


Article Figures & Tables
Figures
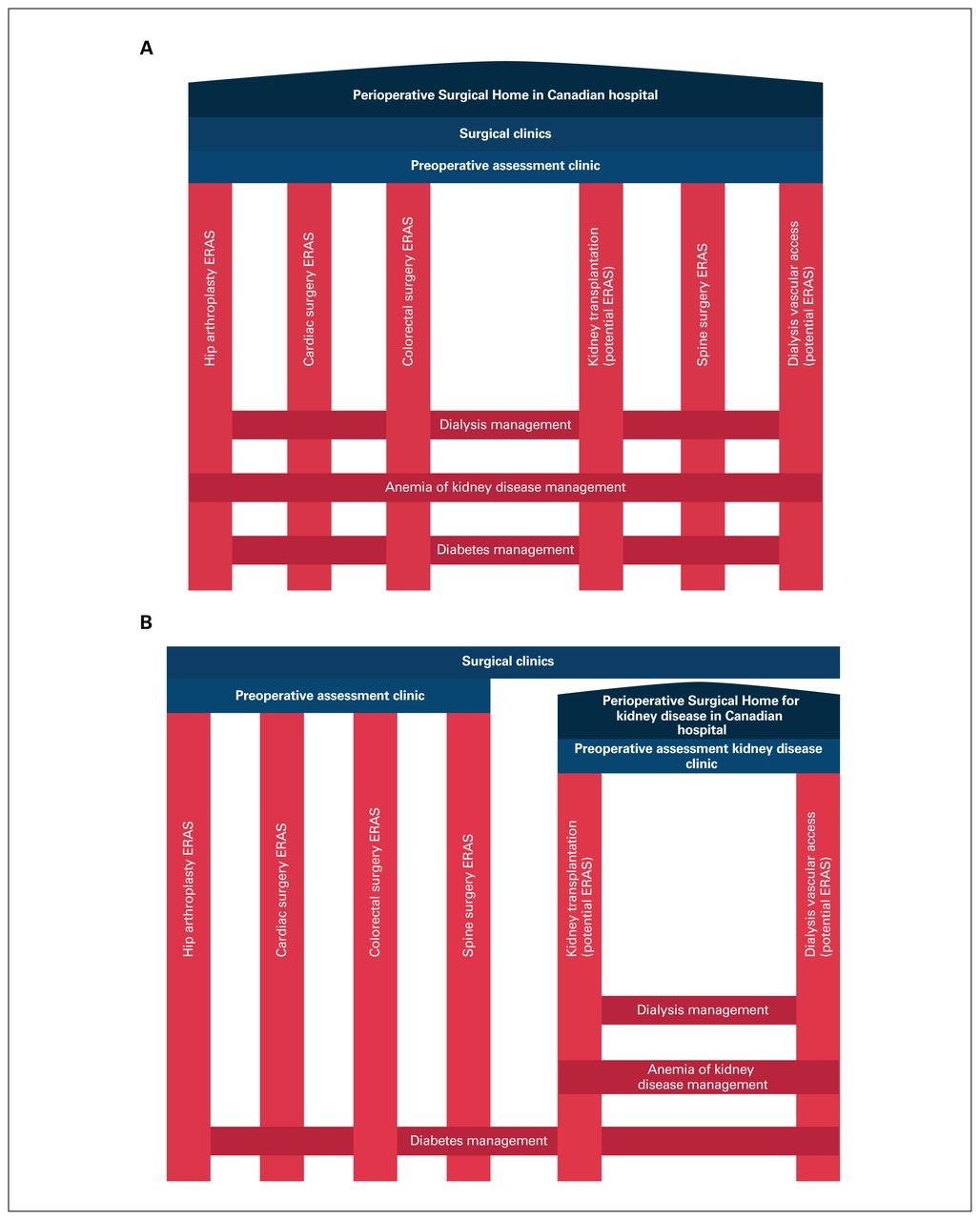
- Fig. 1
Conceptual model of intersecting vertical and horizontal surgical pathways within a Canadian hospital setting, with a Perioperative Surgical Home that encompasses all surgical populations and procedures (A), and only patients with kidney failure and pathways specific to kidney disease (B). ERAS = Enhanced Recovery After Surgery.

Tables
- Table 1
Summary of 2018 ERAS Society protocol elements and grade of recommendation for elective colorectal surgery (27)
Element Grade of recommendation Preadmission Information, education, counselling Strong Preoperative optimization (risk assessment, smoking and alcohol cessation) Strong Prehabilitation Weak Preoperative nutritional care (screening and nutrition itself) Strong Management of anemia (targets, interventions) Strong Preoperative Prevention of nausea and vomiting Strong Preanesthetic medication (anxiolysis and pain) Strong Antimicrobial prophylaxis and skin preparation Intravenous antibiotic treatment, chlorhexidine: strong
Oral antibiotic treatment, advanced skin decontamination: weakMechanical bowel preparation Strong Preoperative fluid and electrolyte therapy to maintain euvolemia Strong Preoperative fasting and carbohydrate loading up to 2 h before surgery Strong Intraoperative Standard Anesthetic Protocol Strong Intraoperative fluid and electrolyte therapy aimed at near-zero fluid balance; goal-directed fluid therapy in patients at high risk Strong Prevention of intraoperative hypothermia Strong Minimally invasive surgical approach (compared to open surgery) Strong Avoidance of routine use of pelvic and peritoneal drains Strong Postoperative Avoidance of nasogastric intubation; if placed, removal before reversal of anesthesia Strong Avoidance of opioids; use of NSAIDs; apply multimodal analgesia in combination with spinal/epidural or blocks when indicated Strong Thromboprophylaxis: mechanical prophylaxis until discharge; low-molecular-weight heparin until 28 d postoperatively Strong Fluid and electrolyte administration aimed at near-zero fluid balance, with avoidance of isotonic crystalloids if giving fluid Strong Bladder catheterization for 1–3 d acceptable; catheter should be removed routinely after this period Strong Prevention of postoperative ileus through multimodal strategy Strong Postoperative avoidance of hyperglycemia with insulin therapy and stress-reducing techniques Stress-reducing: strong
Insulin: strong in ICU, weak on wardOffering of food on day of surgery; offering of immunonutrition (anti-inflammatory supplements such as L-arginine) to malnourished patients Strong Early mobilization through education and patient encouragement Strong ICU = intensive care unit; NSAID = nonsteroidal anti-inflammatory drug.
Consideration Potential target for horizontal perioperative pathway Volume and hypotension avoidance Dialysis timing before and after surgery
Volume management on dialysis
Antihypertensive medication reconciliation in perioperative period
Avoidance of aggressive intravenous fluid administration; adaptation to residual kidney function and urine output
Electrolyte derangements Hyperkalemia
Hyponatremia
Hypocalcemia
Metabolic acidosis
Differences in management based on type of dialysis modality
Anemia Complex iron-repletion strategies at baseline
Patient likely taking erythropoietin-stimulating agents, with unique adverse effects
Lower hemoglobin targets than in the general population
For kidney transplantation candidates, blood transfusions present risk of immune sensitization (greater caution should be taken before blood transfusions)
Bleeding Increased risk of perioperative bleeding
Different pathophysiology of bleeding, necessitating directed management of bleed risk
Altered metabolism of anticoagulants
Miscellaneous Altered metabolism of opioid medications
Lack of validated risk-stratification tools
Higher risk of postoperative cardiac complications with atypical symptoms, with events more challenging to diagnose
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.