


Abstract
Background: Recreational cannabis use was legalized in Canada in 2018. Cannabis use patterns and patient attitudes toward cannabis use, particularly in the context of these legal changes, are not well understood. Our aim was to evaluate baseline cannabis use patterns and attitudes at the time of legalization among patients with upper extremity conditions in Canada.
Methods: In 2018, we conducted a multicentre cross-sectional survey study of 1561 patients with upper extremity conditions at 7 surgical centres. Participants were asked whether they currently use cannabis. If yes, they were asked questions regarding usage patterns and perceptions of cannabis use, including likelihood of use, safety and comfort discussing it with their physician.
Results: In the 6 months after legalization, 790 (51%) participants felt that cannabis was safer than prescription narcotics, with 450 (29%) currently using cannabis. Reasons for cannabis use included pain (56%), stress (51%) and recreation (42%). Of the 1105 patients not using cannabis, 267 (24%) were more likely to consider it after legalization. Of the 450 cannabis users, 73 (16%) had been using it for less than 6 months, 206 (46%) stated they were more comfortable discussing cannabis with their physician after legalization and 195 (43%) were using cannabis more than 4 times per week.
Conclusion: Many patients with upper extremity conditions were regularly using cannabis. Patients were more comfortable discussing cannabis with their physician than before legalization. Treating surgeons should be aware of these trends and expect to receive questions regarding cannabis use.
Societal attitudes toward the use of cannabis for both medical and recreational reasons have undergone a recent shift. In Canada, cannabis has been legalized for medical use since 20011 and was legalized for recreational use in October 2018, with edibles legalized in October 2019.2 Baseline use patterns and perceptions about cannabis use before legalization are largely unknown and are problematic to study as patients often do not feel comfortable disclosing information on illegal substances. Understanding these patterns and attitudes around the time of legalization provides an opportunity to evaluate how these legal changes may influence future use.
Given the recent nature of these legal changes, many physicians have not received formal education in the effects of cannabis, both positive and negative, on their patients.3 Particularly, surgical outcomes may be influenced by cannabis use, systemically (with respect to anesthesia), intraoperatively (with respect to tissue or bone quality and propensity for healing) and post-operatively (with respect to analgesia).4 If the legalization of cannabis results in a large proportion of patients using cannabis at the time of surgery, treating surgeons must be educated in the risks and benefits associated with cannabis use.
The purpose of the present study was to assess the use of cannabis and patients’ reasons for use, patterns of use, and attitudes toward use around the time of legalization of recreational cannabis in Canada. We chose to study these topics in patients with upper extremity conditions presenting to surgical centres for either chronic or acute assessments. We hypothesized that many of these patients would already be using cannabis for various reasons.
Methods
This was a multicentre, cross-sectional survey study. In total, 7 centres participated, including 6 Canadian centres and 1 in the United States (Chicago), meant to act as a comparison. Data collection began in the fall of 2018, immediately after the legalization of recreational cannabis in Canada. Recreational use of cannabis was not legalized at the time of data collection in Chicago, but has since been legalized. Data were collected for a 6-month period.
Study population
The study population consisted of emergent and elective patients with upper extremity conditions seen in the outpatient setting by orthopedic surgeons specializing in the hand, wrist and elbow. We included newly referred and existing patients with chronic upper extremity conditions, such as arthritis or tendinopathies, as well as those with acute injuries, such as fractures, dislocations or soft tissue strains. We excluded patients unable to complete a paper-based survey in English owing to a language or cognitive barrier and patients younger than 19 years, as this is the legal age for cannabis consumption in most provinces (with the exception of Alberta and Quebec, where it is 18 years of age).
Data collection
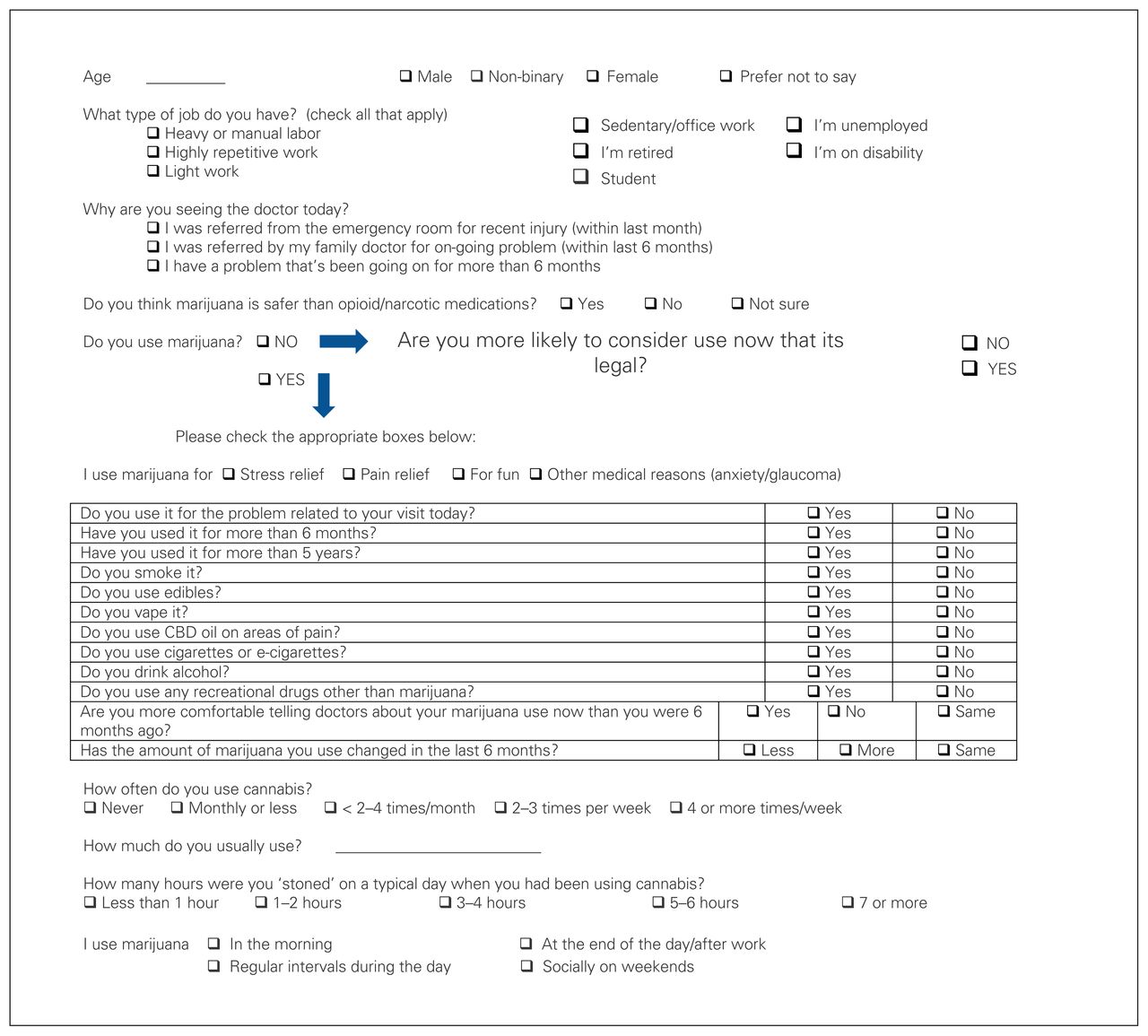
All patients meeting the aforementioned inclusion and exclusion criteria and presenting for an appointment at a participating upper extremity clinic were approached to participate. In keeping with our ethics approval and to ensure participants felt comfortable providing their true responses, participation was voluntary, and an anonymous survey approach was used. A team member not directly involved in their care approached patients for participation. Patients were provided with a letter of information outlining the topic and purpose of the survey before agreeing to participate. Those who verbally agreed to participate completed a paper-based survey in the waiting room (Figure 1). Once surveys were complete, they were placed in an enclosed, opaque collection box before their visit with their surgeon to minimize social desirability bias. We did not collect refusal rates, and participants provided no identifying information.

Cannabis use survey. Note: CBD = cannabidiol.
Since there is no validated survey that assesses baseline cannabis use patterns and attitudes, the senior editors developed the survey used in this study, but it has not been validated. Demographic information included parameters commonly collected in research studies of upper extremity conditions, as well as whether or not participants were currently using cannabis. If participants answered affirmatively to this question, they were then asked to complete further questions regarding the method, frequency, duration and reason for usage. Frequency of use and intensity of use questions were quantified based on the Cannabis Use Disorders Identification Test-Revised (CUDIT-R), which is a validated questionnaire meant to screen for cannabis misuse disorders.5 If participants answered that they were not using cannabis, they were asked whether they were more likely to consider its use now that it has been legalized.
Upon completion, a member of the research team then obtained individual surveys from the collection boxes.
Statistical analysis
Data were collected in a secure Redcap file that was maintained by the lead study site. We conducted descriptive statistics.
Ethics approval
All participating centres obtained ethical approval for the study.
Results
In total, 1561 participants responded to the survey. Baseline characteristics of survey responders are summarized in Table 1. The average age of responders was 49 (standard deviation 16) years (range 19–91 yr), with a near equal split of males and females and a smaller number who chose not to state their gender. Occupations varied, with a substantial number of participants not currently working (retired, unemployed or on disability). As the answers to the question regarding occupation were not mutually exclusive, participants could select as many as applied; there were 1916 responses to this question, and the sum of the percentages for occupation was greater than 100. The most common reason participants presented to the clinic was for an ongoing problem that had existed for more than 6 months; 92 (5.9%) participants chose not to answer this question. About half of the participants (n = 790, 50.6%) felt that cannabis was safer than prescription narcotics, with 561 (36.0%) stating they were unsure and 184 (11.8%) stating they felt it was not safer; 26 (1.7%) participants chose not to answer. Overall, 450 (28.8%) participants responded that they currently use cannabis. This was significantly correlated with male gender and younger age (p < 0.05). Of the 1105 (70.8%) participants who did not use cannabis, 267 (24.2%) were more likely to consider using it since legalization, 771 (69.8%) were no more likely to consider using cannabis and 67 (6.1%) participants chose not to answer.
Baseline characteristics
Of the 450 participants who used cannabis, 191 (42.4%) were using cannabis for the problem relating to their current medical visit. General reasons for use were pain (n = 253, 56.2%), stress (n = 231, 51.3%), recreation (n = 189, 42.0%) and other medical conditions (n = 92, 20.2%). Answers to this question were not mutually exclusive and some respondents reported using cannabis for more than 1 reason. Concomitant substance use was common, including alcohol (n = 320, 71.1%), nicotine (n = 143, 31.8%), and other recreational drugs (n = 55, 12.2%). The most common method of cannabis use was smoking (n = 29, 73.1%), with edibles (n = 241, 53.6), vaping (n = 144, 32.0%) and cannabidiol oil (n = 168, 37.3%) used less commonly. Many respondents reported using cannabis by more than 1 method. Seventy-three (16.2%) patients had been using cannabis for less than 6 months, and 262 (58.2%) reported using cannabis for more than 5 years. When asked if they were now more comfortable discussing their cannabis use with their physician after legalization, 206 (45.8%) answered yes and 207 (46.0%) answered that their comfort had not changed, with only 28 (6.2%) answering that they were not more comfortable.
Cannabis use patterns are summarized in Table 2. Most patients who used cannabis reported that they used the same amount of cannabis over the previous 6 months (n = 309, 68.7%), with 46 (10.2%) reporting increased use and 77 (17.1%) reporting decreased use over the same time period. Cannabis was used most commonly at the end of the day, as reported by 211 (46.9%) patients, though 40 (8.9%) reported using cannabis in the morning, 134 (29.8%) reported using it on weekends or socially and 76 (16.9%) reported using it at regular intervals throughout the day. Some patients reported multiple answers, as these options were not mutually exclusive. Frequency of use varied widely, but with a fairly even distribution. The most common answer was using cannabis 4 or more times per week. When asked for how many hours the patient felt “stoned” on a typical day of cannabis use, responses varied (Table 2). A small number of participants (n = 34, 7.6%) reported feeling stoned for more than 5 hours per day. In an open-ended question, we asked participants to quantify the amounts used. Answers varied widely and are difficult to compare or quantify, given the different dose measurements, but included responses such as “1 joint per day, shared,” “25 mg of oil,” “four ounces per week,” “2 drops of oil,” “0.5 mL of THC,” “not very much,” “enough to take the edge off my pain,” “on an hourly basis,” “1 g,” “6 puffs,” and “1 cookie.” The main findings of the survey are illustrated in Figure 2.
Cannabis use patterns among users

Summary of the main survey findings.
To explore possible differences in cannabis used based on legalization policy, we separately analyzed data from the Chicago participants. In total, 109 surveys were collected from this centre. The average age was similar (46 yr); however, a greater proportion of this cohort was female (n = 61, 56.0%). Type of occupation was also similar (27.5% heavy or manual labour, 23.9% repetitive work, 11.9% light work, 17.4% office or sedentary work, 16.5% retired, 12.8% unemployed, 7.3% on disability, 8.2% students), with the exception of a greater proportion of unemployed patients. Fewer participants (n = 33) felt that cannabis was safer than prescription narcotics (30% v. 50% in the Canadian study population), with most patients reporting that they were unsure whether it was safer (n = 58, 53.2%). A slightly smaller proportion of patients (23%) in the Chicago cohort were currently using cannabis. The smaller size of this cohort meant that only 25 participants were currently using cannabis. We felt this number was too small to draw meaningful comparisons to the overall study group, so we did no further analysis of this cohort.
Discussion
This study reports a point-in-time assessment of cannabis use in patients with upper extremity conditions presenting to surgical care centres around the time of cannabis legalization in Canada. Before legalization, the proportion of orthopedic patients using cannabis was largely unknown; however, use in the general population was reported to be 14%.6,7 Legalization has led to an increased acceptance of cannabis use within the general population,8 with use rates reported to be 18% in 2018.6 Our study found that, around the time of legalization in Canada, 29% of patients with upper extremity conditions were using cannabis, which is higher than rates reported for the general population. Although reasons for this discrepancy are unknown, this increased pattern of use in orthopedic patients may be related to motivations for use, with pain and stress reported most commonly by these patients. In our study population, 24% of patients not currently using cannabis stated they would consider using it now that it is legalized. Further, although most patients in our study who use cannabis had been doing so for more than 6 months (80%), a substantial number of patients were new cannabis users (16%). This would suggest that we may see an increase in the number of patients using cannabis in the coming years. This trend has been noted in the general population, with a significant increase in cannabis use in the year after legalization.6 Although it is important to recognize higher use among orthopedic patients with upper extremity conditions, it is also prudent to note that a large proportion (71%) were not currently using cannabis and were not considering use (70%). Sensitivity to patient preferences in discussions around cannabis use is necessary and potentially more complex than for other nonprescription medications.
Although reasons for cannabis use varied in our study, the most commonly reported reason for use was pain (56%). Managing pain on an acute or chronic basis is common in the orthopedic population and may explain the increased prevalence of use in our study population compared with the general population in Canada. Other studies evaluating the prevalence of cannabis use specifically in orthopedic patients reported rates from 4.2% to 34%.9–11 These studies varied in methodology, patient age and study period, which may account for differences in the reported prevalence. A similarly designed study by Carney and colleagues9 reported a similar prevalence of cannabis use by orthopedic patients at 34%. Their study evaluated orthopedic patients immediately before surgery, and therefore their cohort may have had more pain than our cohort, which included patients in all stages of recovery.9 In their survey, the most common reason for cannabis use was pain,9 as with our study. Of note, their study was conducted in a time and place where medical, but not recreational, cannabis use was legal.
In our study, most participants reported that they felt cannabis use was safer than prescription narcotics, with a small minority (12%) reporting that they felt it was less safe. Further, 42% were using cannabis for their upper extremity condition. This opinion regarding safety is surprising, given that medical use of cannabis is relatively new and the medical community is in the early stages of learning about the risks and benefits of cannabis use. Several studies have reported perioperative concerns with cannabis use, such as airway obstruction12 and higher anesthetic requirements. The need for greater doses of propofol was specifically found among patients using cannabis at least once per week.13 Similarly, increased cardiac workload, and increased rates of myocardial infarction and stroke have been observed in young, chronic users.14 Cannabis used specifically via inhalation has been shown to result in increased coughing, sputum production and airway hyperreactivity.11,15 In our study, the most commonly reported frequency of use was more than 4 times per week, with other studies also showing high daily use rates, at 30%–40%.7,9 Smoking was the most common form of cannabis use in our study. This illustrates the importance in not only asking patients if they use cannabis, but also quantifying the amount, frequency and form of use. In addition to perioperative anesthetic concerns, cannabis use has been shown to have specific musculoskeletal concerns. In a large retrospective review, cannabis use was associated with a significantly higher revision rate in patients undergoing total hip arthroplasty and total knee arthroplasty.16
Although several studies have highlighted the risks of cannabis use, some have also reported benefits. In a study by Moon and colleagues,17 cannabis use was associated with a decreased mortality rate among patients undergoing total hip arthroplasty, total knee arthroplasty, total shoulder arthroplasty and femur fixation. Studies have also reported improved pain control with cannabis use in orthopedic patients.11,18 One study showed decreased pain in patient operative sites after orthopedic surgery among cannabis users.11 A recent systematic review evaluating cannabis use specifically in orthopedic patients found it to be effective for pain control in most studies, although substantial variability in study methodology was noted, which limited conclusions.18 Further, in vitro and animal studies have reported a positive effect on cellular bone health with cannabis use through promoted osteoblast activity and inhibited osteoclast activity, although the clinical relevance of this is not currently known.19
We found that most participants were more comfortable discussing their cannabis use with their orthopedic surgeon than they were before legalization, with only 6% reporting that they were not more comfortable. Surgeons should therefore expect more questions regarding the risks and benefits of cannabis use from their patients. Medical use of cannabis is relatively new, and many practising surgeons may not have received education about its effects in their medical training. In a study by Sideris and colleagues,20 although many physicians supported cannabis use for medical reasons in their patients, few had appropriate medical knowledge surrounding its use and felt the lack of evidence-based practice guidelines. Recently, Canadian physicians-in-training expressed a desire for more training on cannabis use, with 75% reporting they would need more training to feel comfortable prescribing cannabis.3 This study also showed that patient-initiated discussions on cannabis use were common, highlighting the need for appropriate education of physicians.3
Limitations
Although a survey study design allowed us to more easily capture many participants, this approach has inherent weaknesses. The survey used in this study was not validated, and a validated survey to assess these metrics does not exist. Survey studies are prone to selection bias, and we did not record the number of patients who were asked but chose not to participate. Patients were informed of the study topic before completing the survey through a letter of information. Although societal attitudes surrounding cannabis use are increasingly accepting, perceived negative attitudes regarding cannabis use may have limited some patients’ willingness to participate. Recall bias may have influenced participant answers, and the authors have no means by which to verify responses. Moreover, although most surveys were complete, 4% were incomplete. It is unknown why participants chose not to answer certain questions and whether their answers to these questions would have altered our findings, though this is unlikely given the low number. We had hoped to compare results from the Canadian cohort with the cohort from Chicago, where recreational cannabis use was not legalized; however, given the small sample size from this centre, we were not able to draw meaningful comparisons for all study metrics. We were able to capture a large cohort from across North America, but our results are specific to orthopedic patients with upper extremity conditions; it is unknown whether these results are generalizable to other patient populations.
Conclusion
This large, multicentre study highlights that cannabis use around the time of legalization among patients with upper extremity conditions in Canada is high, with many more patients considering use. Most patients feel that cannabis use is safe, and many are using it for their current upper extremity problem. Given that many of our patients are regularly using cannabis to manage their upper extremity conditions, in various forms, future studies should seek to understand specific musculoskeletal and perioperative risks and benefits of cannabis. Moreover, patients reported that they were comfortable discussing cannabis use with their surgeon. Surgeons should expect these discussions and should educate themselves on the effects of cannabis use in their patients. Future studies of the trends of cannabis use after legalization in Canada would be beneficial.
Acknowledgement
The authors thank Joy MacDermid (McMaster University and Western University).
Footnotes
This work was presented at the American Society for Surgery of the Hand Annual Meeting, San Antonio, Tex., Oct. 1–3, 2020.
Competing interests: Neil White reports research support from Bioventus, Arthrex and Acumud, and speaker and consulting fees from Conmed and Bioventus. Jason Strelzow reports consulting fees from OrthoXel, Acumed, BoneSupport, and speaker fees from Acumed and BoneSupport. He also reports committee participation with the Orthopaedic Trauma Association and the American Society for Surgery of the Hand. He is an associate editor with the Journal of Bone and Joint Surgery and the Journal of Hand Surgery. No other competing interests were declared.
Contributors: Ruby Grewal conceived and designed the study. Tom Goetz, Neil White, Armin Badre, Braden Gammon, Andrew Trenholm and Jason Strelzow acquired the data. Laura Sims, Neil White, Braden Gammon and Andrew Trenholm analyzed and interpreted the data. Laura Sims drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
- Accepted July 20, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.