

Abstract
Background: Point of injury needle thoracostomy (NT) for tension pneumothorax is potentially lifesaving. Recent data raised concerns regarding the efficacy of conventional NT devices. Owing to these considerations, the Israeli Defense Forces Medical Corps (IDF-MC) recently introduced a longer, wider, more durable catheter for the performance of rapid chest decompression. The present series represents the IDF-MC experience with chest decompression by NT.
Methods: We reviewed the IDF trauma registry from January 1997 to October 2012 to identify all cases in which NT was attempted.
Results: During the study period a total of 111 patients underwent chest decompression by NT. Most casualties (54%) were wounded as a result of gunshot wounds (GSW); motor vehicle accidents (MVAs) were the second leading cause (16%). Most (79%) NTs were performed at the point of injury, while the rest were performed during evacuation by ambulance or helicopter (13% and 4%, respectively). Decreased breath sounds on the affected side were one of the most frequent clinical indications for NT, recorded in 28% of cases. Decreased breath sounds were more common in surviving than in nonsurviving patients. (37% v. 19%, p < 0.001). A chest tube was installed on the field in 35 patients (32%), all after NT.
Conclusion: Standard NT has a high failure rate on the battlefield. Alternative measures for chest decompression, such as the Vygon catheter, appear to be a feasible alternative to conventional NT.
Tension pneumothorax (TPTX) is a life-threatening condition and the third most frequent cause of preventable deaths on the battlefield.1 Autopsy studies from the Vietnam War suggested that TPTX led to 3%–5% of all potentially preventable deaths.2 The clinical definition of TPTX is a PTX that results in hemodynamic compromise, as the increased intrathoracic pressure interferes with the venous return to the right atrium. Viewed on chest imaging, lateral shift of the mediastinum concurrent with respiratory distress (or difficult ventilation) and/or hypotension is considered the hallmark of TPTX,3,4 even though obtaining a chest radiograph for suspected tension TPTX is considered an unjustified delay. The Advanced Trauma Life Support (ATLS) guideline proposed by the American College of Surgeons recommends that the diagnosis be made based only on clinical grounds. Tension PTX is caused by the progressive buildup of air within the pleural space, and positive pressure ventilation may accelerate this process, which may result in traumatic arrest. The ATLS recommends that needle thoracostomy should be performed at the second intercostal space (ICS) in the midclavicular line using a catheter more than 5 cm long.5
While the urgent evacuation of a patient with PTX is a component of all emergency medical algorithms,5 controversy remains regarding the optimal timing and means of treatment prior to evacuation. Some consider needle decompression (also called needle thoracostomy [NT]) as a temporary means for pressure release and bridging therapy until the insertion of a tube thoracostomy (TT). Others suggest that NT can sometimes be definitive therapy, and that not every NT should be followed by a TT insertion. Finally, some suggest TT, rather than NT, as the primary therapy.4,6,7 The reported success rates and the level of training required for these procedures vary.8
Prehospital NT can be life-saving, but technical aspects of the procedure have given rise to a discussion of whether it should be considered only a temporary measure. Investigators have reported chest wall thickness to be a key factor accounting for failures to successfully evacuate the chest, and therefore recommend the use of longer needles. Stevens and colleagues9 retrospectively examined thoracic computed tomography (CT) studies and determined the chest wall thickness at the midclavicular line to be 41–45 mm compared to the 14-gauge angiocatheter length of 4.5 cm. They concluded that the standard angiocatheter was likely to be unsuccessful in 50% of trauma patients on the basis of body habitus alone.
Similar findings were reported raising the same concerns.10–12 In other reports, techniques such as cadaver dissection13,14 and ultrasonography15,16 were used to detect the penetration of catheters. On the basis of these findings, a recommendation for change was issued, and many prehospital organizations have adopted the use of longer catheters. Tactical Combat Casualty Care (TCCC) guidelines recommend “decompress[ing] the chest on the side of the injury with a 14-gauge, 3.25 inch (8.25 cm) needle/catheter.”17,18
The catheter’s diameter is another concern. Martin and colleagues19 used a porcine model to show that the decompression of the chest by a 14-gauge needle should not be expected to result in relief of tension physiology, as a substantial air leak necessary to cause TPX physiology cannot be effectively drained with a 14-gauge tube.
The preferred NT insertion site itself is subject to debate, with evidence suggesting that the fourth and fifth ICS (at the anterior axillary line, similar to the recommended TT insertion site) may be superior to the classic site (the midclavicular line).12,14 Others raised concerns regarding the function of the NT inserted in this site, and both insertion site options are currently considered valid.4
Despite these and other concerns, the current recommended needle used for decompression is a 14-gauge angiocatheter.5
Owing to these considerations, along with concerns regarding catheter kinking20 and blockage, in 2006 the Israeli Defense Forces Medical Corps (IDF-MC) introduced a thicker, longer catheter for the performance of rapid chest decompression.
We report our experience with NT and preliminary data on our use of a 10-French Vygon TT unit (thoracic trocar and drain; Vygon), instead of the traditional 14-gauge angiocatheter, as the preferred means for rapid chest decompression.
Methods
The IDF clinical practice guidelines for thoracic injury
The IDF-MC clinical practice guidelines (CPGs) concerning thoracic injury advocate a high index of suspicion for TPTX in patients with thoracic injuries. Casualties sustaining a penetrating injury to the thorax presenting with severe dyspnea, decreased oxygen saturation or hemodynamic compromise should undergo chest decompression. Initial decompression is performed by NT; a TT is installed if initial NT fails to improve the patient’s hemodynamic status or oxygen saturation. A TT should also be installed following NT when casualty evacuation time to the next echelon of care is expected to exceed 45 minutes (Fig. 1). While the TCCC guidelines instruct the sealing of chest wounds using a vented chest seal,21 the IDF CPGs on the management of thoracic injuries instruct thoracic decompression as the mainstay of therapy for any casualty with a thoracic injury prior to sealing the wound.

Vygon tube thoracostomy unit (thoracic trocar and 10-French drain) for pleural drainage in neonates.
Needle decompression in the IDF
From 1997 to 2007, a 14-gauge angiocatheter inserted into the second ICS in the midclavicular line was the method of choice for NT. In 2007, the IDF-MC introduced the pediatric Vygon TT unit to be used for NT in adults (Fig. 2). The device consists of a10-French drain made of transparent polyvinyl chloride with X.R.O. line, 1 lateral eye and markings at every centimetre. The tube is 8 cm long with a proximal female Luer-lock connector.

Algorithm for the treatment of chest injuries on the battlefield according to Israeli Defense Forces Medical Corps clinical practice guidelines. ALS = advanced life support; TT = tube thoracostomy.
The procedure is performed preferably under aseptic conditions using a suitable skin disinfectant. Using a No. 11 blade, a small incision is made through the skin, subcutaneous tissue and muscle. The tube and the drain are inserted bluntly and perpendicularly through the anterior chest wall at the second ICS in the midclavicular line, penetrating the pleural cavity to relieve the TPTX. The trocar is removed and the tube is firmly attached to the chest by means of adhesive tape.
Study population
The IDF trauma registry is a prehospital military trauma registry containing data on trauma casualties (civilian or military) cared for by military medical teams. Data are collected in the form of casualty cards. Casualty cards are followed by a more comprehensive after action medical debriefing. Hospital data are collected directly from treating hospitals’ medical charts. All available information is being integrated to the ITR at the Combat and Trauma Medicine Branch at the Surgeon General’s headquarters.
We searched through the registry for records from January 1997 to October 2012 to identify all patients in whom NT was attempted. We collected data on patient demographic characteristics, type of injury, vital signs, life-saving procedures, number of NT attempts, success of NT (subjective improvement after NT was recorded, yes v. no), TT insertion, identity of caregiver, survival, iatrogenic injuries and complications. Predefined signs and symptoms of PTX were extracted from charts and assigned as NT clinical indications.
Statistical analysis
Data were entered into a Microsoft Excel spreadsheet and analyzed using JMP statistical software. We obtained descriptive statistics for all variables. Continuous variables are presented as means ± standard deviations with 95% confidence intervals (CI). Categorical variables are presented as numbers and percentages where appropriate. We compared categorical variables using the Fisher exact test, and continuous variables were compared using the Wilcoxon rank-sum test.
Results
During the study period, 4621 patients were recorded in the IDF-MC database. A total of 111 (2.5%) of these patients underwent NT as part of their treatment, making up the study group. Seventeen (15%) patients underwent bilateral decompression, and 26 (23%) required multiple NT attempts on a single hemithorax. Thirty-five (32%) patients had a chest tube placed in the field, all following NT attempts.
The patients’ mean age was 21 (range 20–25.5) years. Most (101 of 111, 91%) patients were men.
Eighty-seven (78%) patients sustained penetrating injuries, 21 (19%) were victims of blunt trauma, and in the remaining 3 (3%) patients the mechanism of injury was not specified. Eighty (72%) patients received medical care in an austere environment or under threat, while 31 (28%) patients received care in a safe setting.
Most (54%) casualties were wounded as a result of gunshot wounds (GSW); motor vehicle accidents (MVA) were the second leading cause (16%), and blast injuries caused by improvised explosive devices (IED) were the third most frequent cause (13%; Table 1).
Mechanisms of injury
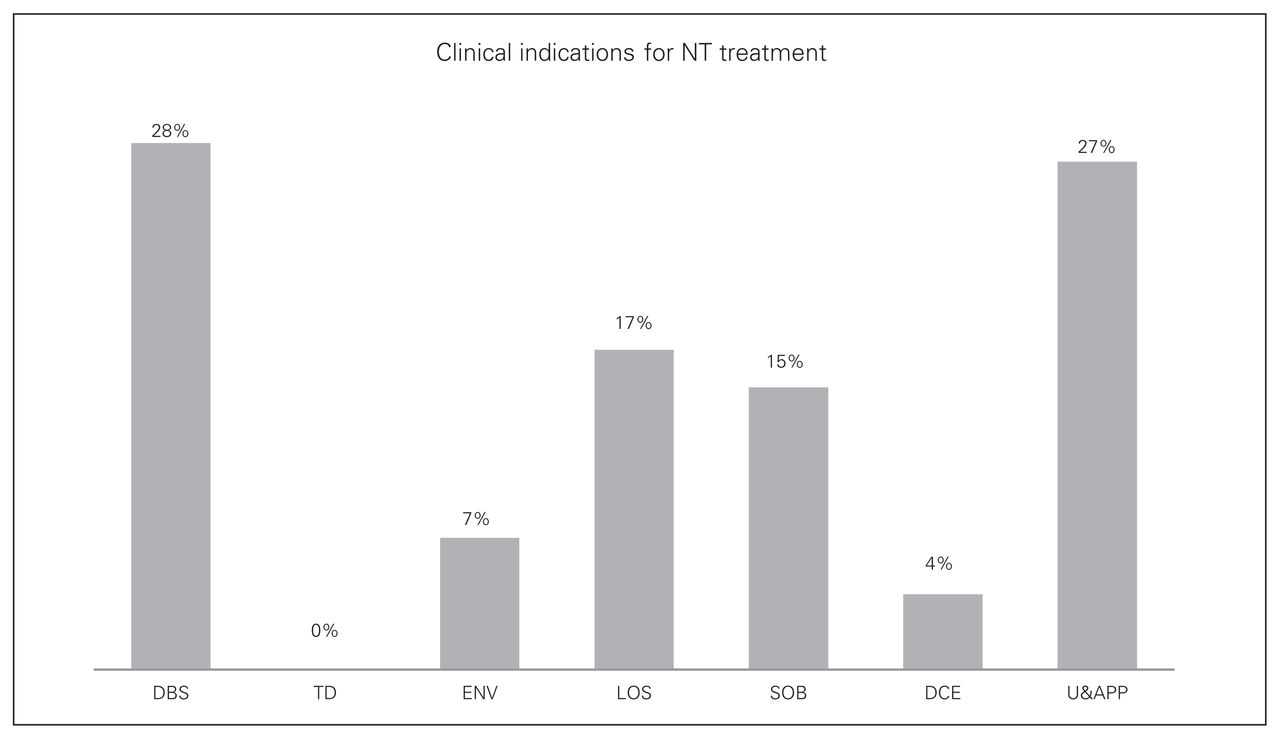
The clinical indications for NT are shown in Figure 3. Decreased breath sounds on the affected side were one of the most frequent clinical indications for NT, occurring in 28% of all cases. Decreased breath sound was more common in surviving than in nonsurviving patients. (37% v. 19%, p < 0.001). Nonresponsiveness and absent peripheral pulses had similar overall frequency to decreased breath sounds; however, these features were more common in nonsurviving than surviving patients (47% v. 6%, p < 0.001). Shortness of breath was present in 15% of patients, while low oxygen saturation was observed in 17%.

Percentage of cases in which each clinical indication was used by flight surgeons to determine neddle decompression (NT) or tube thoracostomy treatment. Specific indications include decreased breath sounds (DBS) on 1 side, tracheal deviation (TD), engorged neck veins (ENV), low oxygen saturation (LOS), shortness of breath (SOB), decreased chest expansion (DCE) and unconsciousness and absent peripheral pulse (U&APP).
Engorged neck veins and limited chest expansion were observed in only a minority (7%) of patients, and tracheal deviation was not reported.
The care providers reported a subjective improvement in patient respiratory function following NT in 83% of the surviving patients and in 86% of the nonsurviving patients. Unfortunately no further specification was available.
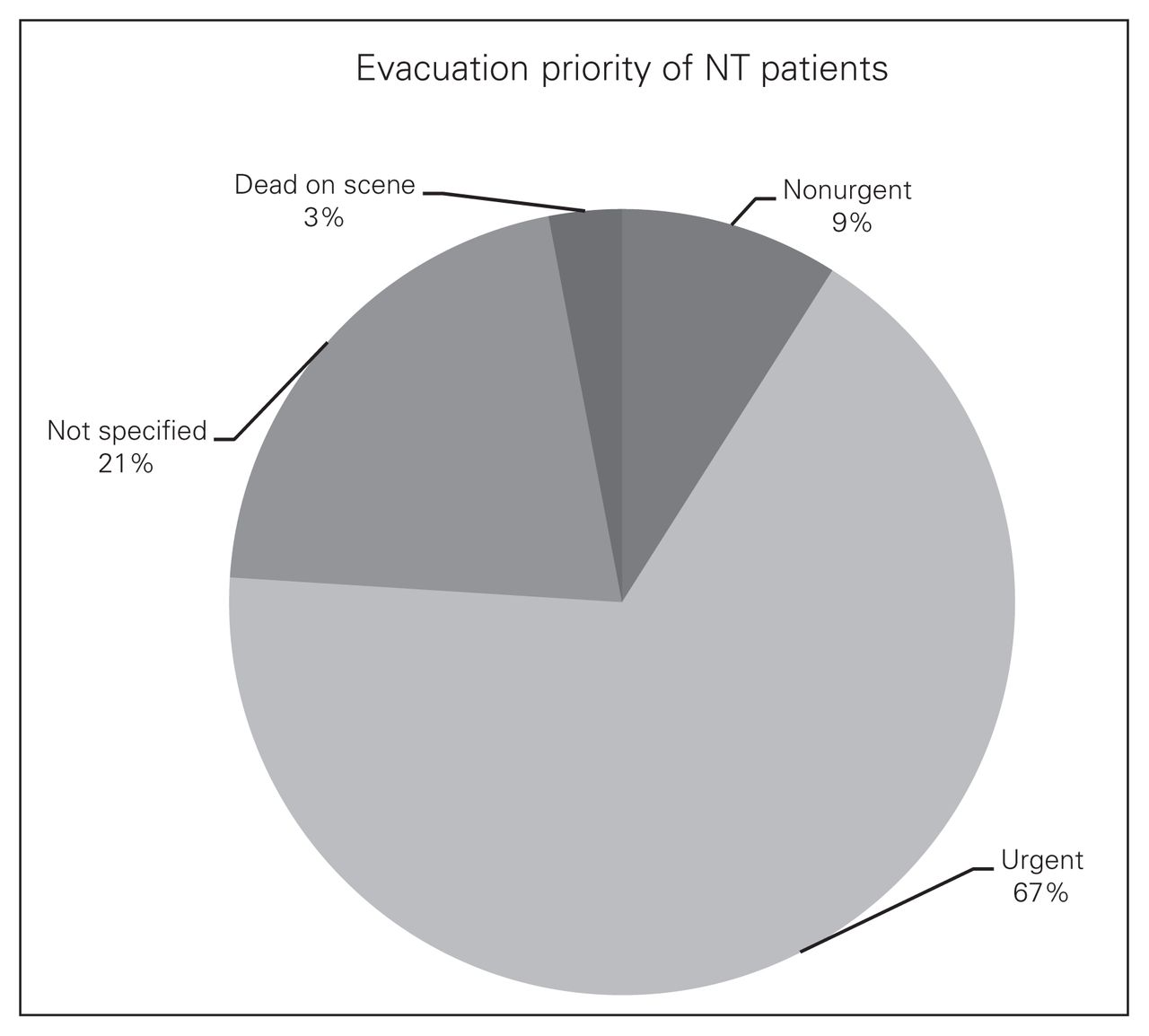
The mean ISS was 31 ± 24.6, which indicates a cohort of severely injured patients undergoing NT. Seventy-four (67%) patients were classified as urgent for evacuation by the medical provider at the point of injury, and only 10 (9%) patients were classified as nonurgent (Fig. 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Evacuation priority of needle decompression (NT) patients.
The overall mortality was 51%. Twenty-three (21%) casualties were defined as killed in action (KIA), and 7 (6%) were pronounced dead on arrival at the trauma centre. None of the KIA patients had a return of spontaneous circulation in the field. Twenty-one (19%) patients died from their wounds after hospital admission.22
Chest decompression was often performed rapidly in a complex resuscitation environment with patients undergoing multiple concurrent interventional procedures. Other life-saving procedures performed on this study population were endotracheal intubation (48%), cricothyroidectomy (9%) and tourniquet application (6%). Twenty-six (23%) patients did not receive additional advanced live-saving procedures.
Prehospital NT was performed by military physicians in 44% of patients, by military paramedics in 9% and by civilian emergency medical services (EMS) paramedics in conjunction with military medical teams (to soldiers and civilians injured in areas with civilian EMS availability) in 12%. Unfortunately, the care providers’ identities were not recorded in 39 (35%) cases. Subjective patient improvement was reported by military physicians in 41 (84%) casualties, by military paramedics in 9 (90%) and by civilian EMS paramedics in 11 (85%). Despite the impressive clinical improvement, mortality remained surprisingly high in the military physicians’ and military paramedics’ groups: 55% and 90%, respectively. The lowest mortality (23%) was found in the civilian EMS paramedics’ group (p = 0.007).
The catheter used for NT was a 14-gauge angiocatheter in 88 (79%) patients and a Vygon TT unit in 6 (5%) casualties, all of whom were treated after 2007. For 16 (15%) patients the documentation did not mention which type of device was chosen, and in 1 (1%) patient both devices were used owing to suspected failure of the 14-gauge angiocatheter.
Most (79%) cases of NT were performed at the point of injury, and the rest were performed during transportation on ambulance or helicopter (13% and 4% of the patients, respectively). In 4 (4%) patients the location of chest decompression was not specified.
No iatrogenic injuries or complications due to prehospital NT were reported.
Discussion
Classic hallmarks of TPTX include a variety of signs and symptoms, the majority of which are nonsensitive and nonspecific.5 An analysis designed to assess the clinical presentation guiding the decision to perform chest decompression in our study population revealed decreased breath sound, absent radial pulses and a low GCS to be the most common presentations. Unsurprisingly, decreased breath sounds as a clinical presentation of TPTX was more common in patients who survived their injuries than in patients who did not, whereas depressed GCS (nonresponsiveness) and absent radial pulses (both clinical indicators for decreased blood perfusion) were more common in patients who died following their injuries. This finding is probably indicative of the more deranged physiology associated with a PTX that resulted in hemodynamic compromise. Tracheal deviation was not detected in any of the casualties in this series, whereas dilated neck veins were reported in only 7% of casualties. These 2 symptoms, which were once considered hallmarks of TPTX, are no longer considered necessary for diagnosis as they appear infrequently in patients with TPTX and accordingly were not used to instruct chest decompression in our series. Decreased level of consciousness and hypotension as well as decreased oxygen saturation, the second and third most prevalent indicators for chest decompression in this series, are considered inconsistent or even rare signs of TPTX23 and are thus less useful for its diagnosis. However, as our series included a subset of patients who required prehospital decompression of TPTX, these findings, suggestive of a significant disturbed physiology, were more frequent than other symptoms indicating chest decompression. This finding is consistent with the IDF-MC CPGs for thoracic injuries that instruct NT or CD in casualties with thoracic injuries who present with hemodynamic compromise or decreased oxygen saturation.
Current CPGs use a wide variety of indications for NT, which inevitably results in chest decompression performed on patients who do not necessarily have TPTX. While the presented data support the possibility to narrow the spectrum of signs and symptoms used to diagnose TPTX, the IDF CPGs were not altered owing to the assumption that overdiagnosis and treatment of TPTX is preferable to underdiagnosis.
A mean ISS of 31 in the present series suggests a cohort of severely injured patients. This is unsurprising considering the relatively high rate of GSW-related injuries, specifically when considering that in a military population the majority of GSWs are the result of high-velocity weapons. Postmortem examinations in Israel are rarely performed, mainly because of religious considerations; it is therefore difficult to determine cause of death. However, considering the high mean ISS and the fact that in 77% of patients NT was not the only life-saving intervention performed, it is reasonable to assume that injuries other than TPTX contributed substantially to the high mortality.
Despite a substantial failure rate,7,24–26 NT can relieve intrapleural pressure and rapidly change a tension to a simple PTX, allowing time to prepare for TT.
In Israel, NT is the only procedure that EMS paramedics are allowed to perform in the civilian environment to treat a suspected TPTX. However, military paramedics are trained and authorized to insert a CD, according to physician instruction, following an unsuccessful NT.
In the present series, medical providers reported a clinical improvement in the patient respiratory status following NT in 83% of surviving patients and in 86% of the patients who eventually died from their injuries. This clinical success rate seems exceptionally high considering evidence suggesting that NT may fail to decompress TPTX in up to 50% of patients.9–12, 27 Furthermore, because a similar rate of clinical improvement was reported in patients surviving their injuries as in patients who did not survive, it seems that these high success rates are the result of inaccurate subjective assessment. In the present study, 32% of patients undergoing NT eventually had a CD installed in the prehospital setting, implying a true failure rate more consistent with that reported in the available literature.
While literature review revealed that major complications (hemorrhage and cardiac injuries) occur, no major complications as a result of NT were reported in our series.28,29 However, as the majority of trauma victims in the IDF do not undergo postmortem examination, this may be the result of undiagnosed complications and could also have been a result of the retrospective limitation of this report.
Some authors now advocate that longer catheters should be used for NT, particularly in a military context,30–32 but occlusion by blood or tissue and slippage out of the chest wall remain important concerns.33 Jones and Hollingsworth34 described 3 cases suggesting angiocatheter failure attributed to kinking and proposed the use of a blunt-ended rigid device designed to treat TPTX. The catheter chosen by the IDF-MC to serve as the NT is a 10-French TT. The use of small-calibre chest tubes in the treatment of adult PTX was first described by Sargent and Turner.35 They used a 9-French (rather than the usual 32-French) catheter in combination with a Heimlich valve, which was simple to insert. Several subsequent series reported the use of a 9-French catheter for the treatment of PTX, most frequently postlung biopsy. These series report high success rates of 87%–95%.36–38
The present series represents a transition in the device used to alleviate TPTX in the IDF, and while it is a preliminary report that was not designed to assess outcomes, initial experience suggest the feasibility of this method.
Limitations
This study has several limitations. It was a small study with no formal sample size calculation. Data were collected retrospectively, resulting in incomplete data collection. Several end points were subjective, potentially resulting in reporting biases. Barton and colleagues24 reported that medical personnel may have documented the release of air or improved compliance to justify the use of NT; however, these are difficult to verify and may be influenced by wishful thinking. Finally, the study was performed in only a military environment in Israel. This population may not be representative of other trauma systems.
Conclusion
We have described our experience with standard NT and our preliminary results using Vygon TT in patients with suspected TPTX. Standard NT has many limitations, while NT using a Vygon catheter offers a potentially safe and reasonable alternative. It does not require advanced surgical skill or training and can be inserted efficiently and safely by ATLS providers. This device should become an accepted part of the military emergency care tool kit. Further prospective studies should be performed to substantiate the efficacy and theoretical advantages of the Vygon TT unit over a 14-gauge angiocatheter.
Footnotes
Competing interests: None declared.
Contributors: J. Chen designed the study. J. Chen and R. Nadler acquired the data, which all authors analyzed. J. Chen, A. Cap and E. Glassberg wrote the article, which all authors reviewed and approved for publication.
- Accepted November 12, 2014.