


Abstract
Background: Several commonly used procedures for knee osteoarthritis (OA) are not supported by evidence-based guidelines. The objective of this study was to identify the proportion of patients who underwent knee arthroscopy or magnetic resonance imaging (MRI) and the timing of these procedures before total knee arthroplasty (TKA).
Methods: We conducted a retrospective cohort study using administrative data sets from Ontario, Canada. We identified the proportion of patients who underwent knee arthroscopy in the previous 10 years or an MRI in the 3 years before their primary TKA. We also evaluated the rate of arthroscopies by diagnosis. We report the timing of each outcome in relation to the TKA, rates by geographical area, and differences in rates over time.
Results: We included 142 275 patients, of whom 36 379 (25.57%) underwent knee arthroscopy (median time 2.8 [interquartile range (IQR) 1.1–6.0] years); 22% of those were within 1 year of TKA and 52% were within 3 years. The rates of arthroscopies for a diagnosis of osteoarthritis (OA) steadily decreased, while those for meniscal-related diagnoses increased over the study period (p < 0.0001). There was significant variation by region. Of the cohort, 23.2% (n = 32 989) had an MRI before their TKA, with rates significantly increasing over time (p < 0.0001).
Conclusion: A substantial proportion of patients with knee OA received diagnostic and therapeutic interventions before TKA that are contrary to clinical practice guidelines.
Osteoarthritis (OA) of the knee is one of the most common chronic health conditions and is a leading contributor to health care service use.1–3 The disease typically involves slow degeneration of knee joint tissues and progressive symptoms, ultimately resulting in deterioration of the joint.4 Surgical replacement of the joint through total knee arthroplasty (TKA) improves symptoms for most patients with end-stage knee OA. Before end-stage disease, patients undergo numerous assessments and interventions aimed at improving symptoms and delaying disease progression.
Several commonly used treatments for knee OA are not supported by evidence-based guidelines. Notably, knee arthroscopy is often performed to treat degenerative meniscal pathology, a common feature of OA, yet substantial high-quality evidence showing a lack of clinical improvement and cost-effectiveness5–12 has led to recommendations against the use of arthroscopy in patients with degenerative knee disease.13–18
Physical examination, history and weight-bearing radiographs are recommended to diagnose knee OA and guide treatment choices.19,20 Importantly, MRI is not recommended for the diagnosis or management of OA, yet patients are often referred for an MRI that is considered unnecessary by orthopedic specialists.21 Previous retrospective studies have shown that few patients with knee pain have a weight-bearing radiograph before receiving an MRI.21 Moreover, MRIs often detect incidental findings, such as degenerative meniscal tears that are common among middle-aged individuals with or without knee symptoms, likely do not contribute to pain and should not change management.22–25
Clinical practice guidelines provide recommendations on appropriate interventions for the diagnosis and treatment of knee OA13–18 based on the best available research evidence and reviewed by panels of international experts. However, the extent to which such guidelines are followed is unclear. Many of the non-recommended treatments for knee OA appear to remain in common use and may occur within close proximity to total joint replacement, perhaps contributing to unnecessary health care expenditures on top of those required for the TKA.
The objective of this study was to identify the proportion of patients with knee OA who underwent knee arthroscopy or MRI and the timing of these procedures before TKA.
Methods
We conducted a retrospective cohort study using administrative data sets accessed through ICES (formerly the Institute for Clinical Evaluative Sciences). We included all Ontario residents who underwent an elective, primary TKA for osteoarthritis between April 1, 2007, and March 31, 2017. The Ontario Health Insurance Plan (OHIP) provides universal health coverage for medical services to all Ontario residents. We used OHIP physician billing records to identify the initial cohort. We excluded patients younger than 40 years, as well as those who had undergone a TKA within the previous 15 years. We also excluded patients if we were unable to identify a hospital admission record for the procedure or if the hospital record for TKA did not include a diagnosis of OA.
We collected baseline variables including age, sex, location of residence, income quintile and Charlson Comorbidity Index, using a 3-year look-back period before the primary TKA. Location of residence was assigned according to the 14 health administrative boundaries, Local Health Integration Networks (LHINs), that are used to administer health care throughout the province. We also recorded medical comorbidities including coronary heart failure,26 chronic obstructive pulmonary disease,27 hypertension,28 diabetes,29 rheumatoid arthritis,30 depression and obesity. Depression was defined as any psychiatric visit or hospital admission for depression or 2 visits to a general practitioner for depression within a 2-year period. Obesity was defined as any physician visit for obesity or hospital admission with a corresponding diagnosis code for obesity in the 3 years before the TKA.
Data sources
The administrative data sources used for this study include the Canadian Institute for Health Information Discharge Abstract Database/Same Day Surgery (CIHIDAD/SDS), which includes all hospital-based admissions for diagnostic and surgical procedures; OHIP, which contains all physician fee-for-service billing requests for patient encounters and procedures; and the Registered Persons Database (RPDB), for demographic information including age, gender, income and geographic location. Data sets were linked using unique, encoded identifiers. A full list of the codes used is provided in a supplemental table (Appendix 1, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.002221/tab-related-content).
Patient-level data were linked across databases with unique encoded identifiers. The use of these data was authorized under Ontario’s Personal Health Information Protection Act, which does not require review by a research ethics board, and thus patient consent was not required. Our reporting follows the guidelines of the Reporting of Studies Conducted Using Observational Routinely Collected Data (RECORD) statement (Appendix 2, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.002221/tab-related-content).31
Procedures
Arthroscopy
We first identified the rates and timing of knee arthroscopy within 10 years before the primary TKA, identified by either a hospital or physician billing record for the procedure. For patients with a hospital-based procedure, we were also able to capture diagnoses associated with the admission. The patient diagnosis recorded as most responsible for the admission was categorized into 4 mutually exclusive categories: 1) osteoarthritis/gonarthrosis; 2) meniscal-related, 3) pain in joint, and 4) other (not belonging to any of the first 3 diagnoses). If patients had more than 1 diagnosis recorded with the procedure, we placed them in the first category of our defined hierarchy.
MRI
We identified patients who had received an MRI in the 3 years before their TKA. We identified MRI using OHIP physician billing codes. Currently, there is not a specific OHIP code for an MRI of the knee joint; therefore, we identified any incidence of the OHIP fee code for an MRI of an extremity or joint.
Statistical analysis
We used descriptive statistics to describe the number of arthroscopies and MRIs per year over the study period as well as the timing of each outcome in relation to the TKA. For knee arthroscopy, we also evaluated the rate of the procedure by corresponding diagnosis code for each year over the study period. We also reported the proportion of patients in the cohort who underwent each outcome by geographical area (LHIN). We used the Cochran–Armitage χ2 test to assess differences in rates over time.
Results
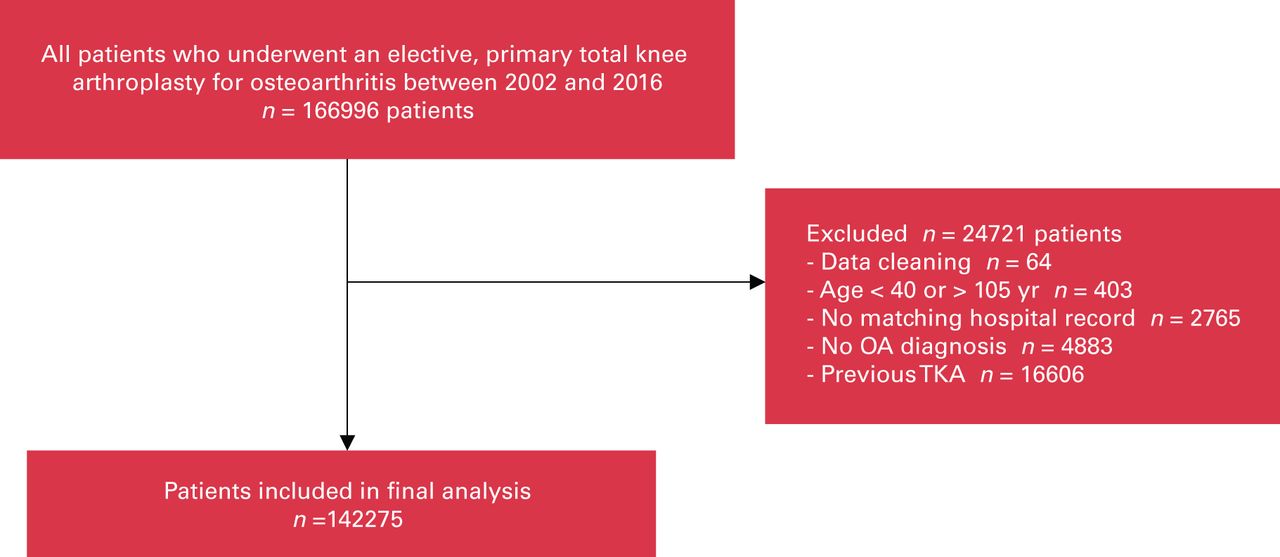
During the study accrual period, 166 996 patients met the coding criteria for study inclusion, of which 24 721 (14.8%) patients were excluded. The resulting study cohort contained 142 275 patients (Figure 1). The average age of the cohort was 67.64 ± 9.31 years, and 62.2% of patients were female (Table 1). In general, the comorbidities did not vary between groups that had different interventions before the TKA.
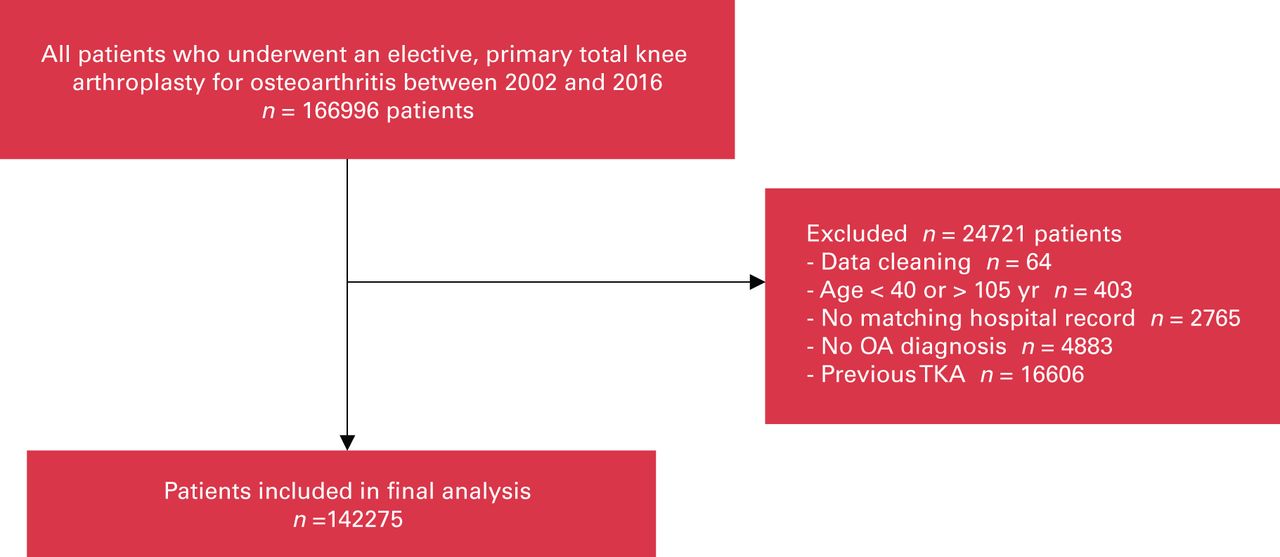
Cohort development flow chart. OA = osteoarthritis; TKA = total knee arthroplasty.
Baseline characteristics of cohort*
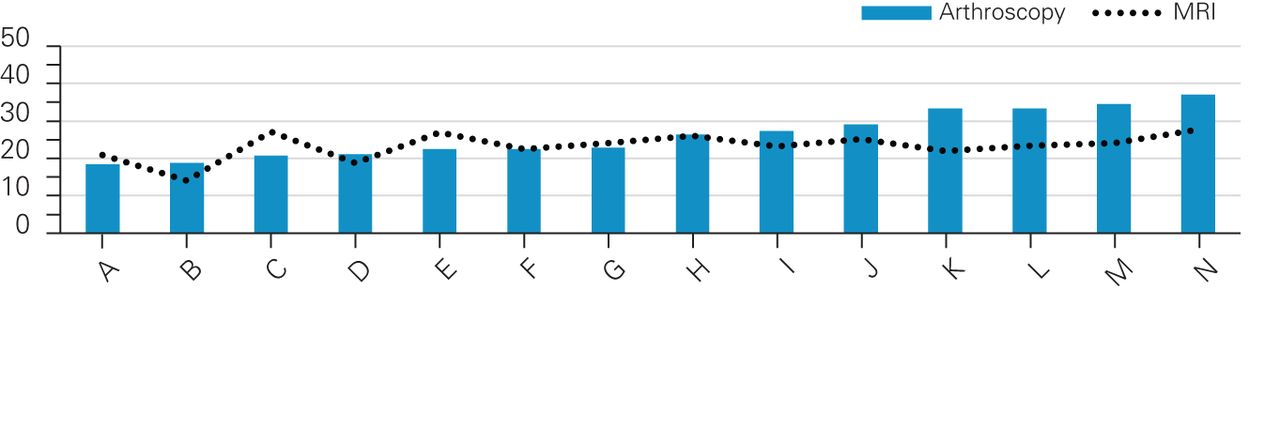
A total of 36 379 (25.57%) patients in the cohort had undergone an arthroscopic knee procedure over the study period, with 8147 of the total TKA cohort (5.7%) undergoing the procedure in the 1 year prior, and 18 777 (13.2%) in the 3 years before their primary TKA. The percentage of patients who underwent a previous arthroscopy gradually decreased over the study period, from 28.8% in 2007 to 21.9% in 2016 (p < 0.0001; Figure 2). The proportion of knee arthroscopies performed for a corresponding diagnosis code of OA steadily decreased each year, while the proportion of knee arthroscopies performed for a corresponding diagnosis code of meniscal-related diagnoses increased over the same period (p < 0.0001) (Figure 3). Median time from arthroscopy to TKA was 2.8 (IQR 1.1–6.0) years, with 22.4% (8147/36 379) of the arthroscopies occurring within 1 year and 51.6% (n = 18 777) occurring within 3 years. Further, there was significant variation in the rates of knee arthroscopies by region (p < 0.001) (Figure 4).
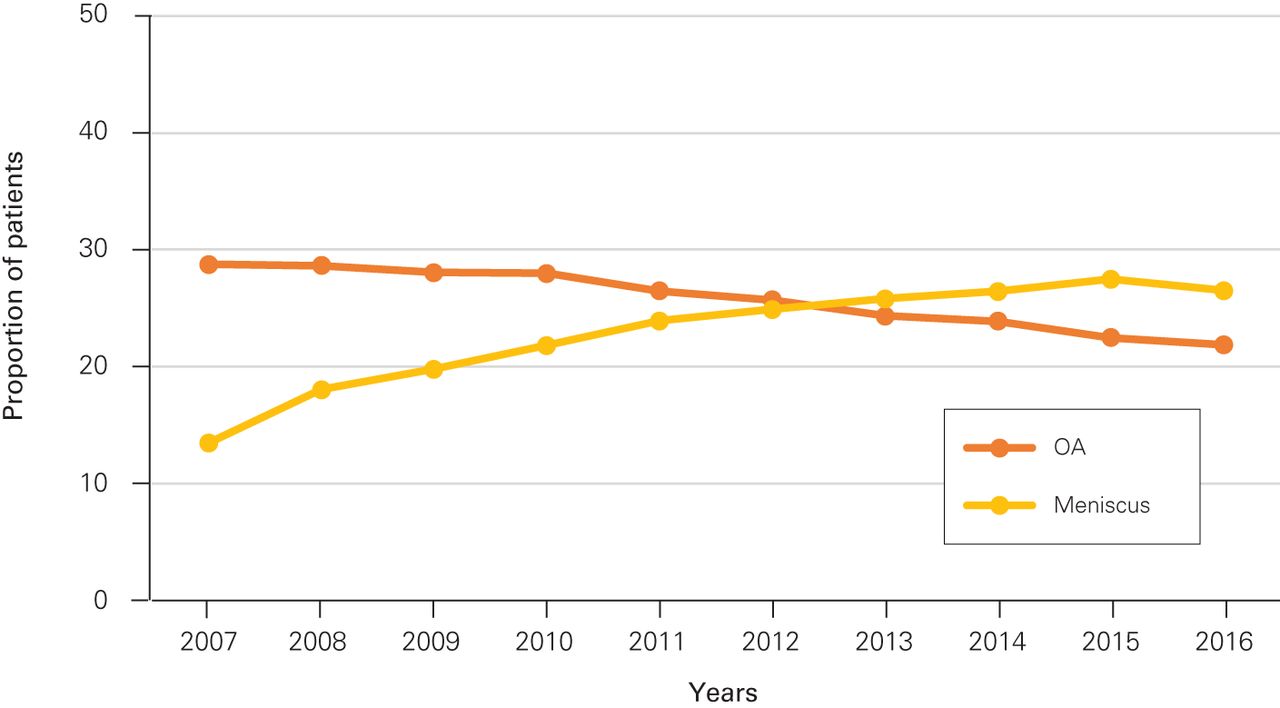
Proportion of patients who underwent each outcome by fiscal year. MRI = magnetic resonance imaging; OA = osteoarthritis.

Rate of arthroscopy by diagnosis and fiscal year. OA = osteoarthritis.

Proportion of patients who underwent each outcome by geographical area over the 10-year period. MRI = magnetic resonance imaging.
Overall, 23.2% (n = 32 989) of the patients had an MRI in the 3 years before their TKA. The percentage of patients who underwent an MRI before TKA significantly increased each year, from 13.5% in 2007 to 26.5% in 2016 (p < 0.0001) (Figure 2). There was a temporal link between MRI and TKA, with 50% of MRIs occurring in the year preceding the TKA.
Discussion
The prevalence of knee OA is rapidly growing, resulting in increased demands for care and substantial patient and economic burden. Therefore, it is crucial to provide value-based interventions. This study identifies that before TKA, a substantial proportion of patients with knee OA received diagnostic and therapeutic interventions that are not supported by strong evidence and clinical practice guidelines.
Hawker and colleagues32 conducted a similar study assessing knee arthroscopy usage in relation to TKA among patients in Ontario. They reported that 5.7% of patients had an arthroscopy to treat OA in 2002. A similar study evaluated the prevalence of primary TKA after arthroscopic knee débridement among patients aged 50 years or older between 1992 and 1996. They reported that 9.2% received TKA within a year and 18.4% within 3 years of their arthroscopy.33
Consistent with our results, a previous analysis of historical utilization trends of knee arthroscopy in Ontario between 2003 and 2012 identified an increase in the proportion of arthroscopy procedures for degeneration or derangement of meniscus and a dramatic decrease in the proportion for osteoarthritis.34 Although these shifts in practice may reflect an appropriate decline in provision of arthroscopy for OA, it may also suggest a change in diagnostic coding, as degeneration of the meniscus is a feature of OA. In other words, the same types of patients continue to undergo knee arthroscopy, and rates are actually increasing.
Degen and colleagues35 reported a significant increase in the use of knee arthroscopy in the United States between 2006 and 2016. Notably, there was also a significant increase in age among patients undergoing meniscectomy, suggesting the procedure continues to be used to treat degenerative meniscal tears that are associated with OA. Dhawan and colleagues36 found that 16% of TKA patients had undergone arthroscopic débridement within 1 year of TKA. A similar evaluation in England37 reports that 9.9% of patients aged 60 years or older who underwent arthroscopic partial meniscectomy received a subsequent TKA within 1 year, and 16.6% within 2 years.
Our study also identified an increasing proportion of MRIs conducted on patients with a diagnosis of OA before TKA. Although we cannot confirm whether the MRI was performed on the index knee, 50% of the MRIs occurred in the year preceding the TKA, suggesting it was likely related to the evaluation of the patient for OA or TKA. Magnetic resonance imaging is not routinely required before TKA; thus, performing these unnecessary MRIs incurs further waiting times, can cause unneeded anxiety while waiting for specialist consultation and can delay imaging for patients presenting with pathology more appropriate for MRI examination. Additionally, the information gleaned from these inappropriate imaging studies does not alter management and incurs significant expenses to publicly funded systems or third-party insurers.
Deveza and colleagues38 evaluated whether the frequent use of MRIs in older adults with knee symptoms may be contributing to continued high rates of knee arthroscopies. They found that 25.1% of patients aged 50 years and older who had a knee MRI underwent arthroscopy in the following 12 months compared with only 3.0% of patients who received a radiograph. Thus, reducing the unwarranted use of MRI in this population may also help to decrease the overuse of arthroscopy that is likely performed to treat identified degenerative meniscal pathology.
Cohen and colleagues39 evaluated preoperative interventions before TKA, reporting an average cost of US$3500 per patient. Importantly, a high proportion of these costs were interventions that were not supported by clinical evidence and occurred in close proximity to TKA, with about 5%–7% of patients receiving a knee arthroscopy within 1 year of TKA. Further, evidence suggests an increased risk of adverse events, including infection or revision arthroplasty, when arthroscopy is performed within 2 years of TKA.40,41
To our knowledge, this is the first study to report the incidence and timing of commonly used yet controversial procedures among a large cohort of patients with knee OA before TKA in a Canadian health care system.
Limitations
As the present results are based on administrative databases, a limitation includes the potential for inaccurate documentation and coding. Further, given the diagnostic and billing codes available during the study period, we could not specify which joint received the MRI. With the close proximity of the MRI to the TKA and the age of our patient cohort, it is plausible to assume a large proportion was done on the index knee. However, additional studies using prospective primary data collection from patients rather than administrative data are required to determine a more precise estimate of the rates of MRI before TKA.
Conclusion
The results show that a substantial proportion of patients received diagnostic and therapeutic interventions within close proximity to TKA that lack the support of strong evidence. These results highlight the need for greater knowledge translation and exchange between expert panels, health care providers, patients and payers.
Acknowledgements
This study was supported by the ICES Western site. ICES is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). Core funding for ICES Western is provided by the Academic Medical Organization of Southwestern Ontario (AMOSO), the Schulich School of Medicine and Dentistry (SSMD), Western University, and the Lawson Health Research Institute (LHRI). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES, AMOSO, SSMD, LHRI, or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed in the material are those of the author(s), and not necessarily those of CIHI.
Footnotes
Competing interests: Trevor Birmingham reports receiving grants (paid to institution) from the Canadian Institutes of Health Research, outside the submitted work. Alan Getgood reports receiving consulting fees and research support from Smith and Nephew Inc. and research support form Ossur Inc. Dr. Getgood is on the advisory board of and has stock options with Precision OS and Spring Loaded Technologies. No other competing interests were declared.
Contributors: Ryan Degen, Alan Getgood, J. Robert Giffin, Jacquelyn Marsh, J. Andrew McClure, Blayne Welk and Kevin Willits contributed to the conception and design of the work. Robert Litchfield and Jacquelyn Marsh contributed to the acquisition of data. Trevor Birmingham, Jacquelyn Marsh and J Andrew McClure contributed to the analysis and interpretation of data. Jacquelyn Marsh and Blayne Welk drafted the manuscript. Ryan Degen, Trevor Birmingham, Alan Getgood, J. Robert Giffin, J. Andrew McClure, Robert Litchfield, Blayne Welk and Kevin Willits revised the manuscript critically for important intellectual content. All of the authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
- Accepted March 3, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.