

Abstract
Background: Rates of surgical management of distal radius fractures are increasing internationally despite the higher cost and limited outcome evidence to support this shift. This study examines the epidemiology of distal radius fractures and asks if the same shift has occurred in Ontario, Canada (population 13.9 million).
Methods: This population-based, retrospective cohort study examined distal radius fractures in people aged 18 years and older over a 10-year period (2004–2013). The incidence analyses were based on the first occurrence of a fracture within a 2-year time period. The number of fractures, age-adjusted incidence rates and frequency of fracture treatment type by year were assessed. We used a Poisson regression with robust standard errors to determine if there was a statistically significant change in the frequency of fracture treatment type over time.
Results: There were 25 355 distal radius fractures among Ontarians 18 years of age and older in 2013. Between 2004 and 2013, the age-adjusted incidence rate for people 35 years of age and older was stable, between 2.32 and 2.70 per 1000 population. Rates of cast immobilization remained stable between 82% and 84%. Of those patients treated surgically, the rate of open reduction and internal fixation rose from 7% in 2004 to 13% in 2013 at the expense of other types of surgical management.
Conclusion: In Ontario, rates of cast immobilization are stable and there has been a movement toward open reduction and internal fixation among patients treated surgically.
The distal radius is the most common fracture site encountered by physicians.1,2 It accounts for up to 20% of all fractures treated in the emergency department. Fractures of the distal radius are most common in women and the elderly. Proper management requires accurate fracture assessment, diagnosis, treatment and evaluation of outcomes.3 The most common form of treatment is closed reduction and cast immobilization. Typically, surgical management is reserved for displaced fractures that cannot be adequately reduced and immobilized. This decision is based on parameters such as the degree of postreduction radial shortening, dorsal tilt and/ or intraarticular displacement or step-off.4 There are often multiple acceptable treatment approaches to the same fracture pattern, including surgical and nonsurgical ones.5 In recent years, there has been a rise in the rate of surgical management in the United States. Chung and colleagues found that open reduction and internal fixation (ORIF) of the distal radius increased from 3% to 16% in the United States between 1996 and 2005.6 Concurrently, nonsurgical management decreased from 82% in 1996 to 70% in 2005. This change in treatment has been seen in other countries, such as Sweden and Finland, which have a single-payer model similar to Canada.7–9 We anticipated that Ontario would have a stable or modestly declining rate of nonsurgical management as surgeons at our institution have not perceived a large change in clinical management.
The central aim of this study was to understand the epidemiology of fracture care in Ontario using population-level data. We investigated whether Ontario has experienced the increase in rates of surgical management of distal radius fractures seen in other countries. We delved deeper to see if treatment varies by patient age or region in Ontario.
There are obvious cost implications of this change in management, and there is little evidence to support a shift to surgical management.10 In 2007, the mean payment per Medicare beneficiary for ORIF was more than double that for cast immobilization (US$3832 v. US$1459, respectively). 11 Multiple systematic reviews, meta-analyses and prospective studies with various patient populations all indicate equivalent functional outcomes for the 4 most common methods of treatment: cast immobilization, percutaneous pinning with cast immobilization, external fixation and ORIF.1,12–15
Methods
We conducted a population-based, retrospective cohort study examining distal radius fractures over a 10-year period. It included all people aged 18 years and older covered under the Ontario Health Insurance Plan (OHIP) between 2004 and 2013. This study was approved by the University of Toronto’s research ethics board.
Data sources
We used (a) the Registered Persons Database (RPDB), which contains demographic information on everyone who has received a health service in Ontario; (b) OHIP, which provides details on medical services billed by Ontario physicians; and (c) ICES’ Physician Database (IPDB), which contains information on physicians’ demographics, specialty training and certification and practice location. We obtained access to these databases through ICES, and data sets were linked using patient-specific encrypted identifiers.
Identification of distal radius fracture
Ontarians aged 18 years and older with a distal radius fracture between 2004 and 2013 were identified from OHIP billing codes. They were categorized by primary treatment modality, as having received (a) cast immobilization only, (b) percutaneous pinning with cast immobilization, (c) external fixation or (d) ORIF (Appendix 1, available at canjsurg.ca/016218-a1). If a patient received 2 or more treatment modalities within a 3-week period, the primary treatment modality was categorized as the most invasive treatment (where cast immobilization < percutaneous pinning with cast immobilization < external fixation < ORIF) (see Appendix 1). With our reliance on billing codes we risked counting reoperations as a new index event (i.e., double counting). Therefore, we defined a new event in a patient only if it occurred more than 2 years after any initial treatment modality. This was a conservative decision based on reoperation data.16 This also meant that in patients with bilateral fractures, only the first documented fracture was counted.
Treating physician
The treating physician was defined as the person who billed for the OHIP treatment code. However, if a patient in the group that received only cast immobilization was referred to an orthopedic surgeon or plastic surgeon and seen within 3 weeks, then this surgeon was defined as the treating physician.
Geography
The unit of analysis was the local health integration network (LHIN). The RPDB links patients to a specific LHIN. The IPDB links a physician’s practice to a specific LHIN.
Statistical analysis
We determined the number of fractures among patients aged 18 years and older. We calculated the age-adjusted incidence rate for men and women 35 years of age and older as this allowed us to compare our results with those of other studies that have previously reported data from other countries and cities in this format.17 We used 2006 as the standard population for this calculation and calculated 95% confidence intervals [CIs]. We determined the frequency of fracture treatment type by year among people aged 18 years and older. We used a Poisson regression with robust standard errors18 to determine if there was a statistically significant change in the frequency of fracture treatment type over time. A p value less than 0.05 was deemed significant. The goodness of fit was confirmed with a χ2 test. We evaluated the 2013 data in more detail by calculating the frequency of fracture treatment type by age and LHIN.19
Results
The number of distal radius fractures for patients aged 18 years and older was 25 355 in 2013. The age- and sexadjusted yearly incidence rates for patients aged 35 years and older remained between 2.32 and 2.70 per 1000 population over the 10-year study period (Fig. 1). The male and female age-adjusted incidence rates for people 35 years of age and older were also stable; they remained between 1.45 and 1.64 per 1000 population and between 3.04 and 3.45 per 1000 population, respectively (Fig. 1 and Table 1).
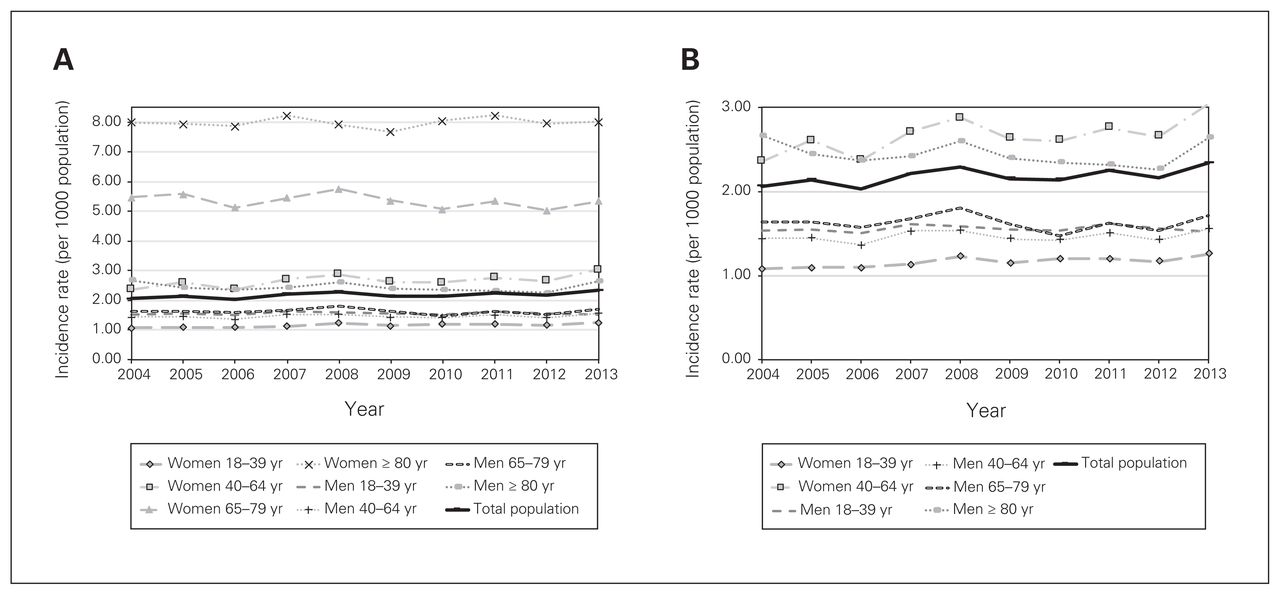
Incidence rates of distal radius fractures in Ontario (2004–2013) (A) for all groups and (B) taking a closer look at the groups with rates between 0 and 3.00 per 1000 population. Note that crude incidence rates are provided for each age–sex group. The total population was age- and sex-adjusted for patients 35 years of age and older to allow for comparison with previously reported data from other jurisdictions.
Standardized incidence rate per 1000 population for patients aged 35 years and older, using 2006 as the standard population
Sixty-seven percent (16 881 of 25 355 patients in 2013) of all fractures in patients 18 years of age and older occurred in women. Women aged 50–64 years represented the largest subgroup (22% of all distal radius fractures). There was a relatively stable incidence rate for men for each age category until age 80; the incident rate increased for male patients aged age 80 years and older. Women experienced a steady increase in fracture rate with age; the highest incidence rate in women aged 80 years and older (8.02 per 1000 population) was much higher than for men in this age group (Fig. 1).
Rates of cast immobilization remained stable between 82% (18 222/22 192) and 84% (21 330/25 355) over the 10-year study period. There was a statistically significant increase in the rate of ORIF, from 7% (1407/19 792) in 2004 to 13% (3184/25 355) in 2013 (incidence rate ratio [IRR] 1.07, 95% CI 1.06–1.08) (Fig. 2 and Appendix 1). Simultaneously, there was a reduction in the proportion of distal radius fractures treated with percutaneous pinning with cast immobilization and external fixation from 6.1% and 3.3% in 2004 to 2.2% and 1.1% in 2013, respectively (Fig. 2 and Appendix 1). These were statistically significant decreases (percutaneous pinning with cast immobilization: IRR 0.90, 95% CI 0.89–0.92; external fixation: IRR 0.82, CI 95% 0.79–0.84). There was some variation by age group, with men and women 80 years of age and older having the highest frequency of cast immobilization (95% [529/559] and 91% [2499/2751], respectively) (Fig. 3).

Treatment of distal radius fractures among Ontarians 18 years of age and older (2004–2013).

Variation in patterns of treatment for distal radius fracture by patient age in 2013. CI = cast immobilization, EF = external fixation, ORIF = open reduction and internal fixation, PP + CI = percutaneous pinning with cast immobilization.
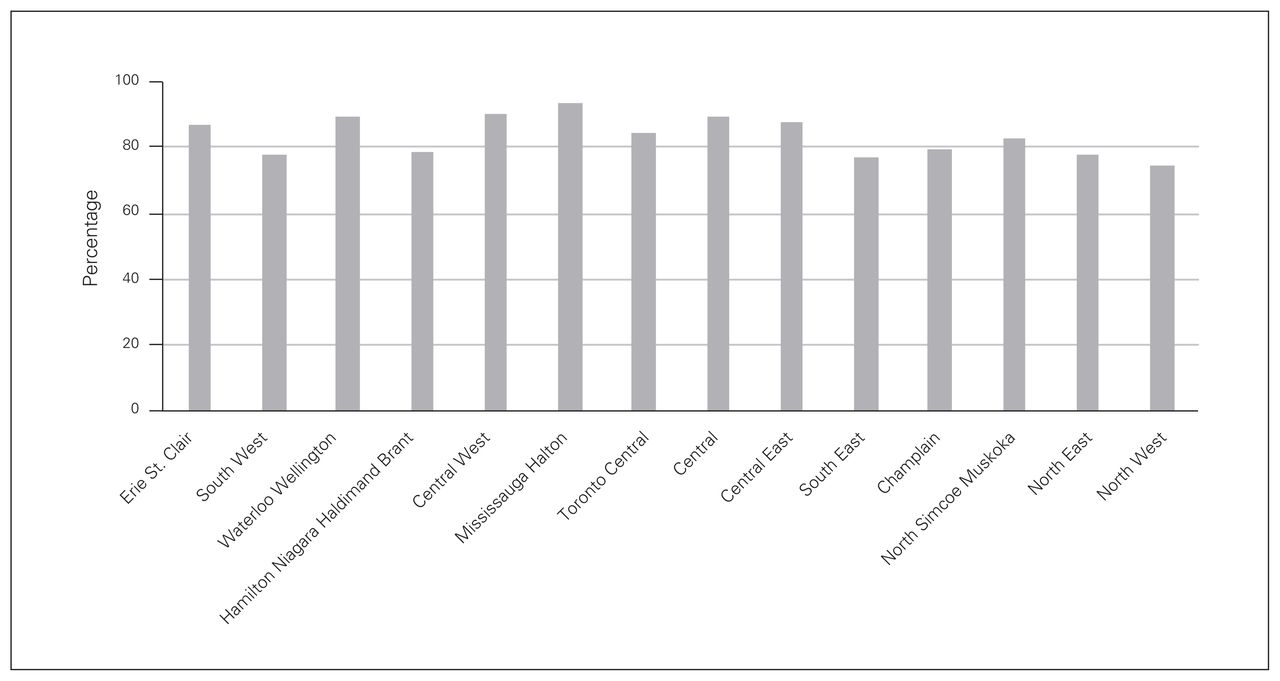
In 2013, most (22 549/25 355) distal radius fractures were managed by an orthopedic surgeon. A small subgroup was managed by plastic surgeons (2.4%, n = 597) and physicians in nonsurgical specialties (8.3%, n = 2102), namely family physicians and emergency physicians. Eighty percent of Ontarians (20 198/25 201) had their distal radius fracture treated locally (i.e., in their local LHIN). One LHIN (Toronto Central) treated substantially treated substantially more of the study patients than their share of the Ontario population (144%), and their rates of cast immobilization and ORIF were 84% (3426/4062) and 13% (539/4062), respectively, in 2013. Rates of cast immobization varied from 74% to 93% by region in 2013 (Fig. 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rate of cast immobilization by local health integration network in 2013.
Discussion
Ontario has a population of 13.9 million, representing almost 40% of the entire Canadian population. Between 2004 and 2013, the age- and sex-adjusted incidence rate of distal radius fractures was stable. The rates of cast immobilization remained stable between 82% and 84% over the 10-year period. The rates of surgical management were stable but fractures were more frequently managed with ORIF (from 7% in 2004 to 13% in 2013) than with percutaneous pinning with cast immobilization or external fixation.
Jaglal and colleagues reported that age-adjusted incidence rates were on the decline because of osteoporosis prevention efforts.20 They found that between 1992 and 2002, in the context of a growing population, the number of distal radius fractures was fairly constant.20 Our study shows that the age-adjusted incidence rates for men and women 35 years of age and older are stable and the overall number of distal radius fractures per year has grown in accordance with population growth. It is possible that any earlier gains from osteoporosis prevention efforts have now levelled off.
Ontario has maintained a stable rate of cast immobilization as treatment for distal radius fractures. This is in contrast to the United States Medicare population, where only 70% of patients aged 65 years and older were treated with cast immobilization in 2005,21 and a recent Swedish study, where only 73% of patients aged 18 years and older were treated with cast immobilization in 2010.9 Canada has moved toward ORIF management of those fractures treated surgically, so much so that the rates of ORIF management are similar among these 3 countries (Table 2). However, the United States and Sweden have not abandoned percutaneous pinning with cast immobilization and external fixation to the same degree as Canada, which explains the overall higher rate of surgical management and lower rate of nonsurgical management in those countries (Table 2). Multiple recent systematic reviews and metaanalyses comparing the 4 most common methods of treatment (cast immobilization, percutaneous pinning with cast immobilization, external fixation and ORIF) have found equivalent functional outcomes in patients aged 45 years and older14 and aged 60 years and older.1,15 Similarly, a prospective randomized trial found equivalent functional outcomes for cast immobilization and ORIF in patients aged 65 years and older with a displaced intraarticular distal radius fracture.22 In a younger cohort of 3666 patients aged 18 years and older, 1-year Disabilities of the Arm, Shoulder and Hand (DASH) scores were equivalent among those treated surgically and nonsurgically.12 It is also known that surgical management carries a higher risk of surgery-related complications23 and higher costs for the health care system24 than nonsurgical cast immobilization.
Frequency of cast immobilization and ORIF management in Canada, Sweden and the United States
In Ontario, there is much less regional variation in treatment than in the United States.25 According to Medicare data in the United States, regional variation in ORIF management ranged from 4.6% to 42.1% and correlated with access to a designated hand surgeon.25 Designated hand surgeons would probably receive more complex referrals and therefore operate more. Similarly, we expected that regions in Ontario receiving higher numbers of referrals to treat out-of-region patients would treat more complex fractures and have higher rates of ORIF; however, this did not prove to be the case. Toronto Central is the highest referral region in Ontario, and its rate of ORIF was only 13% in 2013. The rate of cast immobilization was 84% in 2013. Variations between regions may reflect variations in the population, fracture severity and/or access.
Limitations
The limitations of this study include our inability to differentiate between fracture severity and the type of treatment the patient receives. There may be international variations in fracture pattern over time that warrant a higher use of ORIF in the United States or Sweden. Of those patients who received ORIF, we do not know what type of approach (volar v. dorsal) or plate (locking v. nonlocking) was used as the fee code only denotes “open reduction and internal fixation.” From the IPDB we cannot discern if an orthopedic or plastic surgeon specializes in hand surgery as there is no capacity to designate subspecialization as there is in the United States Medicare system.25
Conclusion
Ontario has experienced relatively constant rates (82% to 84%) of cast immobilization as treatment for distal radius fractures. For those fractures treated surgically in Ontario, there has been a movement away from both percutaneous pinning with cast immobilization and external fixation in strong favour of ORIF. This demonstrates that the increase in surgical management has not been universal, and it is difficult to justify because of the increased cost and lack of strong outcome evidence to support this trend.
Footnotes
A portion of this paper was presented at the American Association for Hand Surgery Annual Meeting, Jan. 13–16, 2016, Scottsdale, Ariz.
Funding: Funding was provided by the Physicians’ Services Incorporated Foundation for the collection and management of the data.
Competing interests: None declared.
Contributors: K. Armstrong, H. von Schroeder, N. Baxter, T. Zhong and S. McCabe designed the study. K. Armstrong, N. Baxter, T. Zhong, A. Huang and S. McCabe acquired and analyzed the data and H. von Schroeder also analyzed the data. K. Armstrong wrote the article, which all authors reviewed and approved for publication. All authors agreed to be accountable for all aspects of the work.
- Received September 23, 2019.
- Accepted January 9, 2019.