


Summary
The establishment of a single health authority in Saskatchewan in 2017 paved the way for the creation of the provincial Department of Surgery that oversees surgical services and academic activities across the province of Saskatchewan. The consolidation of surgical activities under 1 administrative infrastructure and leadership facilitated a coordinated delivery of surgical care to the people of Saskatchewan and notably increased academic productivity. The value of a provincial surgical department was evident during the COVID-19 pandemic and enabled a rapid and cohesive response to the challenges of surgical service delivery provincewide. Although this model of a provincial department may not be able to be applied to every jurisdiction, it has worked well in a province of 1.18 million people and 252 surgeons. A major achievement of this model has been the enhancement of communication, coordination and collaboration among 14 surgical sites and their surgeons.
On Jan. 4, 2017, the Government of Saskatchewan announced the creation of a single provincial health authority1 following the recommendations of an Advisory Panel on Health System Structure.2 The panel recommended the amalgamation of 12 regional health authorities into a single Saskatchewan Health Authority (SHA) and the consolidation of clinical services under 1 administrative umbrella. The panel also recommended a standardized approach on eHealth, procurement and physician recruitment. The SHA became the largest employer in Saskatchewan, with 43 000 staff and a budget that reached $4.24 billion in 2022.
Although single health authorities were created in Alberta and Nova Scotia, an approach to integrate clinical and academic missions at a provincial level was introduced in Saskatchewan with the creation of provincial departments chaired by provincial departmental heads. These provincial departmental heads (reporting to both the dean of the University of Saskatchewan College of Medicine and the chief medical officer of the Saskatchewan Health Authority) provide leadership to enable a seamless integration of clinical and academic activities of the provincial department and identifiy gaps, assess needs and articulate strategies to enable clinical and academic planning to ensure the quality and safety of health care delivery to the residents of Saskatchewan.
We explored the structure and the role of the Department of Surgery in Saskatchewan in integrating clinical and academic mandates. We also focused on the advantages and challenges of a provincial mandate in the delivery of surgical care to an entire province and the experience during the COVID-19 pandemic.
Provincial departmental model
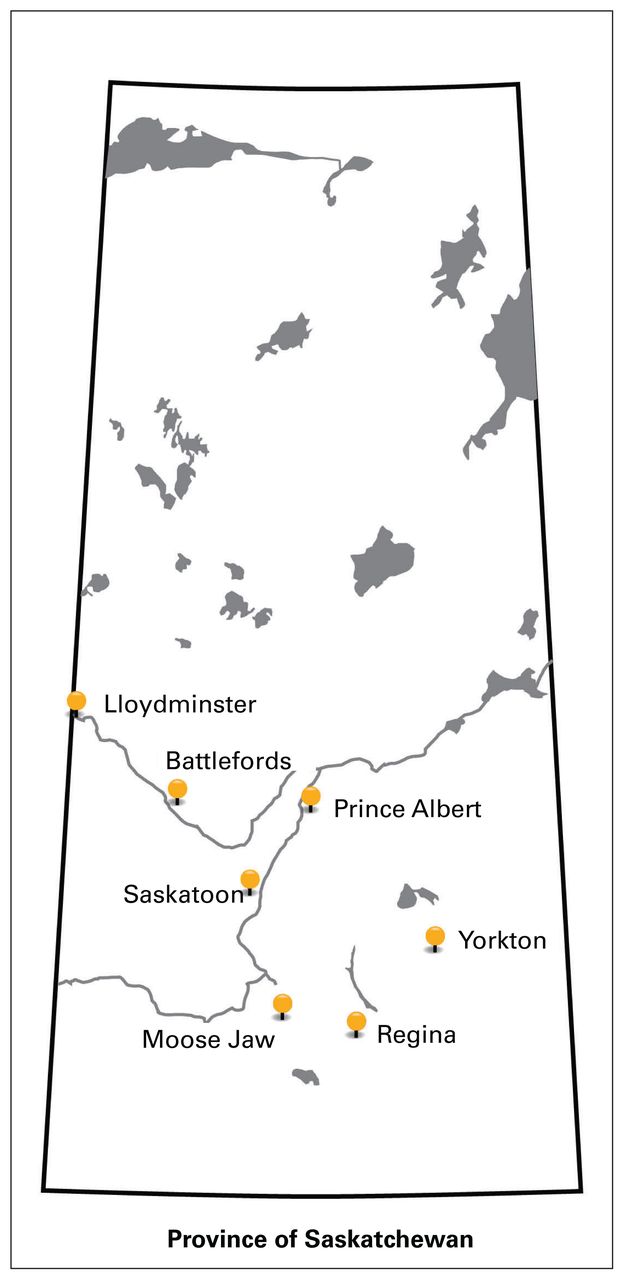
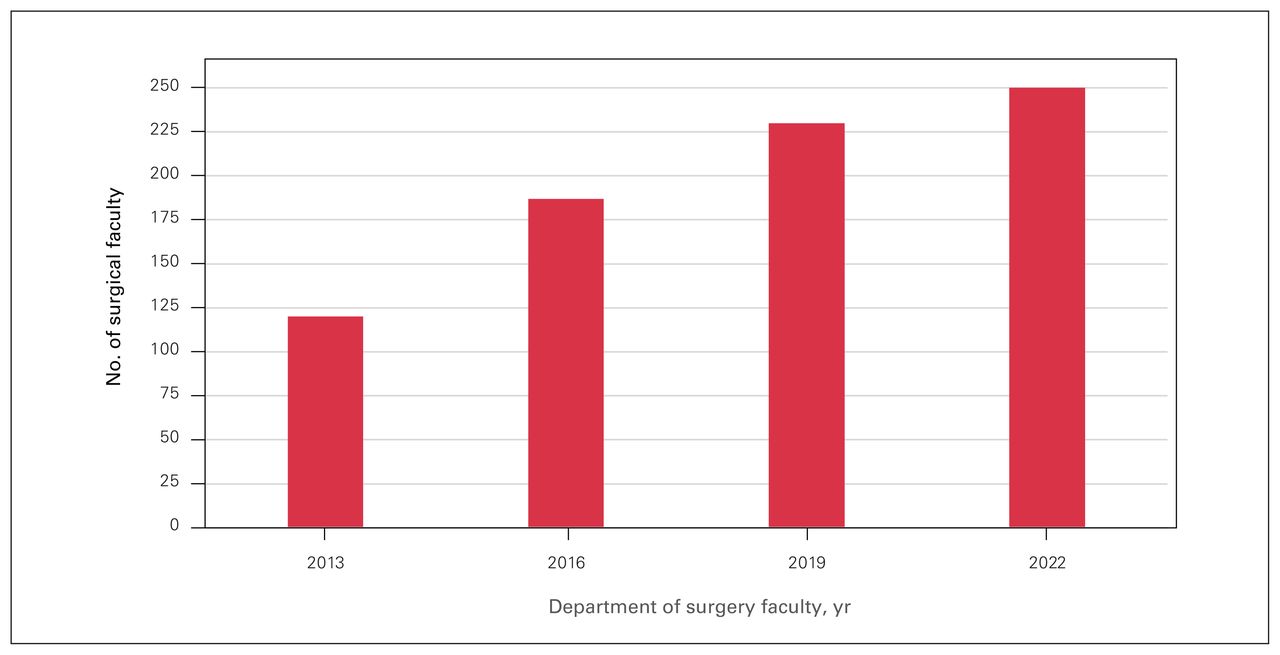
Saskatchewan was ideal for the establishment of a single provincial Department of Surgery, with a population of 1.18 million (36% living in rural areas) and a large territorial extension of 651 900 km2.3 There are 7 regional surgical centres in Saskatchewan (Figure 1). Surgeries are performed in 14 hospitals distributed across the province, affiliated with the 7 regional centres. Surgical volumes before the start of the COVID-19 pandemic were more than 90 000 procedures per year (Table 1). For the past 9 years, the department has experienced an unprecedented growth, doubling the number of faculty to 252 surgeons in 2022 (Figure 2).

Map of the province of Saskatchewan showing the geographic distribution of regional surgical centres.

Number of surgical faculty in the province of Saskatchewan.
Surgical procedures by location in Saskatchewan
The core of the Saskatchewan provincial department governance structure is the Saskatchewan Surgical Council (Figure 3), which includes the area department leads from the 7 regional surgical centres and is chaired by the provincial departmental heads of surgery. The area department leads oversee the day-to-day surgical services in their regions, as well as academic and quality improvement activities, and report to the provincial departmental heads and the area chief of staff of each region. The division heads report to the area department leads and supervise the service and academic function of their surgical specialty. The departmental directors of education, research, quality improvement and surgical humanities report to the provincial departmental heads and provide leadership and support to the area department leads and division heads to fulfill their program missions across the province (Figure 4).
Saskatchewan Surgical Council, from left to right: Dr. Nishaan Cheddie, ADL, Moose Jaw; Dr. Sharon Koubi, ADL, Yorkton; Dr. Oladapo Mabadeje, ADL, Prince Albert; Dr. Gary Groot, director, quality improvement; Dr. Joan Wheat-Hozack, ADL, Lloydminster; Dr. John Tsang, ADL, Regina; Dr. William Dust, ADL, Saskatoon; Dr. Ivar Mendez, provincial head surgery. ADL = area department lead.
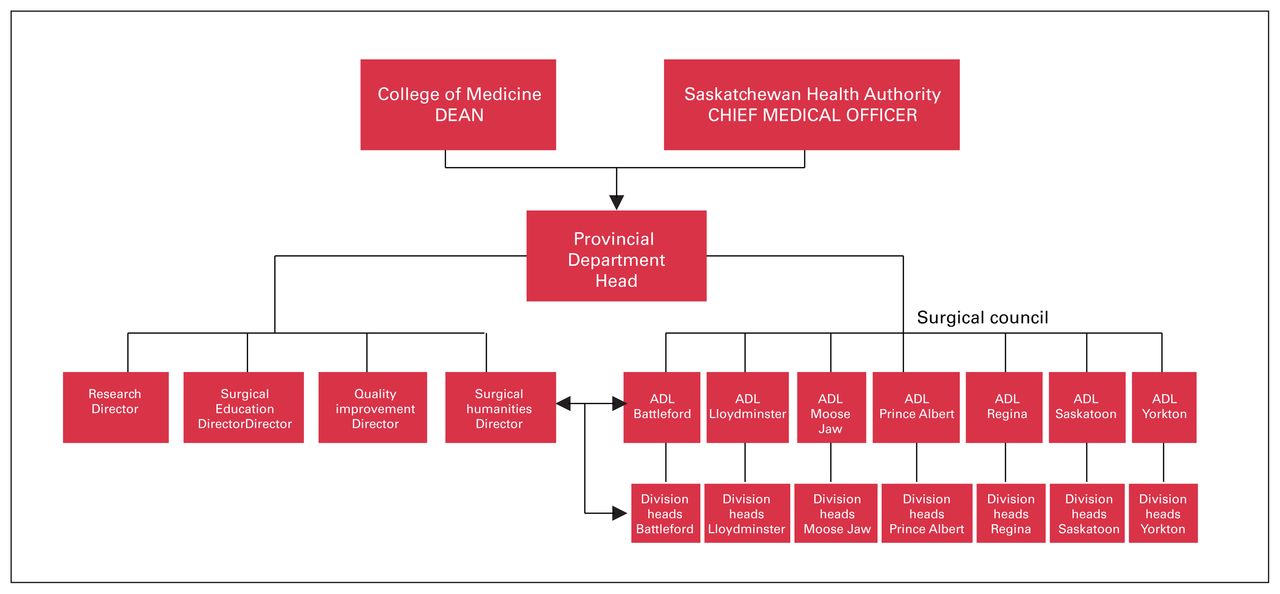
Organizational chart of the Saskatchewan provincial Department of Surgery. ADL = area department lead.
The council meet every 3 weeks, although during the height of the pandemic, meetings were increased to weekly. The council receives reports from all regions regarding clinical status and academic activities. This update was crucial during the pandemic as it allowed a coordinated surgical response to specific needs or crisis situations.
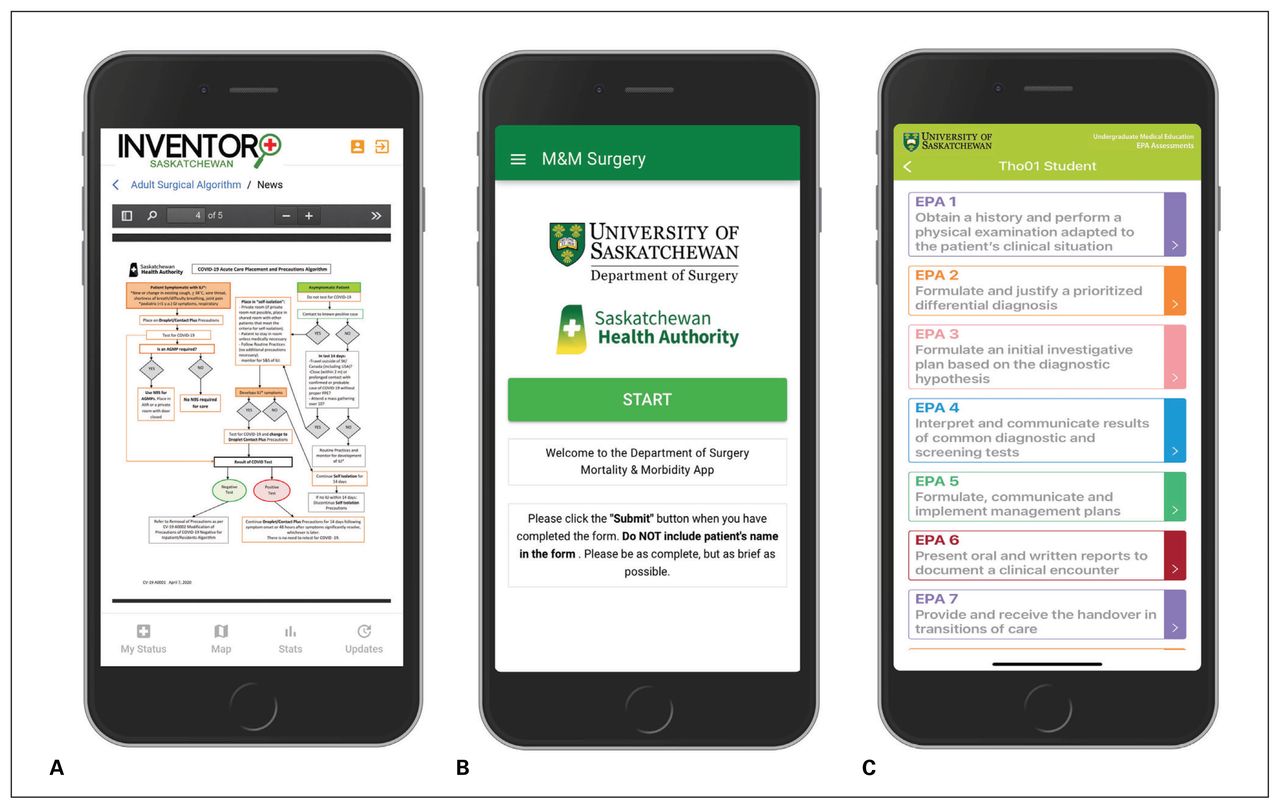
Communications across all departmental administrative structures and membership are facilitated by a dedicated communications office that has access to all department members. Electronic biweekly communications highlight the clinical and academic accomplishments of department members, a quarterly newsletter and annual report provide an in-depth overview of departmental activities. The department developed 3 proprietary smartphone apps (available to all department members) for quality improvement, undergraduate education and the management of the pandemic response (Figure 5).

Screen shots of proprietary smartphone apps: (A) Inventory, COVID-19 app, (B) Morbidity and mortality rounds app, (C) Entrustable professional activities app.
Clinical service and COVID-19
The primary mandate of the provincial department is the provision of surgical services to the people of Saskatchewan based on the principle that any citizen of Saskatchewan should receive the best surgical care possible regardless of their geographical location. This task is greatly facilitated by having a single provincial health authority that oversees the credentialing of all surgeons. Although surgeons are recruited to practise in specific centres, this common credentialing process allows the flexibility of surgeons to provide clinical support to other Saskatchewan centres when needed, such as during the pandemic.
The department’s common provincial human resource strategy with a single recruitment process fulfills the needs of different regions. It supports recruitment to smaller centres, avoids duplication and promotes the creation of centres of excellence. Standardization of surgical services and equipment across the province is an important goal of the department. Mobility of surgeons and patients increases surgical access and facilitates service level loading to different regions. This promotes development of smaller centres and decompresses the surgical burden on the busiest regions of Regina and Saskatoon.
Surgical mentoring and collaboration in surgical regions are enabled by use of innovative remote presence technology. This includes surgical mentoring in the operating room, virtual care to reduce interfacility transport and remote diagnostic robotic technology.4,5 Surgical working rounds at a provincial level are conducted regularly by several divisions and facilitate consultations and referrals within the province. Enhancing the surgical capacity of smaller rural and remote centres is essential as one-third of the population in Saskatchewan lives in rural areas.3 There are considerable barriers to accessing health care services by these populations.6 Increasing surgical access to these underserved populations is a priority for the department.
Quality improvement initiatives, such as the implementation of standardized morbidity and mortality rounds in all Saskatchewan surgical centres are possible owing to the provincial nature of the department. We have created a morbidity and mortality rounds smartphone app (Figure 5) available to all Saskatchewan surgeons and in addition to a provincial Surgical Quality & Safety Committee that has representatives from all regions. The department participates in the National Surgical Quality Improvement Program, started 3 years ago in Saskatoon, which is the largest surgical centre of the province and is being expanded to other Saskatchewan centres.
The value of a provincial surgical department was evident during the pandemic. By March 2020, the province-wide administrative and communications structures within the department were in place. We formed a cohesive unit for real-time analysis of pandemic information, decision-making and knowledge dissemination for front-line surgical teams across Saskatchewan. The department coordinated a provincial surgical approach to ensure the continuation of emergency, urgent and cancer surgeries. Guidelines for the postponement of elective procedures and a roadmap for surgery resumption were established. The department developed and deployed a proprietary smartphone app called Inventory (Figure 5) to access real-time information of the SARS-CoV-2 status of all surgeons in the province and areas of increased SARS-CoV-2 activity. The Inventory app also provided information on surgical algorithms and guidelines, which was useful throughout the pandemic as they changed in response to increased understanding of SARS-CoV-2, the different variants, new therapies and the advent of vaccines. With the Inventory app, surgeons across Saskatchewan had, at their fingertips, updated information to ensure the safety of patients and surgical teams. The department is fully engaged in a provincial strategy to deal with the pandemic backlog of surgeries; an effective use of both the physical and human resources across all regions of the province will be crucial in dealing with the backlog. Current challenges include the expansion of provincewide initiatives, such as level loading of patients across surgical centres, pooled referrals, Enhanced Recovery After Surgery and the switch of inpatient surgery to day surgery.
Academic mission
The academic activity in surgical centres in Saskatchewan has been enhanced by incorporating centres under a provincial academic departmental structure. When the establishment of the provincial department occurred, surgeons practising in Saskatchewan were offered assistant professor status at the University of Saskatchewan. This offer was accepted by 98% of all surgeons. This increase in surgical faculty at a provincial level boosted the ability of the department to fulfill its academic mission and expand academic activities to regions that were traditionally focused on clinical service alone.
The new faculty were given access to all university services, funding opportunities and academic promotion streams. Teaching at the undergraduate and postgraduate level, as well as participation in clinical and research rounds and quality improvement programs became a requirement for all members regardless of their location of practice. Provincial surgical grand rounds were implemented and transmitted to all centres by videoconferencing.
As the College of Medicine has a distributed learning model, surgeons in smaller centres had the opportunity to teach undergraduate medical students. The department delivered 14 000 undergraduate teaching hours across the province in 2019. The department developed a proprietary smartphone app for the documentation of entrustable professional activities that was deployed in all surgical clerkship’s rotations regardless of their geographical location (Figure 5).
From their base in Saskatoon, the rotation of surgical residents to different surgical centres in the province was implemented. These rotations were highly rated and allowed the residents to experience different regions and practice patterns and establish relationships with their local surgical teams. This has contributed to the retention of these residents in Saskatchewan and has increased recruitment to smaller centres of the province.
Opportunities for research funding and collaboration were open to all Saskatchewan surgeons. A provincial research office was established with a full-time research coordinator and biostatistician services. The office provides direct support to researchers for submission of funding applications, ethics approval, research contracts, manuscript preparation and publications. Productivity has increased as more surgeons participate in research; this increase in academic activity has been remarkable as surgery was traditionally service-oriented in Saskatchewan (Figure 6).

(A) Peer-reviewed publications, (B) Research funding.
The department established a surgical humanities program with the goal of engaging surgeons, residents and medical students in music, art, poetry, drama, literature, history of medicine and philosophy. The program also focused on emerging social issues concerning inclusivity, equality, diversity and social justice. A quarterly publication called the Journal of Surgical Humanities was established. A surgical humanities day was instituted with a public lecture, an exhibition of art by members of the department and a classical music concert with an ensemble orchestra of surgeons, residents and medical students.
Conclusion
The province of Saskatchewan established the first provincial Department of Surgery in Canada in 2017. The full range of surgical and academic activities across Saskatchewan now fall under the umbrella of a single department and its leadership. The consolidation of clinical services and academic mission under this administrative structure facilitated the coordinated delivery of surgical care to the people of Saskatchewan and increased academic productivity. The siloed structure of 12 different health authorities, each with its own independent surgical department, has been transformed into a cohesive administrative unit with equitable regional representation. By the onset of the pandemic in March 2020, the department had successfully transitioned the amalgamation process and its administrative and communication processes had matured. This maturity was crucial in successfully facing the challenges of the pandemic that allowed us to maintain vital surgical services across the province despite surgical slowdowns, kept our patients and surgical teams safe and dealt with the large surgical backlog.
The creation of a provincial surgical department had a major effect on the academic activity of surgeons across Saskatchewan. Traditionally, the emphasis was on clinical service and academic activities were relegated to a distant second place. The incorporation of all Saskatchewan surgeons into the University of Saskatchewan College of Medicine and improving access to academic mentoring, funding and collaboration made the department the thriving academic entity it has become. Quality improvement programs at the provincial level have been possible with the implementation of standardized morbidity and mortality rounds and the expansion of the National Surgical Quality Improvement Program to other Saskatchewan centres, which will lead to better surgical care.
Although this model of a provincial department may not apply to every jurisdiction, it has worked well in a province with 1.18 million people and 252 surgeons distributed in 14 locations. A major achievement of this model has been the enhancement of communication, coordination and collaboration of the 14 surgical sites and their surgeons. Building and strengthening relations among centres and surgical teams has been the platform upon which the Saskatchewan provincial Department of Surgery stands today.
Footnotes
Contributors: All authors contributed substantially to the conception, writing and revision of this article and approved the final version for publication.
Competing interests: None declared.
- Accepted July 12, 2022.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools





