

Abstract
Objectives: To determine the population-based incidence of splenic injuries in the Province of Ontario, the proportion of splenic injuries treated by observation, splenectomy and splenorrhaphy, changes in management over time and the variation in management of splenic injuries among Ontario hospitals.
Design: A retrospective cohort study.
Patients: All adults (older than 16 years) admitted with a diagnosis of splenic injury (clinical modification of the International Classification of Diseases, 9th revision) to acute care hospitals in Ontario between 1991 and 1994, identified from the Ontario Trauma Registry.
Results: The incidence of splenic injury was 1.7 cases per 1000 trauma admissions per year. Patients with splenic injury were young (median age 32 years) and male (71%), and the death rate was 8%. Observation was the commonest method of treatment (69%), followed by splenectomy (28%) and splenorrhaphy (4%). The use of observation increased over the study period from 59% to 75% (p < 0.001). There was significant variation in the use of observation among hospitals (range 11% to 100%, p < 0.0001).
Conclusions: The majority of splenic injuries are managed by observation with an acceptable hospital death rate. The use of observation has increased over time, confirming the growing adoption of this management approach by most hospitals in the province when feasible. Splenorrhaphy was infrequently performed despite reports to the contrary from many centres in the United States. There was significant variation in splenic injury management, suggesting the need for further refinement and dissemination of practical guidelines for splenic salvage.
Salvage of the injured spleen in adults has been championed as the optimal management strategy for blunt trauma. Splenic salvage may be accomplished by observation or splenorrhaphy. Advocates of observation have argued that this approach avoids laparotomy in many splenic injuries and reduces the risk of later post-splenectomy sepsis.1–7 The alternative salvage strategy is splenorrhaphy, and several authors have indicated a clear preference for this approach.8–11 Proponents of splenorrhaphy contend that when observation fails, the patient is more likely to undergo splenectomy and that splenorrhaphy more effectively accomplishes splenic salvage without exposing patients to the risks of blood transfusion. No studies in adults address the issue of who should undergo splenorrhaphy and who should be managed by observation. Splenectomy is reserved mainly for hemodynamically unstable patients or those having extensive anatomic injury.
Most of the literature describes experience at 1 or 2 centres, giving little information as to how widely splenic conservation is adopted among different hospitals over the same period of time. One study reporting results from North Carolina12 found that the use of observation for splenic injuries increased in that state from 33% to 49% over 5 years, but the study did not determine the proportion of patients treated by splenorrhaphy. More recently, the same group found that more than one-half of all splenic injuries resulted in conservation of the organ, being accomplished by observation in 40% and by splenorrhaphy in 12%.13 Although 2 Canadian studies have documented a preference for observation as the treatment of choice in blunt trauma,14,15 there is little information about the current standard of practice in managing blunt splenic injuries among many Canadian hospitals.
Studies of variation in practice patterns evaluate the adoption of a particular management strategy by clinicians. 16,17 Such an analysis would provide a better perspective of the extent to which splenic salvage strategies are employed and the degree to which this varies among hospitals over time. A population-based study would also provide an estimate of the frequency of splenic injuries, which remains poorly defined.
Our objectives in this study were as follows: to provide a population-based estimate of the frequency of adult splenic injuries in Ontario; to determine the proportion of adult splenic injuries managed by splenectomy, splenorrhaphy and observation within the province; to assess changes in management over time; and to measure the amount of variation in the use of splenic conservation strategies among provincial hospitals.
Method
The study population was a retrospective cohort of all adults (age more than 16 years) who had splenic injuries and were treated at acute care hospitals in Ontario during the period January 1991 to December 1994. There were 11 hospitals that were designated as Level I trauma centres for their regions. Data were obtained from the Ontario Trauma Registry (OTR) (a branch of the Canadian Institute for Health Information) from 2 existing data sets. The minimal data set contained limited information on all admissions to acute care hospitals in the province, including age, sex, type of injury and operative procedures using classification codes of the clinical modification of the International Classification of Diseases, 9th revision (ICD-9-CM),18 length of hospital stay and death rate. The comprehensive data set contained detailed information on all trauma admissions with an injury severity score (ISS)19 greater than 12 to Level I trauma centres within the province. Data contained in the comprehensive set included demographics, admitting systolic blood pressure, associated anatomic injuries, ISS, revised trauma score (RTS)20 and Glasgow coma scale (GCS) score.21 Duplicated records due to transfer from one hospital to another were dealt with by either taking the most recent admission as the one of record or taking the admission during which splenectomy or splenorrhaphy was performed as the index admission for that splenic injury.
Patients with splenic injury were identified using the ICD-9-CM code 865 (856.01–865.14). Splenic operations were identified by using the ICD-9-CM procedure codes 41.5 (splenectomy) and 41.95 (splenorrhaphy). Patients were then divided into 3 groups based on the method by which they were managed: observation, splenorrhaphy and splenectomy. The frequency of failed observation could not be accurately determined from the OTR data. Changes in management over time were assessed by determining the proportion of splenic injuries treated by each of these methods during each year of the study.
Variation in management among hospitals was assessed by determining the proportion of patients treated by observation divided by the total number of treating hospitals. The variation in the proportion of observation by hospital was estimated for all hospitals as well as the Level I trauma centres. To test whether variation by hospital arose by chance, the log-likelihood ratio was tested against the null hypothesis that the logistic regression coefficients for each hospital were equal to each other. Multiple logistic regression was used to assess the simultaneous effects of predictive factors. Factors hypothesized to affect variation in management included the following: age; provincial region; year of admission; hospital caseload of splenic injuries; presence of shock (systolic blood pressure < 100 mm Hg) on arrival to the Emergency Department; presence of severe head injury (defined as GCS score less than 7 or head abbreviated injury score greater than 2); the presence of multiple (2 or more) injuries; and whether the hospital was designated as a trauma centre. A probability value of 0.05 was considered statistically significant.
Results
Incidence of splenic injuries
During the 4-year study period, 2147 patients were admitted to 147 acute care hospitals in Ontario for the management of splenic injury. Of these, 1688 patients were 16 years of age or older. The total number of trauma admissions over the study period was 253 872, giving a hospital-based incidence of 1.7 splenic injuries per 1000 trauma admissions per year. The population-based incidence of splenic injuries for Ontario was 5.1 cases per 105 person-years (the population of Ontario aged 16 years or greater in the 1992 census was 8 318 474).
Splenic injury management in all Ontario hospitals
Patients with splenic injury had a mean age of 32 years (interquartile range [IQR] 27 years) and 71% were male (Table I). Observation was the commonest method of treatment in 69% (1161 patients) followed by splenectomy in 28% (467 patients) and splenorrhaphy in 4% (60 patients). The in-hospital death rate for all patients in the province with splenic injuries was 8% (135 patients) and the median length of stay was 8 days (IQR 10 days). The splenorrhaphy group had a significantly lower death rate than the observation group (0% versus 8%, p = 0.04). There were no other differences among groups. Unfortunately, the absence of information on the injury mechanism and standard ISSs in this data set precluded further comparisons.
Characteristics of Patients Who Had Splenic Injuries Treated in 147 Acute Care Hospitals in Ontario, Grouped by Method of Treatment
Management of splenic injuries in Level I trauma centres across Ontario
Only 658 (39%) of all documented splenic injuries were treated in designated trauma centres in the province (Table II). The median patient age was 31 years (IQR 23 years) and 70% were male. Blunt injury as the causative mechanism occurred in 95%, and the median number of injuries per patient was 8 (IQR 7). Associated injuries to the thorax (77%) and head (59%) were the most common. The diagnosis of splenic injury was made by computed tomography in 37% and diagnostic peritoneal lavage in 16%. The method of diagnosis was unspecified in 47%. Although the median GCS score was 15, 20% of patients had profound depression of conciousness as indicated by a GCS score of 7 or less. The median ISS was 34 (IQR 19), and 32% of patients demonstrated shock on arrival at the Emergency Department (defined as systolic blood pressure less than 100 mm Hg). The death rate was 20% and the median length of hospital stay was 14 days (IQR 22).
Characteristics of Patients Who Had Splenic Injury and Were Treated at Level I Trauma Centres in Ontario, Grouped by Method of Treatment
Observation was the commonest form of management in 65%, followed by splenectomy in 33% and splenorrhaphy in 2% (Table II). Significantly more patients who underwent splenectomy demonstrated shock on arrival at the hospital than those managed by observation (43% versus 27%, p = 0.03). Although the death rate in the patients treated by splenorrhaphy was again lower than in those managed by observation or splenectomy (7% versus 22% and 18% respectively), the differences were not statistically significant. There were no other significant differences among groups.
Time trend for the management of splenic injury across all provincial hospitals
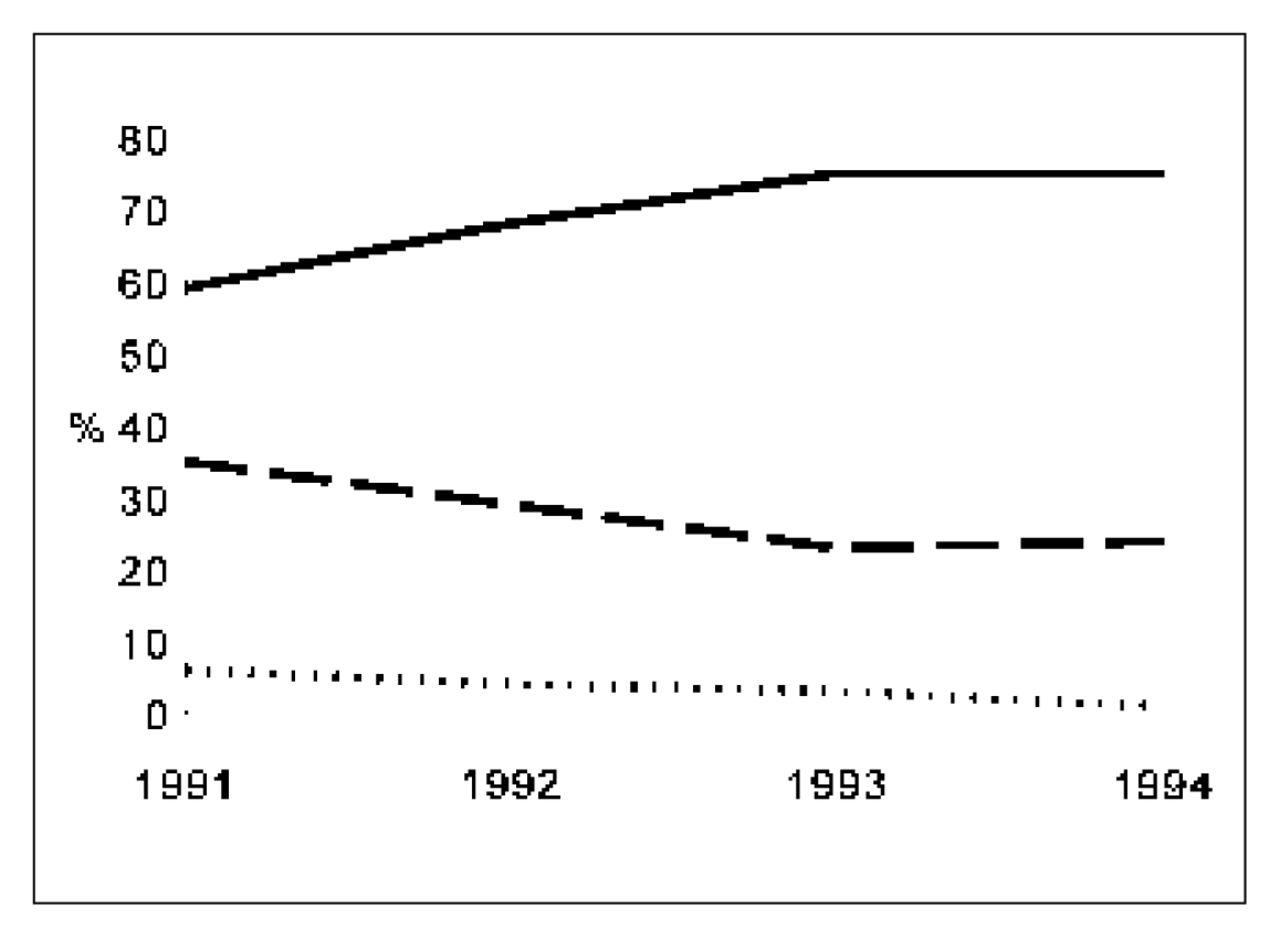
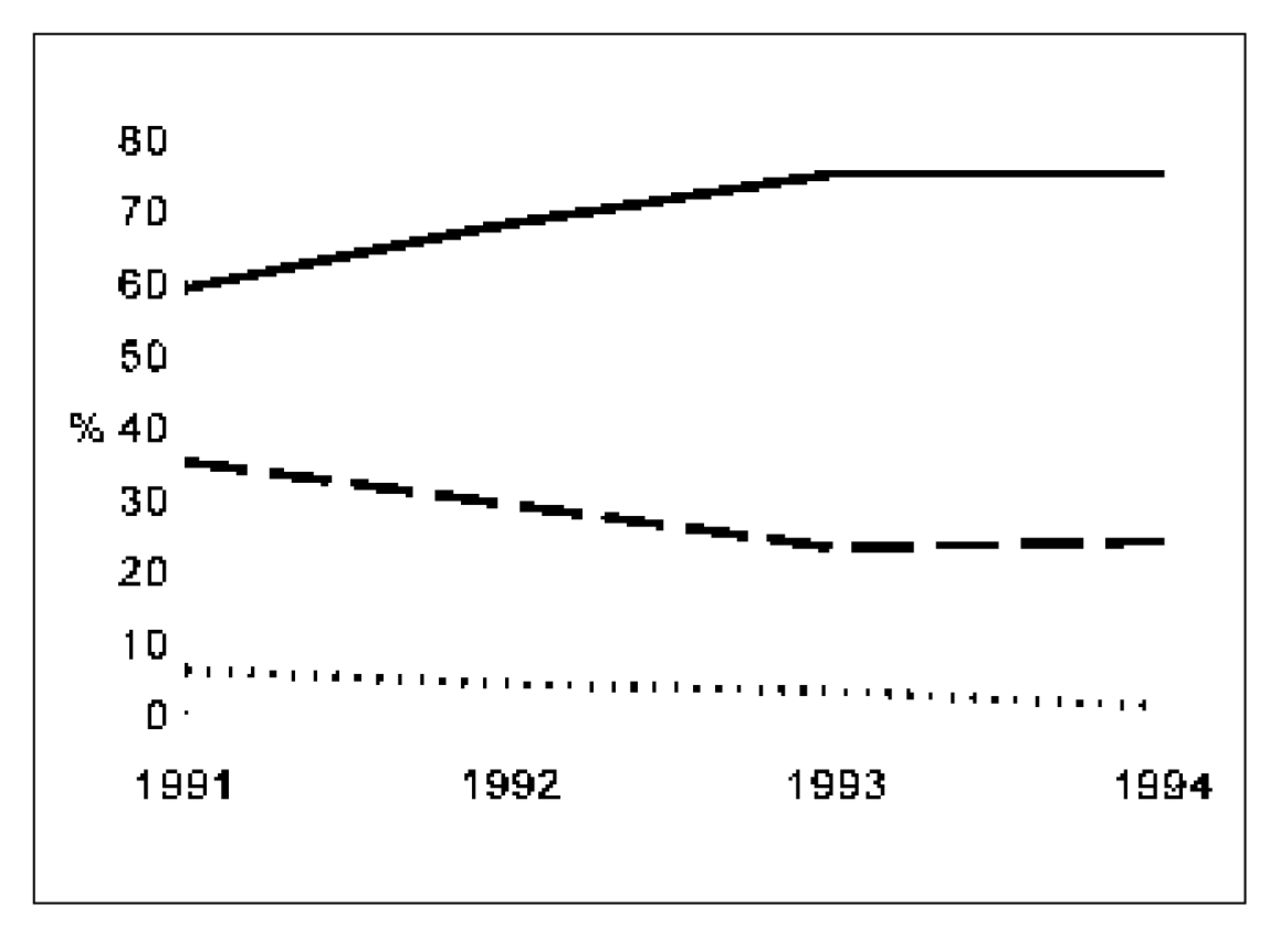
The proportion of patients whose splenic injuries were managed by observation increased from 59% in 1991 to 75% in 1994, whereas the use of splenectomy decreased from 35% to 24% over the same time period (Fig. 1) (p < 0.001). Use of splenorrhaphy decreased during this period from 6% to 1%.
{kind=link}
Time trend for the management of splenic injuries by year of admission in all Ontario hospitals. Observation (solid line) significantly increased while splenectomy (broken line) and splenorrhaphy (dotted line) decreased (χ2 = 33.6, p < 0.001).
Variation of splenic injury management by hospital
The use of observation varied significantly among all acute care hospitals, ranging from 11% to 100% (p < 0.0001). Factors influencing the choice of splenic injury management in all Ontario hospitals are reported in Table III. The use of observation was most affected by the treating hospital but was also affected by the year of admission and patient age. The geographic region, lead trauma hospital designation, hospital caseload and patient sex did not influence the choice of treatment.
Logistic Regression Model of Factors Influencing Variation in the Proportion of Patients Treated by Observation in all Ontario Hospitals
Significant variation was also present in the use of observation among Level I trauma hospitals (33% to 100%, p < 0.0001). Factors predicting the use of observation in trauma centres were the presence of multiple (2 or more) injuries and the presence of shock (systolic blood pressure less than 100 mm Hg) on arrival at the hospital (Table IV). There was still significant variation in management among trauma centres after controlling for these factors.
Logistic Regression Model of Factors Influencing Variation in the Proportion of Patients Treated by Observation at Level I Trauma Hospitals in Ontario
Discussion
Although injuries to the spleen are of great concern in the management of trauma patients, there are no reliable estimates of the incidence of this injury in the literature. This study reveals that injuries to the spleen are relatively uncommon, occurring in 1.7 cases per 1000 trauma admissions per year in the average Ontario hospital. The significant mortality of 8% bolsters the argument that such injuries are best managed by experienced clinicians.
Most injuries (72%) resulted in salvage of the spleen. Observation represented the single largest treatment group in this cohort; splenorrhaphy was rarely used. This practice pattern was similar regardless of whether patients were managed in a trauma designated or non-trauma designated hospital. In contrast, Clancy and associates13 recently reported that splenectomy constituted the largest treatment group among trauma centres in North Carolina. Despite this difference, they found that observation still represented the most commonly employed method of splenic conservation, in 40% of cases, whereas splenorrhaphy was used in 12%. There were no differences in death rate or length of hospital stay between patients treated by observation or splenectomy in either our study or that of Clancy and associates, 13 confirming that the use of observation is safe in appropriately selected patients.
The use of observation significantly increased across Ontario over the study period whereas splenectomy and splenorrhaphy decreased. This trend is similar to that in an earlier report from the United States12 and confirms the growing adoption of observation as the management of choice.
Since the primary goal of this study was to describe the current practice pattern in the management of splenic injuries across Ontario hospitals, a study of practice variation was also performed. Such studies have been employed to evaluate the adoption of various management strategies.16,17 We found that despite the growing adoption of observation, the use of this method varied significantly across all Ontario hospitals. This variation was partially explained by patient age and year of admission but not by hospital caseload of splenic injuries or the level of expertise (trauma designated versus non-trauma designated) of the treating hospital. Similarly, variations found in the use of observation in the trauma-designated hospitals were only partially explained by injury severity parameters such as the presence of shock or multiple injuries. Although it is conceivable that variation in management is due mainly to variation in the severity of splenic injury presenting to different hospitals, it is equally conceivable that other factors may well be contributing to this finding.
It has been stated that the most important factor affecting practice variation is physician practice style and the lack of consensus on the diagnosis and treatment of the condition.22,23
Differences in selection criteria for who should undergo observation as well as differences in transfusion practices likely account for some of this variability and cannot be adequately assessed in a retrospective database study. Although the literature is replete with large case series of observation in blunt splenic injury,1–7 only a single study developed prospective guidelines for the successful use of this approach. Smith and colleagues6 found that hemodynamic stability, age less than 55 years, CT appearance of grade I, II or III injury, absence of other injuries complicating assessment, and absence of other abdominal injuries were all correlated with successful use of observation in blunt splenic injuries. We found that only some of these factors accounted for the variation in the use of observation in Ontario trauma centres. Consistency in the management of splenic injury will come about only after further refinement of prospectively derived guidelines that can be reliably applied in order to produce safe and successful use of observation.
Splenorrhaphy has been advocated by many as a safe method of splenic conservation.8–11 Proponents of this approach contend that those who fail observation are more likely to undergo splenectomy and that splenorrhaphy more effectively accomplishes splenic salvage without exposing patients to the risks of ongoing transfusions. No studies in adults have identified selection criteria to determine which injuries would be better managed by splenorrhaphy than by observation. Conceivably, both strategies would produce similar results in comparable patients. Indeed, in the series by Feliciano and associates,8 92% of repairs involved only compression, simple suture or topical application of hemostatic agents, suggesting that some of the patients could have been managed by observation. Regardless of its potential advantages we found that splenorrhaphy was infrequently performed and that its use significantly decreased over time. Similar results from the North Carolina trauma registry13 suggest that few surgeons believe this to be the optimal method of conservation in the majority of blunt splenic injuries.
This study is limited by our inability to identify cases of unsuccessful observation. Consequently, we canot ascertain whether this management method was appropriately used and whether any deaths resulted from not performing splenectomy sooner on some patients. Although there was no means of determining the frequency of ICD-9-CM coding errors, it is unlikely that such errors would systematically occur in one treatment group over another, thereby biasing the final results and conclusions. Finally, we were limited by the absence of severity stratification of the splenic injury in the non-trauma hospitals, which could further explain variations in management. Consequently, the results of this study only document the current practice pattern, and we cannot conclude that all factors that can affect variation have been controlled for. Moreover, we cannot conclude that one form of splenic injury management has been demonstrated by our data to be superior to another. Only by prospective studies that subject patients with similar injuries to different treatments can such conclusions be drawn.
In summary, although splenic injuries are infrequently encountered in the community, the death rate remains significant. Splenic preservation is now a widely adopted method of management and is almost entirely accomplished in the Canadian setting by observation, the use of which has steadily increased with time. Despite potential advantages of splenorrhaphy, we have shown that it is rarely used. The existence of variation in practice of splenic injury management may partly be attributable to uncertainty by some practitioners about the optimal selection criteria for splenic conservation. Consistency in management would be facilitated by further prospective development and dissemination of usable criteria that identify cases of splenic injuries for which the spleen can be successfully salvaged.
Footnotes
Presented at the annual meeting of the Trauma Association of Canada, Vancouver, BC, Sept. 24, 1997.
- Accepted January 13, 1999.