


Abstract
Background: Increasing strain on public health resources in Canada, in particular with respect to accessing specialist care, necessitates the exploration of alternative models of care. The aim of this study was to assess the efficacy of electronic consultation (eConsult) in providing orthopedic surgery specialist service to patients in the Champlain Local Health Integration Network (LHIN) of Ontario.
Methods: This was a cross-sectional review of all 564 Champlain LHIN orthopedic surgery referral requests received via the Champlain Building Access to Specialist service through the eConsult (BASE) system in 2017. Primary outcome measures were impact on primary care provider (PCP) referral pattern and time to receive orthopedic consultation.
Results: eConsult prevented unnecessary in-person consultation 64% of the time, while PCP referral decisions were modified 51% of the time. Of all eConsults, 94% were rated as valuable to PCPs in their practice and 97% of eConsults resulted in actionable advice. eConsults took an average of 14.5 minutes of specialist time to complete, and the mean time from referral to response was 3.7 days.
Conclusion: The eConsult system spares unnecessary consultation to orthopedic surgery; catches important referrals that would have otherwise been missed; saves time for patients, PCPs and orthopedic surgeons; and improves efficiency in a socialized health care system.
Wait times for specialist services, including orthopedic surgery, are growing in Canada owing to the inability of the limited resources provided by a socialized health care system to meet the demands of an aging demographic.1 Wait time has several components. The patient must first present to a primary care provider (PCP) who has availability. The PCP must then recognize the problem and refer to a specialist. Specialists, in turn, must then see the patient, diagnose and schedule an intervention as needed. As of 2018, the average time between PCP referral and orthopedic surgical intervention in Canada was 39.0 weeks, including a 14.6-week wait from PCP referral to specialist appointment.1–3 This is the longest wait experienced across all specialties4 and is longer than the clinically agreed-upon acceptable wait for surgical intervention (13.5 wk) established via surveys of experienced clinicians in the field.1 This wait for specialist response has increased from 8.1 weeks in 1993, highlighting the increasing strain experienced in Canada’s social health care system.1,4 The Champlain Building Access to Specialists through eConsultation (BASE) system is a novel platform that addresses the wait time between PCP referral and specialist response.5
Longer wait times have been shown to adversely affect patient outcomes.6–9 Patients in Canada requiring spine surgery have demonstrably worse functional outcomes if they wait longer for surgery,6 and those forced to wait for joint replacement experience a linear decline in their chance for a good functional outcome for every additional month they wait. Further, those who waited for extended periods of time for revision joint arthroplasty had increased pain and disability.8 Several studies reiterate the point that longer waiting times lead to poorer functional outcomes after joint replacement,7,9–11 in addition to the pain and suffering inflicted upon patients forced to wait.9,10,12,13
Not only does waiting cause direct harm to patients, but the economic impact is also substantial. Ostendorf and colleagues calculated that for each additional month spent waiting for total hip arthroplasty, a patient can expect to lose 0.035 quality-adjusted life-years.10 The Centre for Spatial Economics estimates the cost of waiting for each joint replacement surgery performed in Canada at $26 400,14 and Sommerville and Stokes estimate a total cost of $99 million to the province of Ontario each year.14
Access to specialty services is not a new problem, but as wait times grow, this burden is exacerbated. A study of family practice referrals to specialty service in 2017 showed that 36% of all specialist referrals went unacknowledged at 7 weeks, including 38% to surgical specialties and 43% for orthopedic surgery specifically.15 This is corroborated by 2018 Ontario health statistics, which show that less than 31% of priority 2 patients (i.e., should be treated within 42 days, according to Health Quality Ontario’s own metrics) receive care in that time frame.4 There is an imperative extant in the current Canadian health care system to provide a more efficient means of specialist care. Few previous studies have shown promising results,16,17 especially in the Canadian context.18 The Champlain BASE platform is secure, does not require overlapping time commitments and allows instant remote access between PCPs and specialists. The aim of this study is to describe the impact of eConsult on PCP referral pattern and wait time for orthopedic specialist response in Ontario.
Methods
Study design
We performed a cross-sectional analysis of PCP referral patterns, questions, diagnoses and outcomes of orthopedic eConsult in the Champlain Local Health Integration Network (LHIN) in 2017.
System employed
Two of the authors (C.L., E.K.) developed the Champlain BASE service in Ottawa with assistance from the Champlain LHIN, to facilitate remote access to specialist medical services. A protocol for its delivery was published previously.5
In brief, this system allows interaction between PCPs and orthopedic surgeons through a standardized form with additional ancillary information (for example, laboratory results and imaging) attached. The orthopedic surgeon can then offer advice as to treatment decisions and whether further referral or contact is warranted or care can be deferred to a more appropriate specialty or subspecialist with orthopedics. Each interaction is associated with a mandatory survey (Box 1) that assesses the utility to the patient, the impact on subsequent in-person consultation and the utility to the PCP. The specialist is reimbursed at $200 per hour, pro-rated to time spent consulting to a maximum of 1 hour.19 This platform has been endorsed by regulatory bodies in Ontario as an acceptable standard of care for patient consultation.20,21
Questions asked of primary care providers at terminus of eConsult.
Which of the following best describes the outcome of this eConsultation for your patient?
I was able to confirm a course of action that I originally had in mind
I got a clear advice for a new or additional course of action that I will be implementing
I got a clear advice for a new or additional course of action that I am not able to implement
None of the above
As a result of the eConsultation would you say that
Referral was originally contemplated but now avoided at this stage
Referral was originally contemplated and is still needed
Referral was not originally contemplated and is still not needed
Referral was not originally contemplated, but eConsult process resulted in a referral being initiated
How helpful and/or educational was this response in guiding your ongoing evaluation or management of the patient? (Likert scale 1–5).
Study participants
The Champlain LHIN comprises a population of roughly 1.3 million residents in Eastern Ontario, who receive specialist services from 1 tertiary care hospital system in Ottawa, Canada.22 We analyzed 564 eConsults received by orthopedic surgeons in Eastern Ontario from all areas of the Champlain LHIN completed through the Champlain BASE service from January to December 2017. All study participant identities were kept confidential, and each case was assigned a coded number to ensure anonymity.
Data collection
All data were collected and stored securely in the Champlain BASE system via robust methods, described elsewhere.5 We collected these data prospectively at the time of eConsult and analyzed them retrospectively. Data collected included the reason for eConsult, the written dialogue of the conversation, the length of time to receive a response, the results of the encounter and PCP response surveys.
Data review
Two independent reviewers (W.J.H and B.M.) reviewed eConsults to orthopedic surgery in 2017 and categorized them by clinical topic and type of question asked, using predetermined categories.
Disclosure
Two authors (C.L. and E.K.) were involved in the development and implementation of the Champlain BASE system. Neither receive compensation for the use of this system. Neither are involved in using this system with regularity (C.L. consults via this platform about once per month).
Results
In 2017, a total of 564 eConsults submitted through the Champlain BASE service were received and reviewed by an orthopedic surgeon. This represents 4.6% of all eConsults sent. Of these orthopedic referrals, 10% were from nurse practitioners and 90% were from family physicians. The average time for the PCP to receive a response after placing a request for consultation was 3.7 days (median 4.0 d), and 94% were answered within 7 days. The average amount of time required of an orthopedic surgeon to respond to these consult requests was 14.5 minutes.
We defined 9 types of clinical questions and 27 clinical problem categories. The most frequent question type asked was classed as “general management” (197/564 [35%]), in which either multiple questions were asked, or the essential question was “what should I do next?”. The second most common question asked was whether surgery was indicated (126/564 [22%]) (Figure 1).

Type of question asked by primary care providers of orthopedic surgeons via the eConsult system.
The most frequent topic questions were those related to spine pathology (71/564 [13%]), undifferentiated pain (62/564 [11%]), pediatric orthopedics (57/564 [10%]) and soft tissue injuries (56/564 [10%]) (Figure 2).

Content of question asked by primary care providers of orthopedic surgeons via the eConsult system.
Overall, 56% of primary care providers received new and actionable advice from eConsult, and an additional 42% were able to confirm an uncertain course of action. Further, only 2% of eConsults resulted in advice that PCPs were unable to implement (Figure 3).
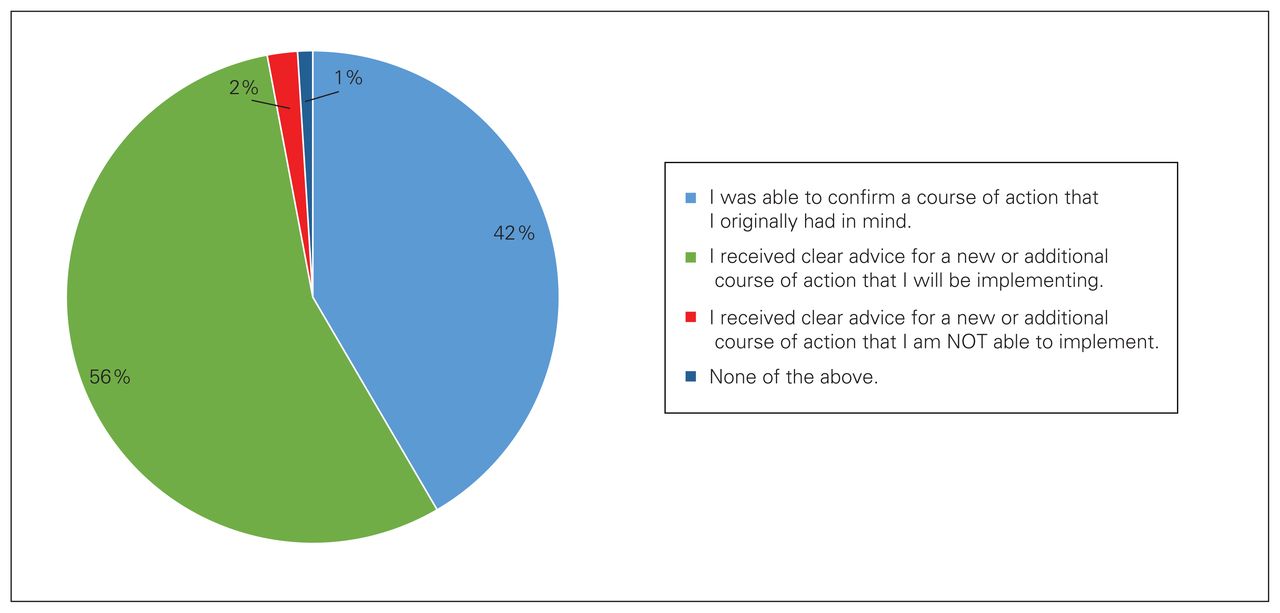
Primary care provider response to survey question 1.
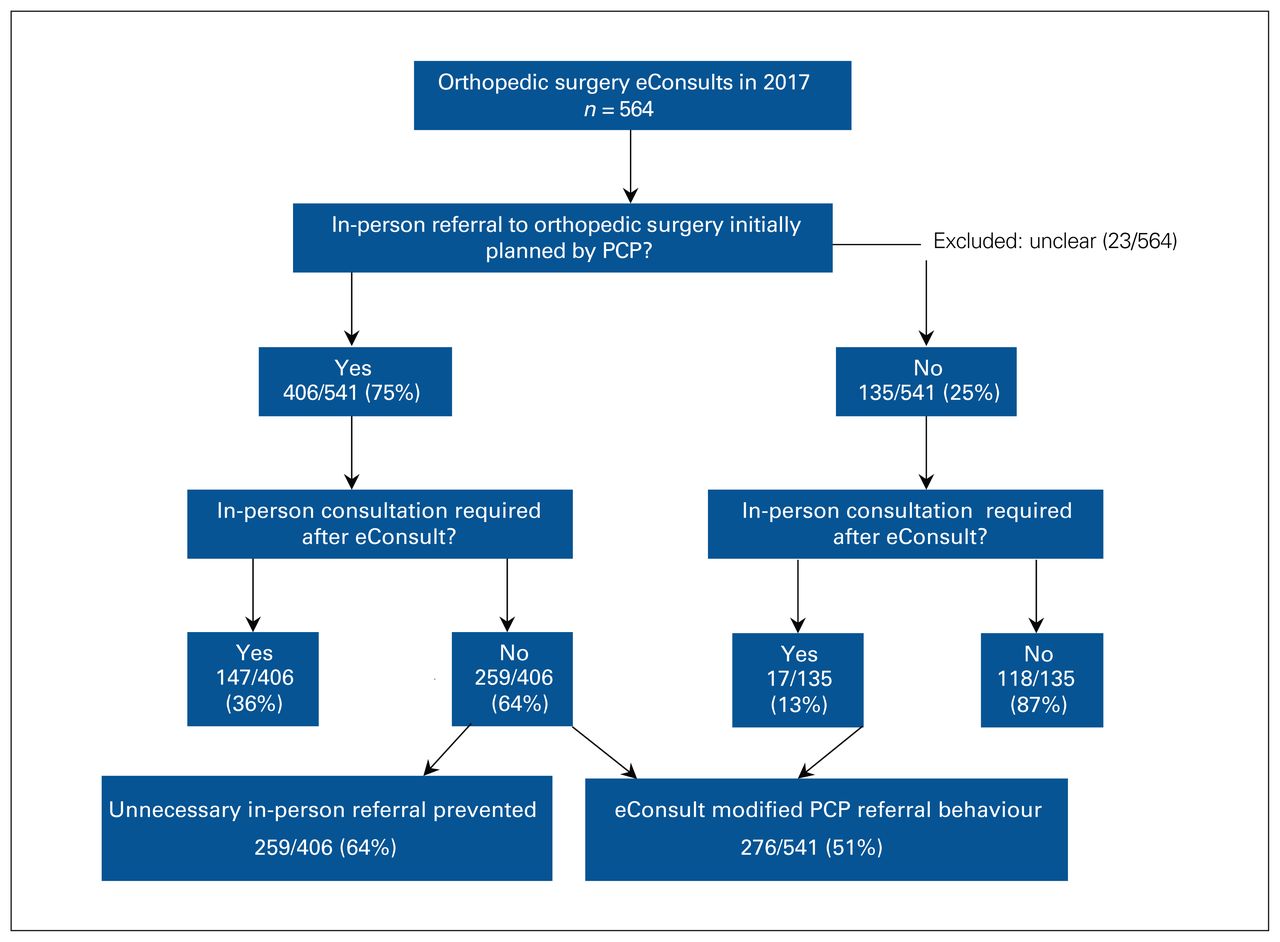
The consequence of eConsult is shown in Figure 4. Unnecessary referral was avoided in 64% of cases originally planned for referral, and PCP decisions were altered 51% of the time. Importantly, 13% of patients originally not considered to need orthopedic specialist care were indeed referred after eConsult for consideration of operative management.

Impact of the eConsult system on the decision to refer to an orthopedic surgeon. PCP = primary care provider.
Finally, the eConsult system’s perceived value to PCPs was ranked as “valuable” and “very valuable” 22% and 72% of the time respectively (Q3, Box 1).
Discussion
eConsultation is the provision of remote care where that care is deemed safe by all participants: PCP, orthopedic surgeon and patient. Although this is not a traditional consultation model, this study shows the impact the eConsult system can have on both wait times to receive specialist advice and subsequent referral patterns to in-person consultation. Although wait time from PCP referral to appointment with an orthopedic surgeon in Ontario currently averages 14.6 weeks, the average time for response to an eConsult was 3.9 days. In cases where in-person referral was not ultimately necessary, this system was clearly superior, sparing wait and travel time for the patient and clinic time for the orthopedic surgeon. Further, the average time spent on eConsult cases was reported as 14.5 minutes, arguably less than the average time spent on a clinic visit when the clerk, technician, nurse and surgeon’s time are taken into consideration. This study further found that 64% (Figure 4) of all cases originally planned for referral to an orthopedic surgeon were not ultimately necessary after eConsult. With nearly 500 000 office visits to orthopedic surgeons occurring each year in Ontario,23 the potential to add efficiency to this system is clear. Not only does eConsult save time for the patient, PCP and orthopedic surgeon involved, time is freed up and wait-lists are shorter for those who do require in-person consultation.
A corollary and significant finding of this study is that 13% (Figure 4) of patients initially not considered to need in-person consultation were indeed referred after eConsult. This is an important patient population that might have otherwise been lost (or at least delayed) to necessary orthopedic follow-up and potential intervention. As mentioned, there are health, quality of life and economic impacts to delayed treatment of common orthopedic problems like end-stage osteoarthritis requiring joint replacement.7–10,24
Although other methods have been implemented to address the strained resources experienced in remote and rural settings in Canada, eConsult offers a potential solution to a large fraction of these cases because it does not require both parties to interact at the same time (telemedicine) or demand expensive and time-consuming gap training of nonorthopedic surgeons (PCP adjunct courses). Given the relative efficiency of eConsult compared with traditional in-person consultation in the rural and remote context, we advocate for the increased use of eConsult in these settings. Conversely, we acknowledge that this model may lend itself to operational drift when PCPs ask questions that do not make efficient use of specialist time (i.e., the management of undifferentiated back pain). Our study does note additional interactions between PCPs and orthopedic surgeons (135, as shown in Figure 4) that would not have otherwise occurred. These additional interactions cancel out some of the efficiency gained by deferring unnecessary in-person consultations (259, as shown in Figure 4). Overall, we believe this model is best suited as a complementary platform alongside current programs that provide rapid access to ancillary medical care (care for low back pain, for example).25
In an era of increasing access to medical data, outcomes, collaborative treatment plans and research all require meticulous data gathering. The eConsult system facilitates these goals by keeping a comprehensive and complete record of the physician–physician interaction. It also provides a protective mechanism for physicians delivering care, as all advice and treatment decisions are documented.
Limitations
Limitations exist in the outcomes reported by this study. Namely, objective follow-up data are lacking and are not currently a component of this system. It remains to be seen whether long-term outcomes after eConsult compare with traditional models of health care delivery in a Canadian context, as this may not be true in other models.18 Whether PCPs learn from ongoing interaction to add further efficiency to the system, or begin to ask less suitable questions to detract from it, remains an important question. Because patient safety and follow-up after deferral of in-person orthopedic consultation remain the responsibility of the PCP, it is possible that some cases requiring operative intervention may be missed. It is difficult to imagine that this cohort would eclipse the 13% catch rate shown in Figure 4 of patients not initially considered to need consultation, but data to support or refute this are lacking and constitute the most important present weakness of this platform.
This study is also limited by its relatively small sample size (representing roughly 0.1% of all office visits to orthopedic surgery in Ontario in 2017) and its limited current engagement (a majority of eConsults to orthopedic surgery in 2017 were completed by fewer than 10 different surgeons).
This sample of patients also suffers from selection bias in that those clearly needing joint replacements are referred automatically, and those with a common orthopedic problem with a known solution (wrist and hip fractures) are rarely the subject of an eConsult, presumably because they have been captured at local emergency departments.
Conclusion
There are important trade-offs in any health care system; the principle of triple constraint demands this. Canada has chosen to sacrifice wait times for universality and quality, and therefore we must be honest about the negative impact this system has on its people. The ever-increasing wait times experienced by patients in Canada for specialist intervention constitute a grievous imposition on both those who fund the system with their tax dollars and those who rely on it for care. Pain, suffering and inferior outcomes are inflicted on patients during their wait for specialist care. The eConsult system alleviates a small part of this by adding efficiency and thereby sparing the limited resources provided by a social health care system. This model prevents unnecessary referral to orthopedic surgery, catches referrals that would otherwise be missed and, when appropriate, delivers care in a much faster, more cost-effective manner than traditional in-person referral.
Footnotes
Competing interests: Erin Keely reports employment as the co-executive director of the Ontario eServices team, which is funded by the Ontario Ministry of Health, for oversight into eConsult programs. Dr. Keely uses the system and receives compensation, approximately once per month. Clare Liddy and Erin Keely are co-executive directors of the Ontario eServices program. No other competing interests were declared.
Contributors: William Hadden and Brad Meulenkamp contributed to the conception and design of the work. Sheena Guglani, Alenko Sakanovic, Clare Liddy and Erin Keely contributed to the acquisition, analysis and interpretation of data. William Hadden contributed to drafting the manuscript. Sheena Guglani, Alenko Sakanovic, Clare Liddy, Erin Keely and Brad Meulenkamp revised the manuscript critically for important intellectual content. All of the authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
- Accepted September 27, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.