


Article Figures & Tables
Figures
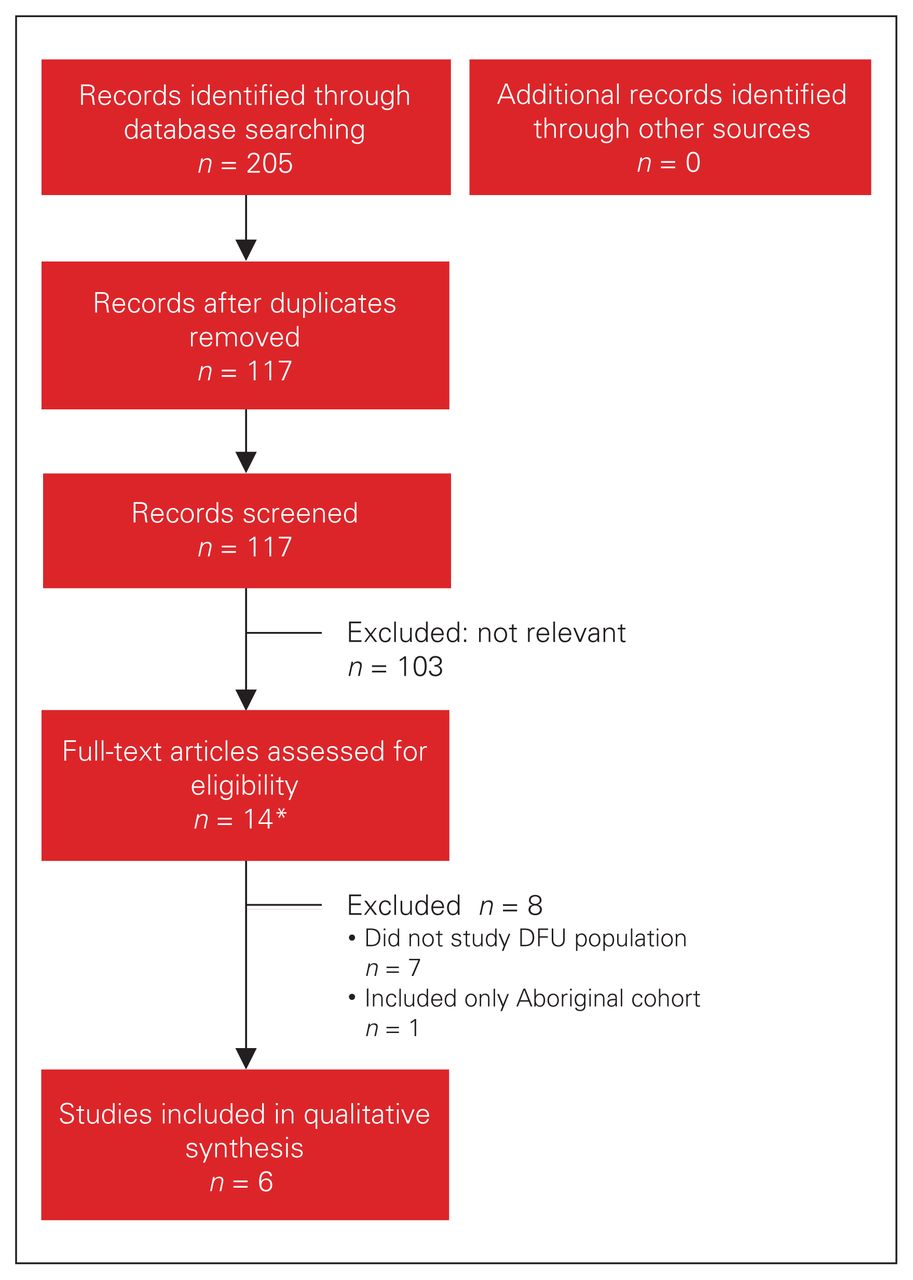
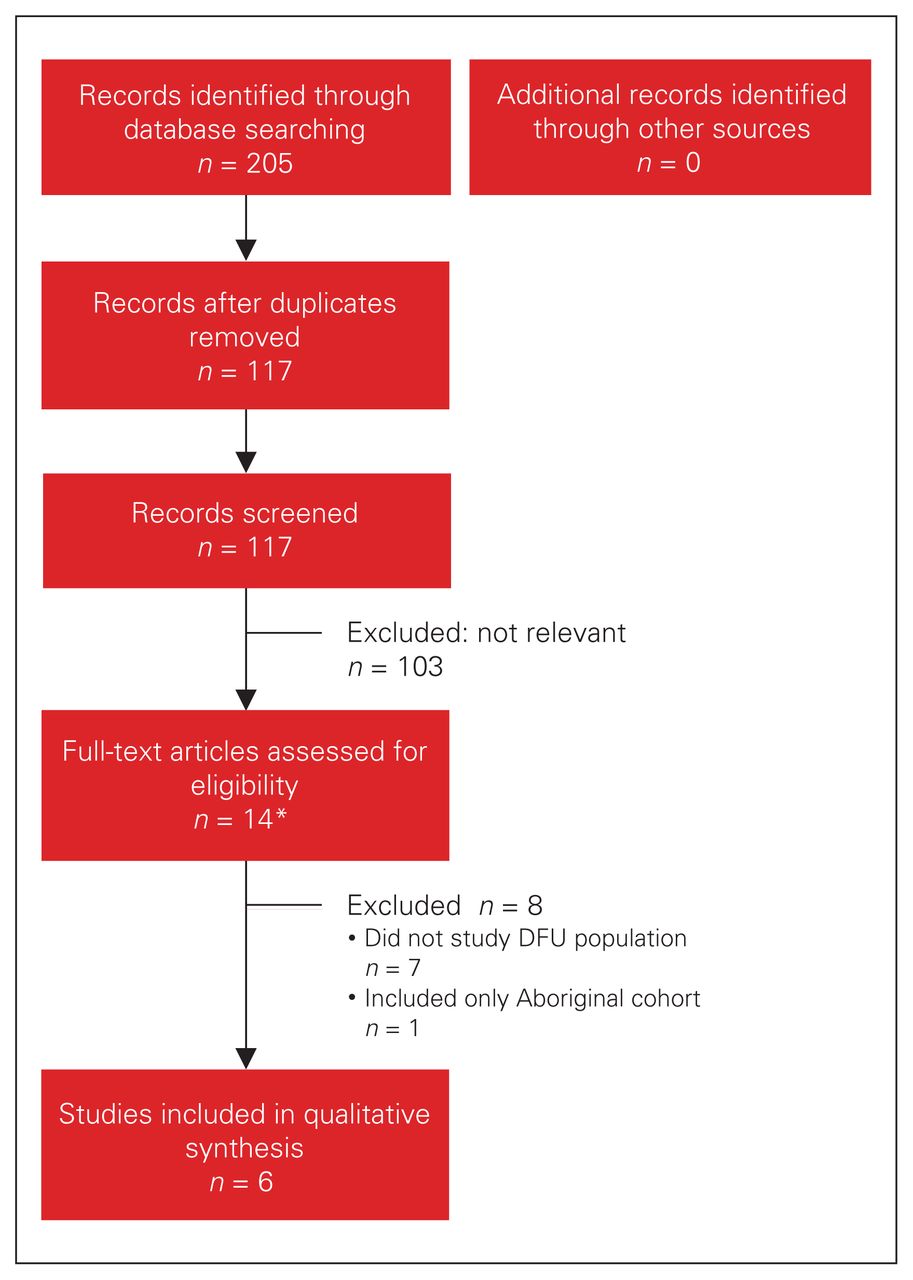
- Fig. 1
Flow diagram showing study selection. *One article had only an abstract, as the final manuscript was still being drafted. (13) DFU = diabetic foot ulcer.
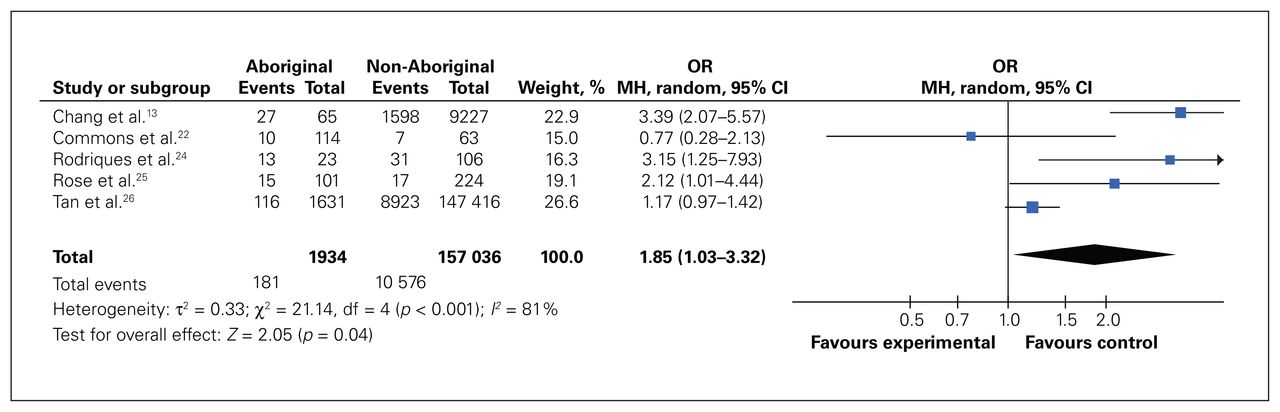
- Fig. 2
Effect of Aboriginality on major lower-extremity amputation. CI = confidence interval; df = degrees of freedom; MH = Mantel–Haenszel; OR = odds ratio.
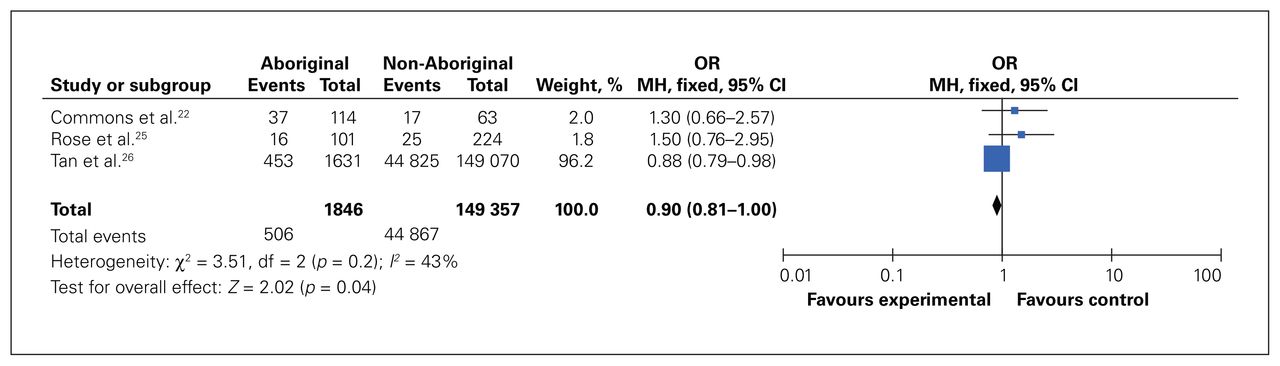
- Fig. 3
Effect of Aboriginality on minor lower-extremity amputation. CI = confidence interval; df = degrees of freedom; MH = Mantel–Haenszel; OR = odds ratio.

Tables
Study Country Length of follow-up, yr No. of Aboriginal patients/no. of non-Aboriginal patients M/F gender, % Baseline population age, mean ± SD,* yr Findings Chang et al., (13) 2018 US 4 651/92 279 45.7/54.3 71.9 ± 11.9 Incidence of major amputation within 1 yr after diagnosis of DFU was higher for Native American patients than White patients (4.1% v. 1.0%, p < 0.001)
In multivariable analysis, being Native American was associated with increased risk of major amputation compared to being White (HR 2.42, 95% CI 1.62–3.62)
Commons et al., (22) 2015 Australia 1 114/63 59.9/40.1 54.4 (95% CI 28.8–80.1) Indigenous patients were younger than non-Indigenous patients (50.5 [95% CI 28.3–72.6] yr v. 61.6 [95% CI 36.1–87.1] yr) and had higher incidence of major amputation (RR 4.1 [95% CI 1.6–10.7]) and minor amputation (RR 6.2 [95% CI 3.5–11.1])
Jia et al., (23) 2017 Australia 1 66/441 68/32 62.9 ± 12.8 Independent risk factors for infection: ulcers healed between 3 and 12 mo (OR 2.3 [95% CI 1.6–3.3]), deep ulcers (OR 2.2 [95% CI 1.2–3.9]), peripheral neuropathy (OR 1.8 [95% CI 1.1–2.9]), previous foot ulcers (OR 1.7 [95% CI 1.2–2.4]), foot deformity (OR 1.4 [95% CI 1.0–2.0]), female gender (OR 1.5 [95% CI 1.1–2.1]) and age (OR 0.98 [95% CI 0.97–0.99])
No association found between infection and Indigenous background
Rodrigues et al., (24) 2016 Australia 3 23/106 62.8/37.2 63.43 ± 14.07 (CI 60.98–65.89) Indigenous group had higher amputation rate than non-Indigenous group (56.5% v. 29.2%)
Mean age at amputation was similar in Indigenous (62 [SD 12.5] yr [95% CI 55.09–70.14 yr]) and non-Indigenous (62.0 [SD 11.5] yr [95% CI 57.81–66.25 yr]) groups
Rose et al., (25) 2008 Canada 1 101/224 63/37 59 ± 14 (Aboriginal 55 ± 13, non-Aboriginal 61 ± 14) Aboriginal patients had higher rate of any amputation than non-Aboriginal patients (24% v. 15%), but frequency of major amputation (defined in this study as amputation proximal to toes) was not influenced by ethnicity
Aboriginal patients had shorter average time from initial clinic visit to major lower-extremity amputation than non-Aboriginal patients (50 [SD 64] wk v. 62 [SD 56] wk, p < 0.01)
Living in rural or reserve community was correlated with shorter average time from initial clinic visit to major lower-extremity amputation than living in urban community (45 [SD 56] wk v. 66 [SD 61] wk, p < 0.002)
Aboriginal ethnicity was not associated with poorer clinical outcome when nonurban residence was controlled for
Earlier major lower-extremity amputation was significantly associated with nonurban residence, Aboriginal ethnicity and arterial insufficiency on univariate analysis; however, when nonurban residence was controlled for, Aboriginal ethnicity was not associated with earlier amputation
Tan et al., (26) 2019 US 12 1654/149 070 66.6/33.4 59.2 ± 13.7 (Aboriginal 54.4 ± 13.3, White 60.7 ± 13.4) Native American patients had increasing trend of major amputation over study period
Native American patients had significantly higher major amputation rates than White patients (5.4% v. 7.1%, p < 0.001) and higher risk of major amputation (OR 1.47 [95% CI 1.2–1.8])
Native American patients had lowest rates of open bypass (0.9%) and endovascular revascularization (5.0%) of all ethnic groups studied (p < 0.001)
CI = confidence interval; DFU = diabetic foot ulcer; F = female; HR = hazard ratio; M = male; OR = odds ratio; RR = relative risk; SD = standard deviation.
↵* Except where noted otherwise.
Study Overall bias: risk of bias judgment Overall predicted direction of bias for this outcome Chang et al. (13) Serious Unpredictable Commons et al. (22) Serious Unpredictable Jia et al. (23) Moderate Unpredictable Rodrigues et al. (24) Moderate Unpredictable Rose et al. (25) Moderate Unpredictable Tan et al. (26) Moderate Unpredictable
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.