

Case report
A 65-year-old woman presented to the emergency department with a 36-hour history of constant epigastric pain, back pain and obstipation. Her medical history included chronic obstructive pulmonary disease (COPD) and a remote hysterectomy. Her pain was sudden in onset following a violent sneezing episode. On examination, the patient’s vital signs were within acceptable limits. There was minimal distention of the abdomen with no bowel sounds. There was no peritonitis on palpation. All laboratory investigations, including a lipase, were normal. There was concern that this could have been aortic pathology, so a CT with intravenous contrast only was ordered (Fig. 1). This led to a diagnosis of bowel obstruction; gastric versus cecal volvulus were both entertained. We proceeded with an upper gastrointestinal (GI) contrast study that demonstrated normal flow of contrast but with a gas shadow in the lesser sac displacing the stomach superiorly and anteriorly (Fig. 2). A contrast enema demonstrated a proximal narrowing of the colon just before filling the cecum in the lesser sac. At this time, the diagnosis of cecal herniation through the foramen of Winslow was made, and the patient proceeded to laparotomy, where the diagnosis was confirmed. The bowel appeared viable and was easily reduced through the foramen, which permitted 2 fingers to pass through. The patient had a redundant right colon that had failed to retroperitonealize. A right hemicolectomy was performed. The patient tolerated the procedure well and was discharged from hospital 4 days later.
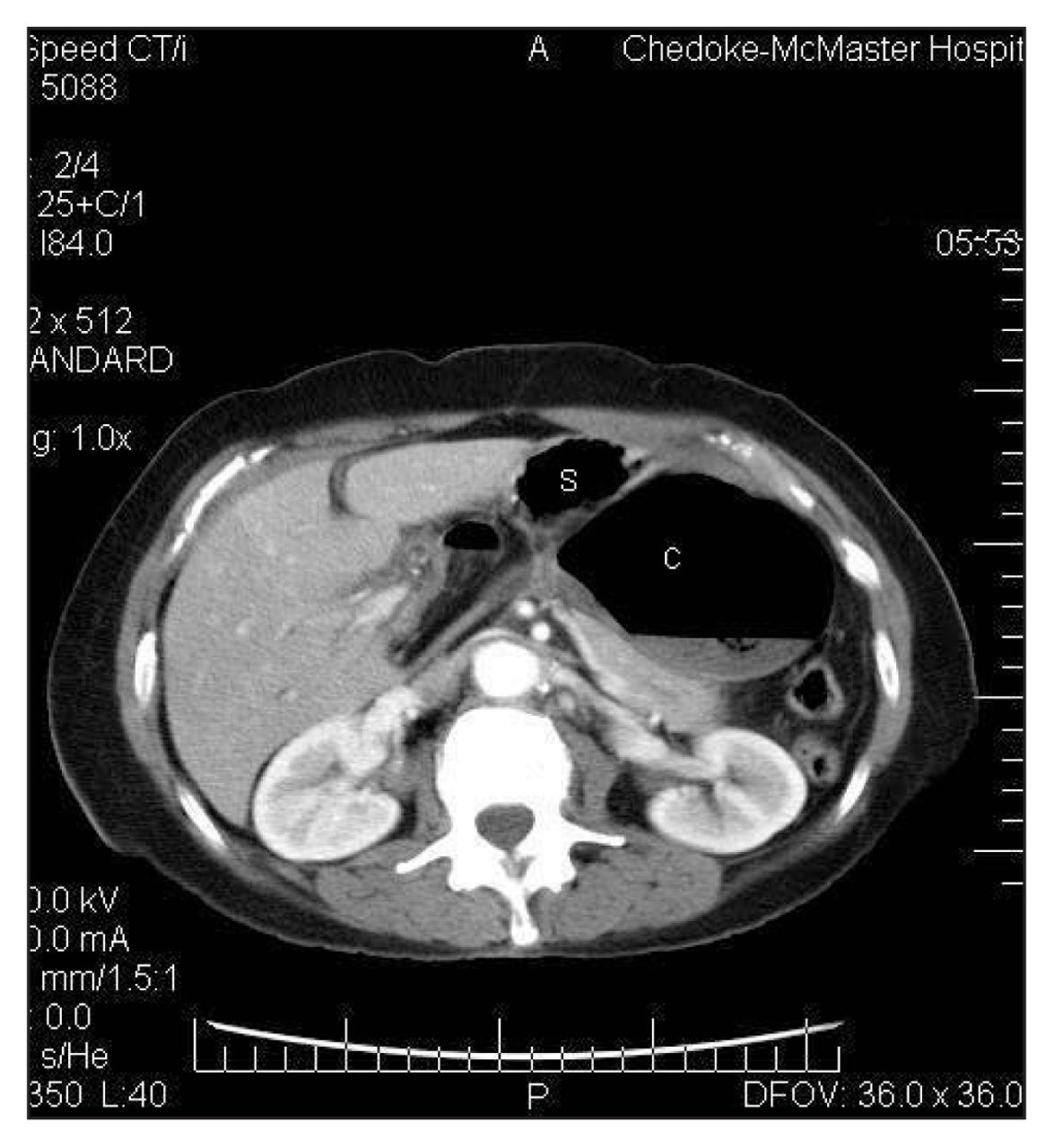
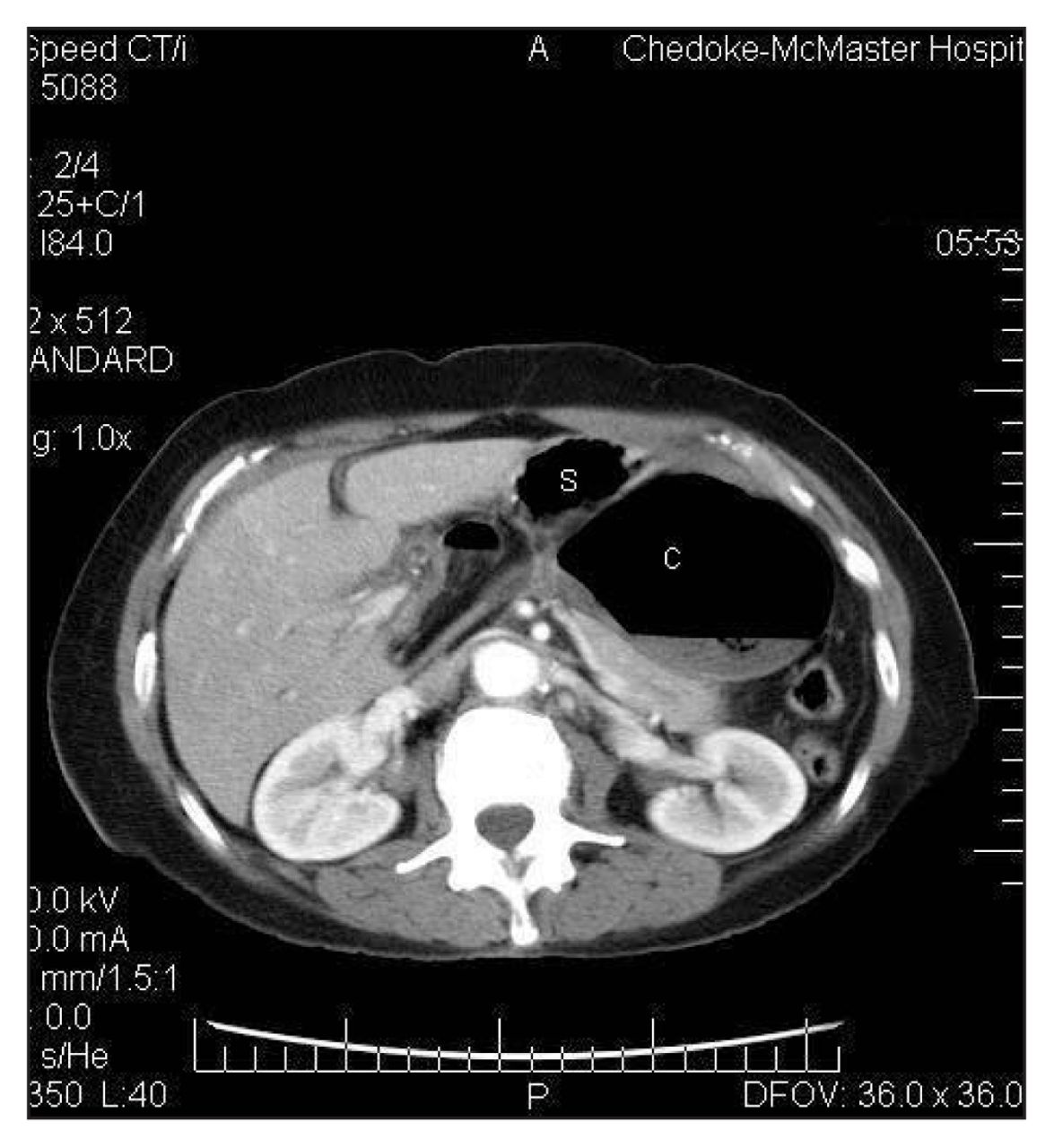
CT scan showing gas collection behind the stomach. Note the mesentery forming a bird’s beak pointing toward the patient’s right. S = stomach, C = cecum.

{kind=link}
{kind=link}
Lateral view from the upper gastrointestinal study demonstrating a retrogastric gas collection with colonic features. S = stomach, C = cecum.
Discussion
Internal hernia through the foramen of Winslow is a rare occurrence, accounting for less than 0.1% of all abdominal hernias. 1 In a thorough review of the disease, Erskine summarizes the major risk factors: 1) a common intestinal mesentery, 2) failure of the right colon to retroperitonealize, 3) a long small bowel mesentery, and 4) a large foramen of Winslow (described as being one that admits more than one finger).2 Erskine also notes that changes in intra-abdominal pressure may be a contributing factor in the presence of these risk factors. Interestingly, our patient reported a sneezing fit before the onset of her abdominal symptoms, which may well have been the inciting factor in her case. Intraoperatively, our patient was found to have a mobile right colon with a marginally enlarged foramen.
Originally described as an operative diagnosis, preoperative diagnosis of herniation through the foramen of Winslow is possible with a variety of imaging modalities. Several authors have described the plain film findings. Typically, the gastric bubble is displaced laterally and anteriorly by a lesser sac mass.3 CT scan features described by Wojtasek and subsequently by Schuster include the following: 1) mesenteric fat and vessels posterior to the portal vein, common bile duct and hepatic artery; 2) gas and/or fluid in the lesser sac with a “bird’s beak” pointing toward the epiploic foramen; and 3) the cecum absent from its anatomic position.4,5
The upper GI study helped to differentiate the gastric bubble from the lesser sac gas. The lower GI study confirmed the suspicion of a lesser sac hernia with the contrast narrowing in the colon (while passing through the foramen) before filling the cecum in the lesser sac.
At laparotomy, the right colon was found viable in the lesser sac. Surgical options include resection of the involved bowel, versus cecopexy. Most authors to date have found ischemic bowel, warranting resection. There are few instances in the literature where viable bowel was found, although no consensus has been established on management in this instance. We elected to resect the affected bowel, intending to eliminate any chance of disease recurrence.
Footnotes
Competing interests: None declared.
- Accepted April 22, 2005.