgery; however, it remains to be seen whether these results are generalizable. Creation of surgeon report cards that were sent to individual surgeons and department chairs to highlight quality-dependent factors leading to adverse events has also been reported. While a decrease in age-adjusted mortality was demonstrated, the authors experienced pushback from surgeons regarding the report cards, and the study lacked a preintervention comparison.41 A universal strategy to optimize dissemination of results from MMCs has not clearly been identified and is an area requiring additional research.
Limitations
Our study has several limitations that pertain to the nature of narrative systematic reviews, including the potential for unintentional omission of studies addressing the research question and exclusion of non-English literature.50 Unlike systematic reviews, narrative reviews do not involve quantitative analysis and rely on subjective analysis, which can be subject to bias. Furthermore, analysis was focused on descriptive outcomes with no numerical weighting applied to each intervention. The nature of the studies surveyed also created challenges for this narrative review. Many studies lacked comprehensive description of their MMCs or described heterogeneous MMC protocols, which limits comparison and generalizability of this study. Furthermore, outcomes were mostly self-reported perception of learning or satisfaction, with few quantitative measures. Several studies also lacked a preintervention comparison, generating more speculative results. Finally, in our analysis we highlight specific strategies for improving MMCs; however, several studies often incorporated multiple changes to their MMC format, thus confounding the efficacy of each individual intervention.
Creating learning health systems
Our analysis revealed that surgical MMC format changes targeted improvement in at least 1 of the following themes in order to better serve a dual purpose in education and quality improvement: educational value, error analysis, case selection and representation, attendance, and dissemination. These interventions are detailed in a problem and recommendation format in Table 3. Educational value was maximized with standardized presentation formats using PowerPoint templates or SBAR format, restricting presentations to 15–20 minutes, mandatory brief literature reviews, and increasing audience interactions. Focused discussion on causative factors leading to adverse events and taxonomic error analysis were interventions used to improve MMC error analysis. Case selection was improved by using an electronic clinical data registry, such as NSQIP, moderator-selected cases, and use of a prospective proforma. Attendance was increased with teleconferencing and by scheduling consistent MMCs that occur before the operating day. Finally, dissemination strategies included post-MMC newsletters, incorporating MMCs into PDCA cycles, and surgeon report cards. New strategies such as a safety learning system,51 not yet widely adopted in surgery, have begun to standardize presentation formats, incorporate informatics approaches, embrace the perspectives of all members of modern multidisciplinary teams, and create avenues for action.
MMC problems and recommended interventions
As surgical care becomes more complex and more multidisciplinary, these ideals must be applied more rigorously and on a larger scale to systems of surgical care. The next great opportunity in surgical quality and patient safety may be the creation of learning health systems, “in which surgical science, information technology, and surgical culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the delivery process, and new knowledge captured as an integral byproduct of the delivery experience.”52 Part of this effort may involve embracing principles of high-reliability organizations: 53 sensitivity to operations, reluctance to simplify, preoccupation with failure, deference to expertise, resilience and collective mindfulness (Table 4). These new perspectives will undoubtedly build on a rich legacy of thought and action on how surgeons reflect on and learn from their mistakes, and how they use new knowledge to constantly improve the care of surgical patients.
Foundational elements of high reliability organizations
Conclusion
Better MMCs, learning health systems and high reliability principles, embedded in inclusive surgical cultures that value and nurture the contributions of all of their members while blurring traditional boundaries between quality and education, have the unprecedented potential to bridge the gap between knowledge and transformative action in surgical care and systems development.
Footnotes
Competing interests: C. Ball is co-editor in chief of CJS; he was not involved in the review or decision to accept this paper for publication. No other competing interests were declared.
Contributors: N. Slater, P. Sekhon, J. Bedford, H. Wong, J. Chiu, E. Joos, C. Ball and S.M. Hameed designed the study. N. Slater, P. Sekhon, J. Bedford and C. Ball acquired and analyzed the data, which N. Bradley and F. Shariff also analyzed. N. Slater, P. Sekhon, F. Shariff and C. Ball wrote the article, which all authors reviewed and approved for publication.
- Accepted August 14, 2019.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.