


Abstract
Background: Robot-assisted coronary bypass (RCAB) surgery has been proposed as an alternative to conventional coronary artery bypass grafting (C-CABG) for managing coronary heart disease, but the evidence on its performance compared to other existing treatments is unclear. The aim of this study was to assess, through a systematic review of comparative studies, the safety and clinical effectiveness of RCAB compared to C-CABG and other minimally invasive approaches for the treatment of coronary heart disease.
Methods: We conducted a systematic review of primary studies in the English-language literature comparing RCAB to existing treatment options (C-CABG, minimally invasive direct coronary artery bypass [MIDCAB] and port-access coronary artery bypass [PA-CAB]) following Cochrane Collaboration guidelines. Meta-analyses were performed where appropriate.
Results: We reviewed 13 studies: 11 primary studies of RCAB (v. C-CABG in 7, v. MIDCAB in 3 and v. PA-CAB in 1) and 2 multicentre database studies (RCAB v. non-RCAB). The overall quality of the evidence was low. Most studies showed no significant benefit of RCAB over other treatments in a majority of outcome variables. Meta-analyses showed that RCAB had lower rates of pneumonia or wound infection than C-CABG, and shorter intensive care unit length of stay than C-CABG or MIDCAB. Individual studies showed that RCAB had some better outcomes than C-CABG (ventilation time, transfusion, postoperative pain, hospital length of stay) or MIDCAB (transfusion, postoperative pain, time to return to normal activities, physical functioning and hospital length of stay). The review of the database studies showed that RCAB was statistically superior to non-RCAB approaches in postoperative pain, renal failure, transfusion, reoperation for bleeding, stroke and hospital length of stay; however, the difference between the 2 groups in several of these outcomes was small.
Conclusion: Although the findings from this review of comparative studies of RCAB appear promising and suggest that RCAB may offer some benefits to patients, in the absence of randomized controlled trials, these results should be interpreted cautiously.
Traditionally, coronary artery bypass grafting (CABG) was performed via conventional sternotomy and with a cardiopulmonary machine (i.e., conventional coronary artery bypass grafting [median sternotomy] [on pump] [C-CABG(on)]). Later, off-pump techniques (median sternotomy) (C-CABG [off]) and other minimally invasive procedures performed through a minithoracotomy (minimally invasive direct coronary artery bypass [MIDCAB] and port-access coronary artery bypass [PA-CAB]) were developed. Most recently, the introduction of the da Vinci system has led to new robotic surgical approaches (robotic coronary artery bypass [RCAB]), including robot-assisted direct coronary artery bypass and totally endoscopic coronary artery bypass.
A 2016 systematic review of comparative and noncomparative studies of robot-assisted direct coronary artery bypass, totally endoscopic coronary artery bypass and MIDCAB showed acceptable and comparable perioperative mortality rates for all procedures.1 The authors reported on intraoperative details as well as postoperative outcomes and concluded that, despite the limitations of clinical evidence available at the time, findings from their review should be considered a useful benchmark for future studies.
Owing to the lack of evidence about the advantages of RCAB over other surgical techniques, its uptake is still challenged by several limitations, including concern over intraoperative conversion, anastomosis time and anastomotic patency, heterogenicity of clinical outcomes, evolving instrumentation and cost.1,2 The aim of the present study was to assess, through a systematic review of comparative studies only, the safety and clinical effectiveness of RCAB compared to C-CABG and other minimally invasive approaches (MIDCAB and PA-CAB) for the treatment of coronary heart disease.
Methods
We conducted a systematic review of published peer-reviewed primary studies comparing RCAB to C-CABG, MIDCAB or PA-CAB following Cochrane guidelines.3
Literature search
We conducted a comprehensive literature search to identify relevant primary studies comparing RCAB to C-CABG, MIDCAB or PA-CAB. We developed structured search strategies and applied them to the following bibliographic databases: PubMed (MEDLINE and other sources), Embase, Web of Science, Clinical Trials.gov, The Cochrane Library, CINAHL, Econ-LIT, PsycINFO, and the Centre for Reviews and Dissemination (DARE, NHS EED and HTA). The strategies combined relevant key words with controlled vocabulary terms (Medical Subject Headings and Emtree terms) such as coronary artery bypass, robotic surgical procedures and minimally invasive surgical procedures. Keywords included robotic surgery, robot-assisted surgery and da Vinci. Full details of the literature search are presented in Appendix 1 (available at canjsurg.ca/013318-a1). The initial search was performed in October 2017. We performed monthly update searches in PubMed and Google scholar alerts throughout the project to capture any additional studies published after the initial search; the last update was completed in April 2018. All searches were limited to human studies reported in English. No study design filters were applied.
For completeness, we conducted a manual search of the reference lists of relevant papers located through the electronic searches. Results from each of the searches were compiled and entered into a single Reference Manager v. 12 (Thomson ResearchSoft) database, after which duplicate citations were removed.
Study selection
Two reviewers (F.H., F.N.) independently screened the titles and abstracts of all citations to identify studies for full-text review. Both reviewers retrieved and assessed the full-text papers for inclusion and exclusion according to the eligibility criteria (Table 1). Disagreement was resolved through discussion.
Study eligibility criteria for review on safety and clinical effectiveness of robotic coronary artery bypass
Data extraction
Each reviewer independently extracted information from studies using a standard data extraction form. The elements extracted were study design, setting, methods, sample size, baseline characteristics, details of the intervention and comparator, and outcome measures. Data extraction was cross-checked by the 2 reviewers, and disagreements were resolved through discussion.
Assessment of study quality
We used the Cochrane Collaboration Risk of Bias Tool to critically appraise any randomized trials. We appraised the methodologic quality of nonrandomized trials with the Newcastle–Ottawa Scale,4 a visual tool containing 8 items over 3 domains: selection (4 items), to determine the representativeness of participants and assess the presence of selection bias; comparability (1 item), to determine the presence or control of confounding variables; and outcome/exposure (3 items), to determine the adequacy of ascertainment of outcomes and follow-up. Each item in the selection and outcome domains can be awarded a maximum of 1 star, and the item on comparability up to 2 stars. Three possible ratings can be given to studies: poor quality (0 stars in the comparability domain, or 0 or 1 star in the selection or outcome domain), fair quality (2 stars in the selection domain) or good quality (3 or 4 stars in the selection domain).
We used the GRADEpro tool (Grading of Recommendations Assessment, Development and Evaluation)5 to assess the overall quality of the body of evidence for key outcomes. With this tool, the quality of outcomes is rated over 6 domains: study design, risk of bias, inconsistency, indirectness, imprecision and other factors, including publication bias, a large effect size, a dose–response gradient and other plausible confounders. This approach can yield 4 grades, ranging from very low to high confidence in the overall quality of evidence. In the current study, the GRADE assessment of the quality of evidence was based on the following outcomes: length of hospital stay, late myocardial infarction (MI), late stroke, overall survival, postoperative pain score, readmission rate within 30 days and revascularization rate.
Data analysis and synthesis
We tabulated data extracted from included studies to facilitate quantitative and qualitative analysis. Data were assessed for potential meta-analysis.
Characteristics of included studies and findings were synthesized narratively.
We conducted meta-analyses using a random-effects model6 to calculate the summary statistics. A p value of < 0.05 was considered statistically significant. We pooled studies reporting continuous data using the mean difference between surgical groups, and those reporting categoric data using odds ratio. We assessed heterogeneity using the I2 statistic. When heterogeneity was 50% or more,3 it was considered substantial, and the studies were not pooled. In cases of multiple studies published from an institution with overlap of patients and the same outcome measures, we included only the most recent publication and largest sample in the synthesis. We used RevMan software version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration) to conduct the meta-analyses.
Results
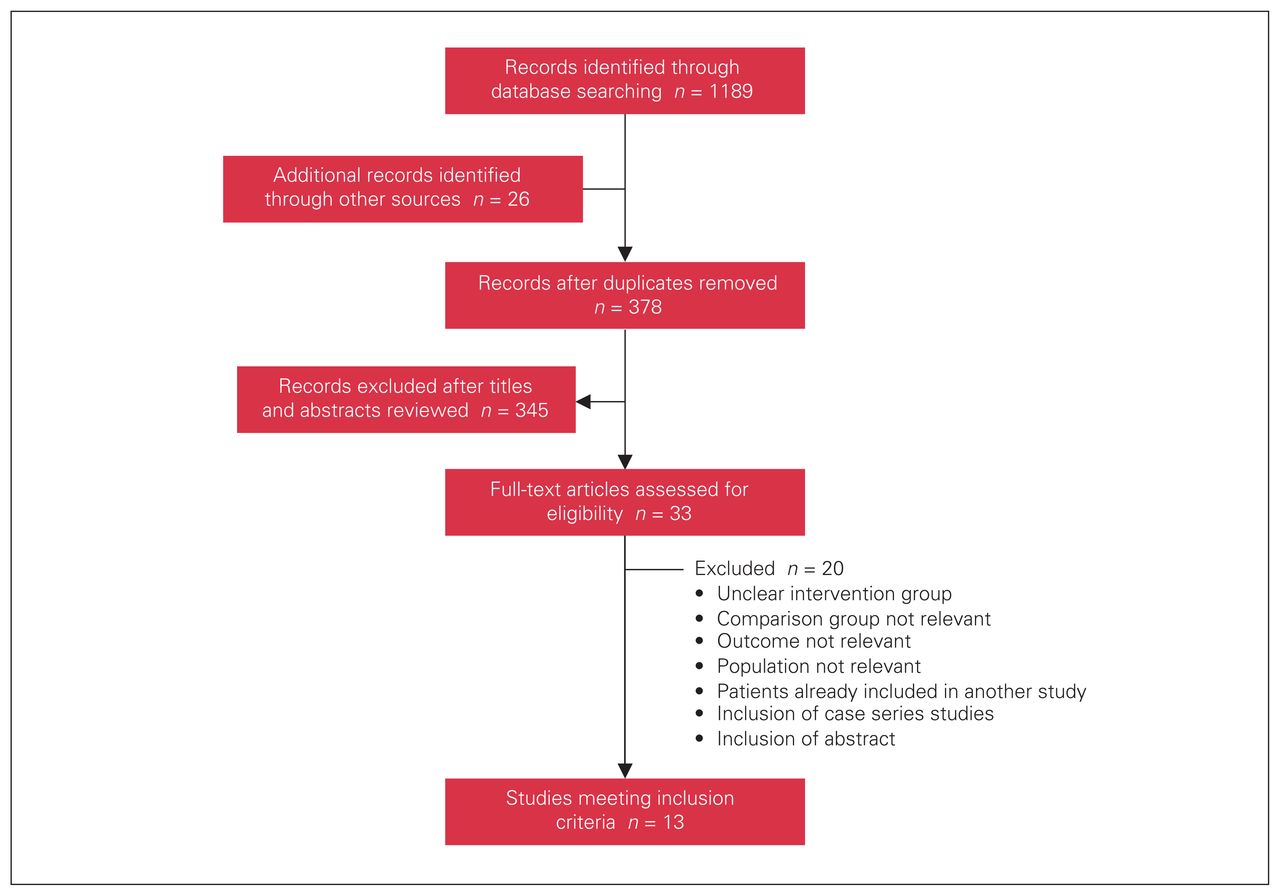
In total, 1215 citations were retrieved through the literature searches, and 33 full-text articles were assessed (Fig. 1). Of these, 13 were included in the review.7–19 Detailed descriptions of included and excluded studies can be found in Appendix 1.

Flow diagram showing study selection.
Seven of the 13 studies were conducted in the United States, 2 in France, 1 in Germany, 1 in China, 1 in Taiwan and 1 in Turkey. Two studies were based on national databases,10,11 and the remaining 11 studies were singlecentre.7–9,12–19 Patients were selected between 1998 and 2014, and sample sizes ranged from 38 to 966 211. Seven studies compared RCAB to C-CABG, on or off pump,7,12–17 3 studies compared RCAB to MIDCAB,17–19 and 1 study compared RCAB to PA-CAB.9 The 2 multicentre studies investigated differences between robotic and nonrobotic CABG.10,11 None of the studies were randomized controlled trials. Three were prospective cohorts,7,17,19 and the remainder were retrospective cohorts. Four studies were propensity score matched.11–13,16
Study quality
With the GRADEpro tool, the quality of studies comparing RCAB to other surgical modalities (C-CABG, MIDCAB and PA-CAB) was rated as low to very low (Table 2). With the Newcastle–Ottawa Scale, quality was rated as good in 1 study,11 fair in 2,12,13 and poor in 10.7–10,14–19
GRADE (Grading of Recommendations Assessment, Development and Evaluation)5 assessment of included studies
Selection bias
In 5 studies, the selection of patients for the control and intervention groups was unclear or not the same.8,9,12,16,17 Three of the 5 did not state whether the eligibility criteria were the same between the RCAB group and the control group.12,16,17
In 2 studies, patients were selected for the intervention and control groups based on availability of the technology and patient’s and surgeon’s preference.8,9 With the exception of those based on national databases,10,11 all of the studies failed to show that the selected cohort was representative of the general population with coronary artery disease. In all studies, medical records or institutional databases provided information on patients’ baseline characteristics.
Confounding
Four studies used propensity scoring to match patients and controls for potential imbalances in age, cardiac comorbidities and noncardiac comorbidities.11–13,16 The other studies did not attempt to control for confounding variables during selection of patients or at the statistical analysis stage.
Detection and attrition bias
Apart from 1 study that used self-reported measurements,17 investigators extracted information on outcome measures from medical records and institutional databases. Most studies had an appropriate follow-up time, since they measured operative and perioperative outcomes. However, in 4 studies examining long-term outcomes, patients were followed for a short period, or the follow-up time differed between the intervention and control groups.8,9,11,18 The presence of attrition bias was unclear in 4 studies, as the investigators did not report the number of patients lost to follow-up.8,9,14,17 Further details on GRADE and methodologic quality assessment are presented in Appendix 1.
Patient characteristics
With 1 exception,14 the mean or median age across studies ranged from 55 to 70 years (Table 3). The majority of participants (59%–100%) were men. The mean or median left ventricular ejection fraction ranged from 52% to 64%. Most studies included only elective cases of CABG.
Characteristics of participants
Surgical procedure
Procedure: Two single-centre studies used the da Vinci system for totally endoscopic coronary artery bypass9,15 (Appendix 1, Supplemental Table S1). In the remaining single-centre studies, robotic-assisted direct coronary artery bypass, in which the anastomosis is performed manually, was used.7,8,12–14,16–19 Nineteen percent to 22% of patients in the national database studies who had RCAB underwent surgery with the use of a cardiopulmonary bypass machine (on pump).10,11 All patients in the remaining studies underwent RCAB off pump. Six of the comparative studies included patients who had C-CABG(on),7,12–15,17 and 1 included those who had C-CABG(off) only.16 Most procedures involved the use of the internal thoracic artery as the graft.
Number of grafts: Two studies were limited to patients with single-vessel coronary heart disease,14,15 and 1 study excluded them.16 Where reported, the mean or median number of grafts for RCAB ranged from 1 to 3, whereas the mean or median number of grafts for C-CABG was 3 or 4. In 1 study of MIDCAB, there was a statistically significantly higher proportion of patients with 1 graft in the MIDCAB group than in the RCAB group.18 The remaining studies comparing RCAB to MIDCAB or PA-CAB provided no information on the difference in number of grafts between groups.
Surgeons: In 4 studies, surgical procedures in the control and intervention groups were performed by a single surgeon or surgical team.7,14,16,19 One of the remaining studies simply described surgeons as being experienced with robotic technology,12 and the rest provided no information on surgeon experience.
Hybrid coronary revascularization: Some patients with multivessel coronary heart disease who underwent a minimally invasive procedure also had a percutaneous coronary intervention. Where reported, the rates of hybrid coronary revascularization in studies of minimally invasive non–robot-assisted procedures ranged from 0% to 48%.7,12,15,18 In 1 study of RCAB, all patients had a percutaneous coronary intervention for other coronary vessels.18 Across studies, the timing of percutaneous coronary intervention varied between 0 (i.e., performed at the same time) and 14 days after CABG. Most hybrid coronary revascularization procedures were performed with drug-eluting stents.
Safety
Conversion to C-CABG: Six studies reported rates of conversion to C-CABG from RCAB ranging from 0% to 5% (Table 4).8,9,12,14,15,18 One study comparing RCAB and MIDCAB showed no differences in rates between these 2 approaches.18 Jegaden and colleagues9 compared conversion rates of RCAB and PA-CAB, and reported none in either group.
Postoperative complications: One study comparing RCAB to C-CABG(on) showed no differences in rates,7 but Poston and colleagues16 reported that patients who underwent RCAB had lower rates of major complications than those who underwent C-CABG(off). One national database study showed significantly higher rates of major complications in the nonrobotic group than in the robotic group.10
Myocardial infarction: Three studies compared MI rates between RCAB and C-CABG.7,12,16 Rates ranged from 0% to 7%, and no differences between groups were found. One of the 2 studies comparing RCAB and MIDCAB showed no significant difference in MI rates between the 2 groups.15 The second study showed significantly lower rates with RCAB; however, this difference disappeared after adjustment for baseline covariates with a propensity score model.19 The single study of PA-CAB showed similar rates of MI as for RCAB.9
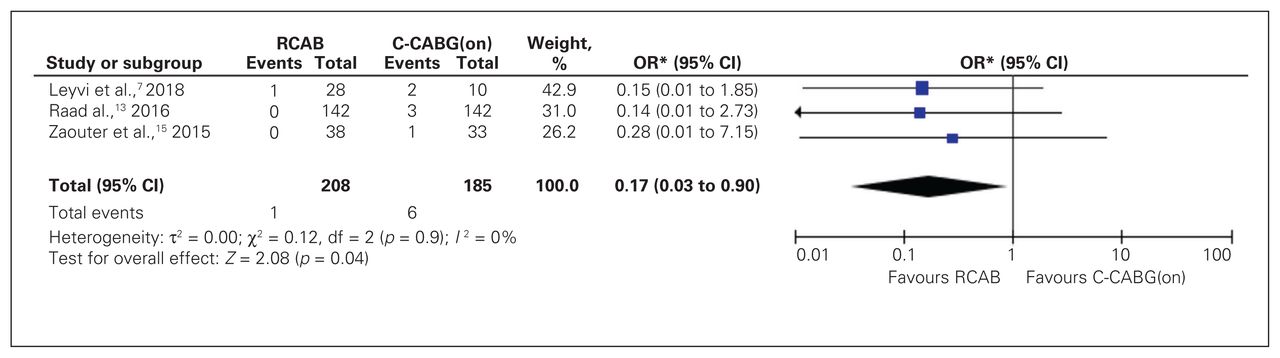
Stroke: Postoperative stroke rates were provided in 4 studies of patients who underwent RCAB or C-CABG.7,13,15,16 A meta-analysis of 3 studies on RCAB versus C-CABG(on) showed no significant difference between the 2 procedures (Fig. 2). The single study on RCAB versus C-CABG(off) also showed no significant difference.16 In 1 study comparing RCAB and PA-CAB, stroke rates were 0% and 2%, respectively (p value not reported).9 No studies reported postoperative stroke rates among patients who underwent MIDCAB, but the 2 national database studies compared rates between robotic and nonrobotic procedures.10,11 Although both studies showed lower rates for stroke, only 1 showed a significant difference between groups, favouring RCAB.11
Atrial fibrillation: Rates of atrial fibrillation varied from 9% to 20%, and no significant differences between patients who underwent RCAB versus C-CABG were reported.14–16 One study comparing patients who had RCAB as well as a percutaneous coronary intervention to those who had MIDCAB showed no significant differences in atrial fibrillation rates (16% v. 30%).19 However, in 1 other study of the same comparators that showed no significant differences among patients who underwent hybrid coronary revascularization, significantly higher rates of arrhythmia were observed in the MIDCAB group than in the RCAB group.18
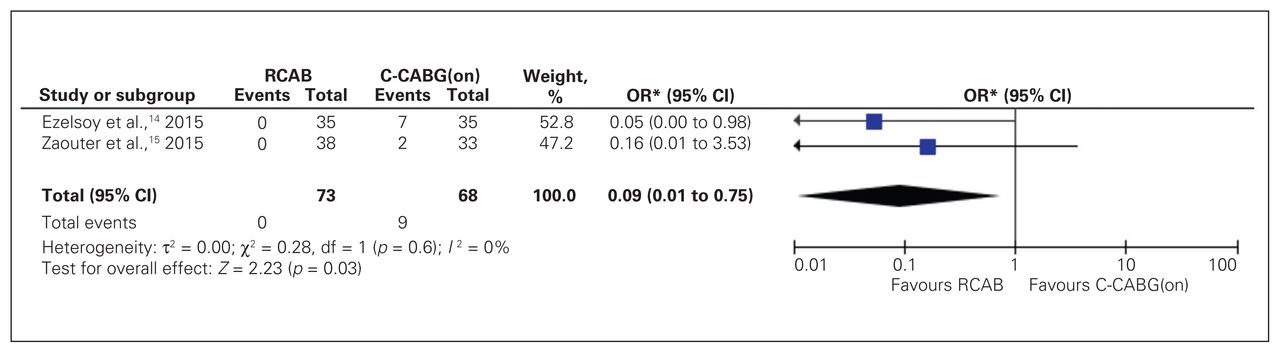
Infection: Of the studies comparing RCAB and C-CABG, 3 provided information on wound infection,7,13,15 2 provided information on pneumonia14,15 and 1 provided information on major infections.16 Meta-analyses showed that RCAB was associated with significantly lower rates of wound infection (Fig. 3) and pneumonia (Fig. 4) than C-CABG(on). There was no significant difference in rates of major infections between RCAB and C-CABG(off). One study of MIDCAB versus RCAB presented rates of wound infection after CABG; no significant differences were found.18 None of the studies reported on infection rates after PA-CAB. However, 1 national database study showed no significant difference in infection rates between patients who underwent robotic and those who underwent nonrobotic surgery.11
Renal failure: Three studies comparing RCAB to C-CABG showed postoperative renal failure rates ranging from 0% to 6%.12–14 The pooled estimate of studies on RCAB and C-CABG(on) showed no differences between approaches (Fig. 5). One study of MIDCAB versus RCAB showed no significant differences in renal failure rates.18 One national database study showed a significant difference, favouring robotic over nonrobotic CABG.10 However, the other national database study showed no significant difference in renal failure rates.11

Meta-analysis of postoperative stroke from comparative studies of robotic coronary artery bypass (RCAB) versus conventional coronary artery bypass grafting (on pump) (C-CABG[on]). *IV random. CI = confidence interval; OR = odds ratio.
Meta-analysis of wound infection from comparative studies of robotic coronary artery bypass (RCAB) versus conventional coronary artery bypass grafting (on pump) (C-CABG[on]). *Mantel–Haenszel random. CI = confidence interval; OR = odds ratio.
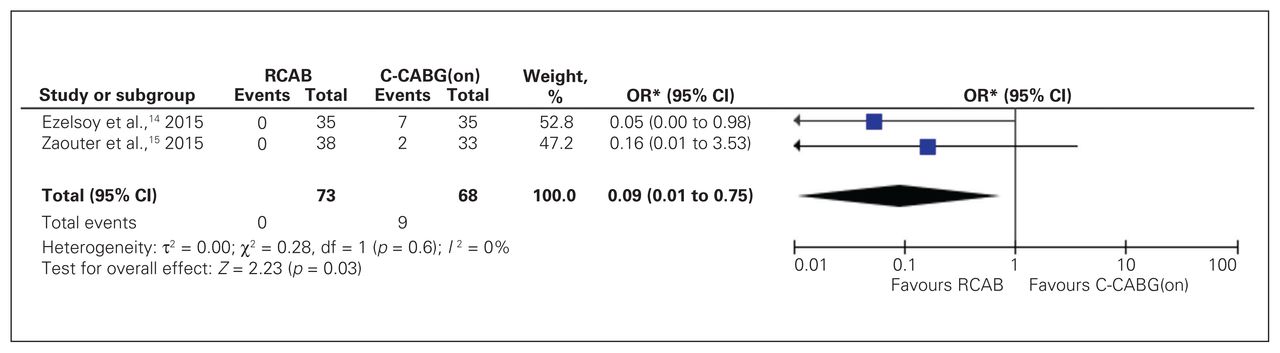
Meta-analysis of pneumonia from comparative studies of robotic coronary artery bypass (RCAB) versus conventional coronary artery bypass grafting (on pump) (C-CABG[on]). *Mantel–Haenszel random. CI = confidence interval; OR = odds ratio.

Meta-analysis of renal failure from comparative studies of robotic coronary artery bypass (RCAB) versus conventional coronary artery bypass grafting (on pump) (C-CABG[on]). *Mantel–Haenszel random. CI = confidence interval; OR = odds ratio.
Safety
Outcomes
Operative outcomes
Cardiopulmonary bypass time: One national database study showed no significant difference in cardiopulmonary bypass time between arrested-heart robotic and nonrobotic procedures (88 min v. 90 min, p = 0.2).10 The remaining studies used off-pump techniques during RCAB.
Harvest duration time: None of the studies compared harvest duration time between RCAB and other surgical approaches. One study indicated that the mean harvest time for the RCAB group was 48 minutes.14
Anastomosis time: Zaouter and colleagues15 reported an average anastomosis time of 60 minutes during RCAB. There were no studies comparing anastomosis time between CABG techniques.
Postoperative outcomes
Ventilation time: In 6 studies comparing RCAB and C-CABG, the investigators reported on differences in mean ventilation time7,13–17 (Table 5). The mean time for RCAB ranged from 0.4 to 16 hours, whereas the mean time for C-CABG ranged from 3 to 14 hours. In 4 of these studies, mean ventilation times were significantly longer for patients who underwent C-CABG than for those who had RCAB.7,13,14,16 For MIDCAB, different results were reported in 2 studies. One showed that a significantly higher proportion of patients who underwent RCAB than underwent MIDCAB had been extubated within 6 hours or less after surgery,18 whereas the second study showed no significant difference between the 2 approaches.17 In a study of RCAB versus PA-CAB, the mean ventilation times for RCAB and PA-CAB were 5 hours and 8 hours, respectively;9 the investigators did not provide the statistical significance of the results. One national database study showed that a significantly higher proportion of patients in the nonrobotic group than in the robotic group required ventilation beyond 24 hours.10
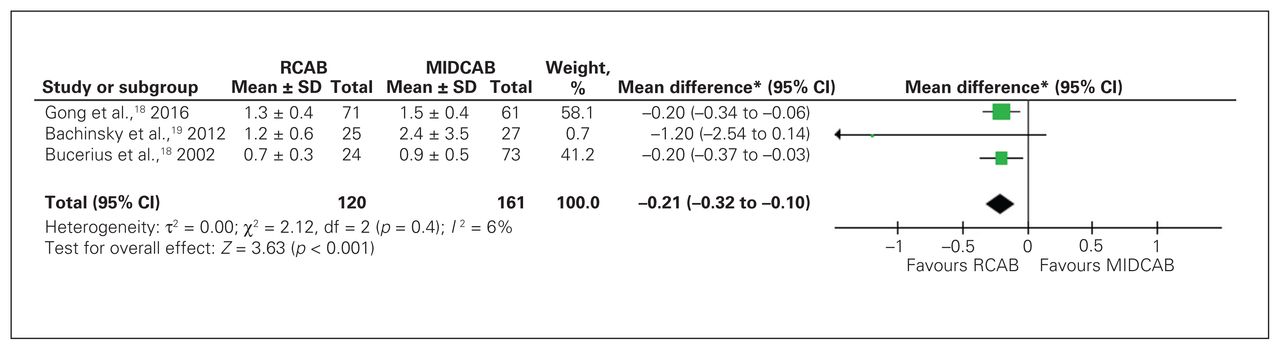
Intensive care unit stay: Seven studies of RCAB versus C-CABG reported on differences in intensive care unit (ICU) stay.7,8,12,14–17 A meta-analysis of 2 studies showed that stays were significantly longer after C-CABG(on) (Fig. 6). The pooled estimate of 3 studies on MIDCAB showed shorter ICU stay after RCAB (Fig. 7).
Transfusion: Three studies compared transfusion rates between RCAB and C-CABG(on).7,12,15 One showed no significant difference,7 whereas 2 showed significantly lower rates in the RCAB group.12,15 Transfusion rates with RCAB and C-CABG(on) ranged from 4% to 26% and from 20% to 58%, respectively. Two studies comparing RCAB to MIDCAB showed different results regarding transfusion rates.18,19 In 1 study, rates were similar (15% v. 18%, p = 0.7),18 whereas in the other, they were significantly higher for MIDCAB (67% v. 12%).19 One national database study showed significantly higher transfusion rates among patients who underwent nonrobotic CABG for single and multiple bypasses than among those who underwent robotic CABG.11
Reoperation for bleeding: Rates of reoperation for bleeding were low (0%–8%). In three studies, they were similar for patients who underwent C-CABG and those who had RCAB.13,15,16 One study comparing RCAB and MIDCAB provided information on the number of patients requiring reoperation due to bleeding; no significant differences were found between groups.18 In the single study of PA-CAB versus RCAB, rates of 2% and 8% for PA-CAB and RCAB, respectively, were reported (p value not provided).9 One national database study showed that the difference of 0.3% in rates was statistically significant and was in favour of the robotic group.10
Postoperative pain: In 4 studies comparing RCAB and C-CABG, pain was measured with different instruments. Pain was assessed through scales in 2 studies, which showed higher pain scores among patients who underwent C-CABG(on) at postoperative day 3–7 than among those who underwent RCAB.14,17 In a third study, pain was measured through use of narcotic medication; the RCAB group required significantly lower dosages during the hospital stay than the C-CABG group.13 However, the fourth study showed no differences in duration of incisional pain between patients who underwent RCAB and those who had C-CABG( off) (13 d v. 27 d).13 Different instruments to measure postoperative pain were also used in 3 studies of MIDCAB versus RCAB.17–19 In 1 study, a higher proportion of patients who underwent MIDCAB had intercostal pain for 3 days (16% v. 6% for RCAB, p = 0.04).18 In the other 2 studies, scales were used to assess pain.17,19 One study showed no significant differences in scores between the groups during the hospital stay or on discharge.19 The second study also showed no differences in pain scores 1–2 days after surgery, but lower scores were observed in the RCAB group than in the MIDCAB group at postoperative days 3–7.17

Meta-analysis of intensive care unit length of stay from comparative studies of robotic coronary artery bypass (RCAB) versus conventional coronary artery bypass grafting (on pump) (C-CABG[on]).*IV random. CI = confidence interval; SD = standard deviation.

Meta-analysis of intensive care unit length of stay from comparative studies of robotic coronary artery bypass (RCAB) versus minimally invasive direct coronary artery bypass (MIDCAB). *IV random. CI = confidence interval; SD = standard deviation.
Postoperative outcomes
Short- and long-term outcomes
Angina: One study comparing RCAB to MIDCAB provided information on angina rates after the procedure18 (Table 6). During 22 months (range 12–60 mo) of follow-up, no significant differences were reported. Rates with RCAB and MIDCAB were 6% and 7%, respectively. In the single comparative study on PA-CAB, 3-year angina-free survival rates were 85% for patients who underwent RCAB and 94% for those who underwent PA-CAB (p value not provided).9 None of the studies measured angina after C-CABG.
Late MI: One study showed late MI rates for RCAB and C-CABG of 5% and 4%, respectively; the difference was not statistically significant.8 Gong and colleagues18 measured late MI during 22 months of follow-up in patients who went RCAB or MIDCAB and found that the rates were low and were similar for the 2 approaches (3% and 2%). In the single study of RCAB versus PA-CAB, only 1 case (2%) of late MI was observed, in the PA-CAB group.9
Late stroke: In 1 study comparing RCAB to C-CABG(off)16 and another comparing RCAB to MIDCAB,18 the investigators reported on late stroke rates after surgery. There were no significant differences between RCAB and C-CABG(off) or MIDCAB,
Graft stenosis: One study comparing RCAB and C-CABG(off) presented information on graft stenosis.16 During 1 year of follow-up, there was only 1 case of stenosis in the entire group. The single study that compared RCAB to PA-CAB indicated that graft stenosis rates were 5% and 0%, respectively.9
Graft failure: Two studies provided information on graft failure after RCAB and C-CABG.15,16 In 1 study, no significant differences between approaches were found.15 In the other study, 20 cases of graft failure involving saphenous vein grafts were observed in the C-CABG group.16 One study presented graft failure rates after RCAB and PA-CAB: rates were low and were similar for the 2 approaches (5% and 0%).9
Revascularization: Differences in revascularization rates between RCAB and C-CABG were provided in 2 studies.7,16 Both showed low rates and no significant differences between approaches. One study compared revascularization rates for RCAB and MIDCAB, which ranged from 0% to 5%.18 No significant differences were found. Jegaden and colleagues9 reported early and late revascularization rates after RCAB and PA-CAB. The early revascularization rates were 0% for PA-CAB and 7% for RCAB, and the corresponding late revascularization rates were 4% and 5%.
Death: Four studies comparing RCAB to C-CABG provided information on mortality rates, which ranged from 0% to 29%.8,12,15,16 Three studies showed no significant differences between surgical groups after 30 days and 1 year of follow-up.12,15,16 Su and colleagues8 reported similar rates of in-hospital death after RCAB and C-CABG, but the overall mortality rate was higher for C-CABG. Mortality rates for RCAB and MIDCAB were presented in 2 studies.18,19 Neither showed significant differences in 30-day mortality rates (Fig. 8), and 1 indicated that rates remained similar throughout 22 months of follow-up.18 Similarly low mortality rates were found after RCAB and PA-CAB (3% and 0%, respectively).9 The 2 national database studies showed no significant differences in short-term mortality rates between robotic and nonrobotic CABG.10,11
Survival: One study provided overall survival rates after RCAB and C-CABG.8 During follow-up of 34–53 months, rates were not significantly different (68% v. 54%). In a study comparing RCAB to MIDCAB, the 5-year overall survival rate was 94% and 88%, respectively, a nonsignificant difference.18 The single study of PA-CAB showed a 3-year overall survival rate of 100% for PA-CAB and 96% for RCAB; the statistical significance of this difference was not reported.9
Time to return to normal activities: One study compared time to return to work or normal activities between RCAB and C-CABG(off).16 Times were significantly shorter for patients who underwent RCAB than for those who underwent C-CABG(off) (44 d v. 93, p = 0.02). Bachinsky and colleagues19 compared time to return to work between RCAB and MIDCAB, and found that the mean time was 37 days for the RCAB group and 57 days for the MIDCAB group, a statistically significant difference (p = 0.01).
Quality of life: Only 1 study comparing RCAB to MIDCAB reported on quality of life 1 month after surgery.19 Physical functioning was significantly better among RCAB patients. However, no differences in mental health were found.

Meta-analysis of 30-day mortality from comparative studies of robotic coronary artery bypass (RCAB) versus minimally invasive direct coronary artery bypass (MIDCAB). *Mantel–Haenszel random. CI = confidence interval; OR = odds ratio.
Short- and long-term cardiac and survival outcomes
Resource-relevant outcomes
Operative time: Three studies reported on operating times for RCAB and C-CABG7,12,16 (Table 7). In 2 studies, operating times were significantly longer for C-CABG(on).7,12 In the third study, times were significantly longer for RCAB than for C-CABG(off).16 The mean operating time in the 3 studies ranged from 162 to 348 minutes for RCAB and from 246 to 306 minutes for C-CABG. Two studies of RCAB versus MIDCAB presented conflicting results. One showed significantly longer times for patients who underwent MIDCAB (261 min v. 386 min, p < 0.001),19 whereas the other showed no significant difference between the 2 approaches (221 min v. 186 min, p = 0.05).18 The study comparing RCAB and PA-CAB showed mean operative times of 204 minutes for RCAB and 192 minutes for PA-CAB; no information on statistical significance was included.9
Anesthesia time: Three studies of RCAB and C-CABG(on) in which anesthesia time was assessed gave conflicting results.7,12,15 Two showed that RCAB was associated with significantly shorter mean anesthesia times,7,12 and the third showed significantly longer anesthesia times for RCAB.15 No information comparing anesthesia times for RCAB and MIDCAB, or for RCAB and PA-CAB was found.
Length of hospital stay: Length of hospital stay was assessed in 6 studies of RCAB versus C-CABG,7,13–17 of which 5 reported significantly shorter stays after RCAB than C-CABG(on) or C-CABG( off).13–17 The mean or median length of hospital stay for RCAB and C-CABC ranged from 4 to 9 days and from 5 to 16 days, respectively. Three studies reported differences in length of stay between RCAB and MIDCAB: 2 studies showed significantly longer stays among patients who underwent MIDCAB,17,18 whereas the other study showed no significant difference between procedures.19 In the single study comparing RCAB and PA-CAB, the mean length of hospital stay was 5.5 days for RCAB and 7 days for PA-CAB; no information on statistical significance was provided.9 One national database study showed that, overall, the length of stay for robotic procedures was significantly shorter than for nonrobotic procedures (4 d v. 5 d, p < 0.001).10 In the other national database study, stays were shorter after robotic surgery among patients who required only 1 bypass but were no different among those who required multiple bypasses.11
Readmission rates: In 2 studies comparing C-CABG( on) and RCAB, there were no significant differences in rates of readmission within 30 days between approaches.13,16 Readmission rates ranged from 4% to 16% in the RCAB group and 9% to 15% in the C-CABG(on) group. None of the studies on minimally invasive procedures (MIDCAB or PA-CAB) provided information on readmission rates.
Resource-related outcomes
Discussion
Cao and colleagues1 referred to contemporary data for C-CABG20,21 and concluded that perioperative outcomes, including MI, atrial fibrillation, stroke, renal failure and reoperation for bleeding, were comparable to those for RCAB. The findings from the present review of comparative nonrandomized studies showed that there were no differences in rates of conversion to C-CABG between RCAB and other surgical techniques. Rates of postoperative complications were significantly lower with RCAB than with C-CABG(off). Robotic coronary artery bypass was comparable if not superior to other surgical techniques regarding the need for blood transfusion or reoperation for bleeding. Patients who underwent RCAB had significantly shorter ICU stays and experienced significantly less pain in the initial days following surgery than those who had C-CABG. Furthermore, RCAB was similar to other bypass techniques with respect to long-term outcomes — including angina, late MI, late stroke, graft stenosis or failure, and the need for revascularization — and in rates of mortality and overall survival. However, as in the review by Cao and colleagues,1 the majority of studies included in the present review involved relatively young patients (in their 60s) with left ventricular ejection fraction within the normal range (50%–70%), and the number of grafts was relatively low, especially in the RCAB group. These characteristics may have affected the overall surgical outcomes.
The follow-up period in the studies included in our review ranged from the length of the hospital stay to 5 years. This variation, together with the fact that only 1 study reported on overall long-term survival for RCAB versus C-CABG, RCAB versus MIDCAB, and RACB versus PA-CAB, makes it difficult to assess long-term survival. Mortality rates (with a follow-up duration of 5 yr) were similar to that reported in a noncomparative study on MIDCAB off pump in which patients were followed for up to 8 years (4%).22
Su and colleagues8 reported that there was a tendency to use RCAB to treat simple cases, since it is more time consuming and technically demanding. Moreover, the techniques and instruments for RCAB are still evolving, and surgical teams are still learning and building their experience. The learning curve associated with RCAB has been well documented, and it takes around 100 operations before adverse outcomes are minimized.23,24 Although every surgeon moves through the learning curve in an individualized fashion, most surgeons experience a greater rate of adverse events over the course of their initial experience with any new surgical technique or modality, including RCAB.
Anesthesia time is variable among centres, likely owing to differences in centre practice of RCAB anesthesia. The use of a double-lumen endotracheal tube rather than a single-lumen tube may change times. As well, the placement of a thoracic epidural catheter changes anesthesia time compared to a single-dose paravertebral block, an intraoperative block or no block.
Resource-related outcomes may depend on several factors, including patients’ characteristics, surgeons’ experience,23,24 presurgical planning,25–27 clinical pathways of each institution, and how outcomes such as operating time, anastomosis time and cardiopulmonary bypass time are measured.1 For example, since there is no sternotomy with RCAB, patients may return to the ICU from the operating room already extubated; if still intubated, they are extubated shortly after completion of surgery. This leads to an expedited ICU course. As well, the lack of sternotomy decreases blood transfusion rates and eliminates the need to restrict mobility for sternal precautions.
Limitations
Several limitations may have affected the findings of this review. First, we did not identify any randomized clinical trials, and all included studies were comparative nonrandomized studies. Thus, confounders are likely to exist. Second, the overall quality of evidence comparing RCAB to other surgical approaches was low, which limited our ability to make strong conclusions regarding the comparison between RCAB and other CABG surgical techniques. Third, although meta-analyses can increase power and precision, they cannot eliminate any biases that exist in pooled studies. Furthermore, in the case of 30-day mortality and complications (e.g., wound infection and renal failure), sample size and number of events were still insufficient to provide pooled results with narrow confidence intervals. Fourth, variation across studies (heterogeneity) was inevitably present. To decrease its presence, we pooled only outcomes measured at similar follow-up intervals, and we did not pool studies that used different surgical techniques (e.g., studies evaluating MIDCAB were not pooled together with studies evaluating C-CABG). Also, results of meta-analyses were used only when the I2 statistic was less than 50%. In addition, as our search was conducted in English, studies that were published only in other languages were not included in this review. Last, the generalizability of the findings of this review to all patients with coronary artery disease is limited, as patients included were relatively young and had favourable baseline characteristics.
Conclusion
The findings from this review indicate that RCAB appears promising and may offer benefits to patients. However, in the absence of randomized controlled trials or well-conducted observational studies, they should be interpreted with caution.
Footnotes
Competing interests: None declared.
Funding: This work was supported by a financial contribution from the Government of Alberta. The views expressed herein do not necessarily represent the official policy of the Government of Alberta. The Health Technology & Policy Unit, School of Public Health, University of Alberta receives a multiyear unrestricted grant from Alberta Health to conduct health evidence reviews to inform policy decisions in the province.
Contributors: F. Hammal, F. Nagase, D. Menon and T. Stafinski conceived and designed the study. F. Hammal and F. Nagase acquired the data, which F. Hammal, F. Nagase and I. Ali analyzed. F. Hammal and F. Nagase wrote the manuscript with contributions from D. Menon and T. Stafinski. All authors critically revised the manuscript and gave final approval of the version of the article to be published.
- Accepted December 18, 2019.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.