

Intussusception in adults occurs infrequently and differs from childhood intussusception in its presentation, cause and treatment. In adults, it accounts for about 2%–3% of bowel obstructions.1 In contrast to childhood intussusception, 90% of cases in adults are associated with an underlying pathologic process such as a malignant lesion. In adults, intussusception is more likely to present insidiously with vague abdominal symptoms and rarely presents with the classic triad of vomiting, abdominal pain and passage of blood per rectum, making diagnosis difficult. CT findings are pathognomonic for intussusception, making CT the most effective diagnostic test.
Case report
A 31-year-old woman presented with a 6-day history of right-sided abdominal pain and several episodes of hematochesia. She had experienced a single episode of emesis 6 days before presentation. She was afebrile, with pain on palpation of her abdomen 5 cm to the right of the umbilicus. A 3-cm mobile mass was palpable at the site of maximal tenderness. She had no peritoneal signs and a leukocyte count of 11.3 × 109/L. CT of the abdomen demonstrated findings consistent with colocolonic intussusception (Fig. 1).

CT scan of the abdomen showing intussusception in the middle portion of the ascending colon. Lead point is a large fat-containing mass.
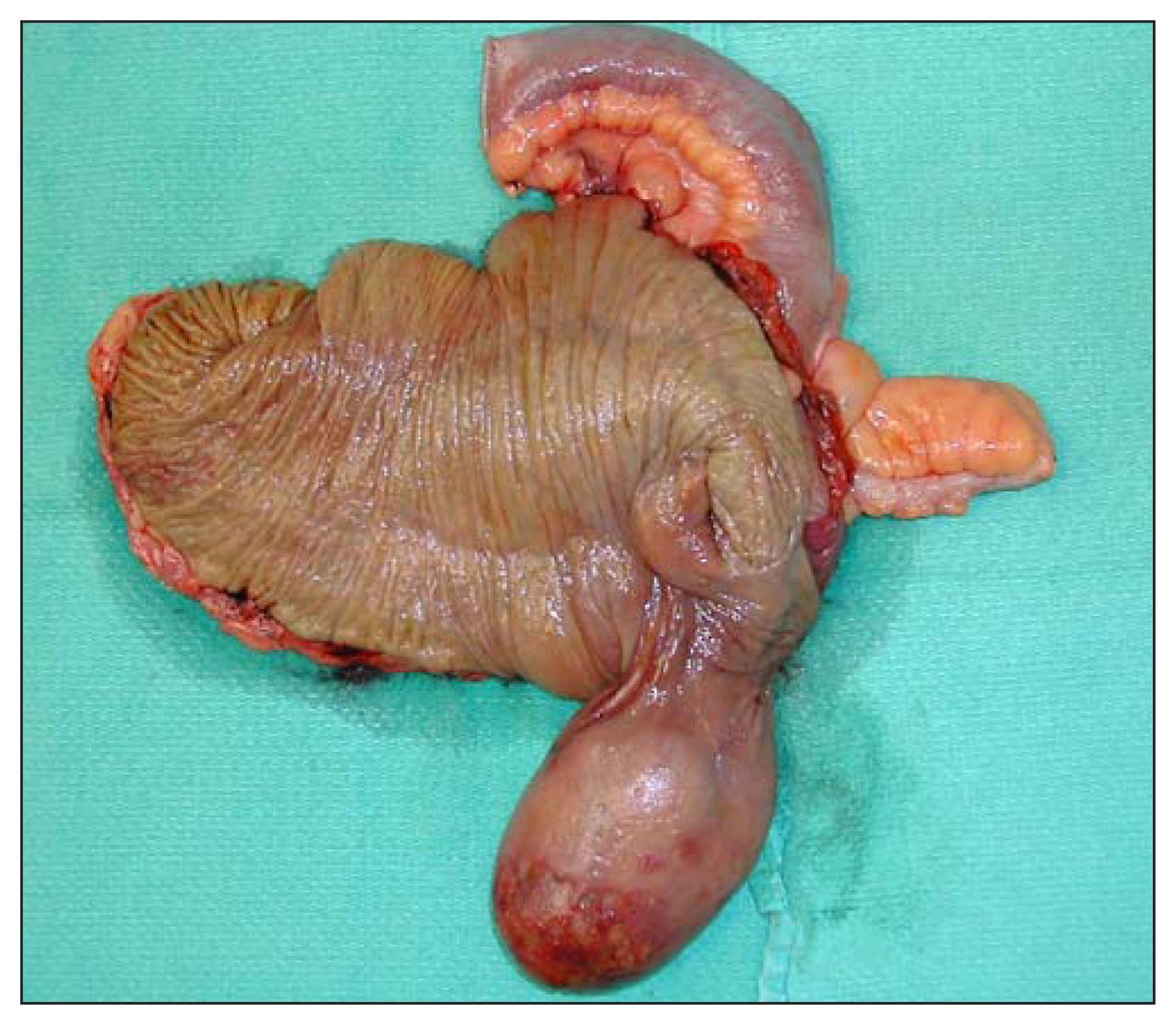
Laparotomy demonstrated a mass in the right ascending colon with no signs of intussusception, leading us to believe that the intussusceptum had spontaneously resolved. A right colectomy with side-to-side anastomosis was performed. The resected colon was opened and a submucosal pedunculated lesion was seen in the proximal cecum (Fig. 2). Pathological examination identified the mass as a lipoma (Fig. 3). The patient’s recovery was uncomplicated.
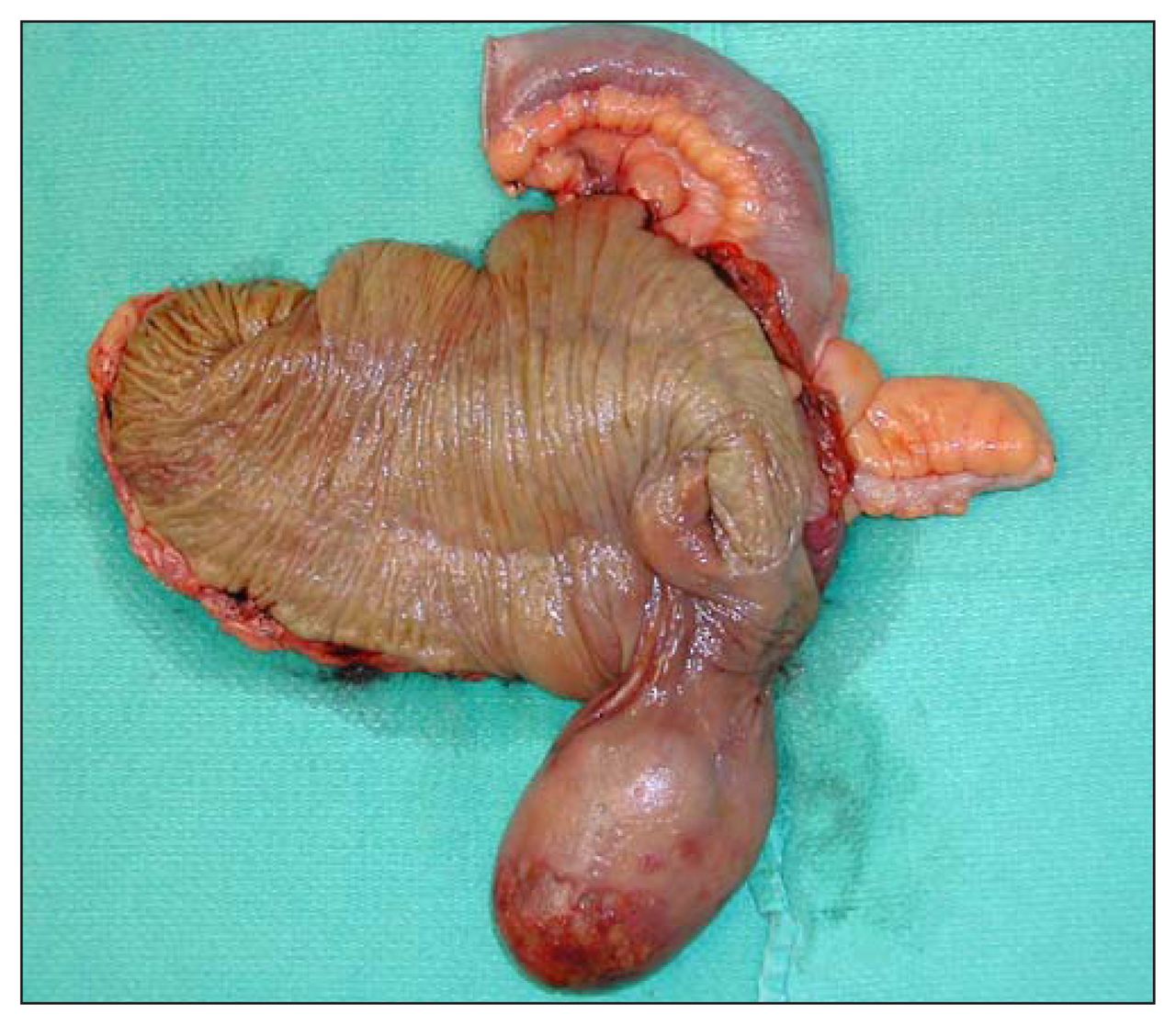
A submucosal pedunculated lesion is seen in the proximal cecum.

{kind=link}
{kind=link}
{kind=link}
Pathological examination of the resected mass revealed a lipoma.
Discussion
Because it is relatively rare in adults, intussusception is seldom diagnosed by clinical findings alone. Intussusception can be confidently diagnosed on CT because of its virtually pathognomonic appearance.2 On CT, intussusception appears as a “sausage-shaped” mass in the longitudinal axis, and as a “target” mass in the transverse axis. More than 90% of intussusceptions in adults have a demonstrable cause, 60% due to neoplasm (60% malignant, 40% benign).3 The high rate of pathologic lead points, along with the high rate of malignancy, makes surgery mandatory in these cases.4 However, there is much debate as to whether resection should be performed with or without prior reduction. The most widely accepted view is that in most cases of ileocolic and colocolic intussusception, the procedure should be primary resection without reduction because of the high risk of underlying malignant disease. In patients with enteroenteric intussusception, reduction should be attempted initially, provided there is no sign of inflammation or bowel ischemia and a malignant lesion is not suspected.3
Footnotes
Competing interests: None declared.
- Accepted February 20, 2006.