

Abstract
Background Recent evidence suggests that home care nursing is variably prescribed after vascular surgery, and may reduce emergency department visits and hospital readmissions. We therefore sought to characterize the indications for home care nursing following vascular surgery from the surgeon’s perspective.
Methods An online survey was distributed to the 141 members of the Canadian Society for Vascular Surgery with questions related to home care nursing after carotid endarterectomy (CEA), endovascular aortic aneurysm repair (EVAR), open abdominal aortic aneurysm (AAA) repair and open or hybrid revascularization for peripheral arterial disease (PAD). We included all questionnaires in our analysis; the frequency denominator changes according to the number of respondents who completed each survey item.
Results There were 46 survey respondents (33% of 141) from across the country. A total of 28 (62% of 45) worked in a teaching hospital. Home care nursing was routinely prescribed by 5%, 10%, 31% and 41% of respondents following CEA, EVAR, open AAA repair and open or hybrid revascularization for PAD, respectively. Across all procedure types, the same procedure-related criteria were most often deemed to warrant a prescription for home care nursing: surgical site infection, wound complications (e.g., open wound, lymphatic leak) and use of negative-pressure wound therapy. Across all procedure types, lack of social support, physical frailty and cognitive impairment were most frequently identified as patient-specific considerations for prescribing home care nursing. Few respondents reported restrictions or standards that informed their prescribing practice.
Conclusion Most surgeon respondents agreed on the indications for home care nursing after vascular surgery. However, evidence-based standards to guide patient selection for home care nursing after vascular surgery are needed.
When patients are discharged from hospital after surgery, home care support can be provided to optimize their recovery at home.1 In a recent study of vascular surgery quality outcomes and costs within a single-payer health care system, home care services constituted an important proportion of health care cost within 30 days of discharge, second only to hospital readmission.2 A follow-up study of nursing care showed that receiving home care nursing (at home or in the community) was associated with a lower risk of hospital readmission or an emergency department visit within 30 days of discharge.3 However, home care nursing was inconsistently prescribed.3 Data on the use and effect of home care nursing after vascular or other surgeries remain sparse. Furthermore, the perceived indications for home care nursing among vascular surgeons remain uncertain. Given these considerations, our objective was to characterize the surgeon’s perspective on current indications for discharging patients with home care nursing after vascular surgery.
Methods
Study design
We conducted a survey of Canadian vascular surgeons to understand their prescribing practice with respect to home care nursing, in accordance with the Checklist for Reporting Results of Internet E-Surveys.4 We created the survey using the SurveyMonkey platform. It contained 31 multiple choice questions spread over 9 pages (with 1–6 items per page). Two authors tested the survey for ease of use and feasibility before submission. Potential respondents had the opportunity to change their answers throughout the survey by using the back button. We disabled multiple responses per Internet Protocol (IP) address to limit the number of multiple entries per individual. No personal information was collected or stored.
Respondents first identified their region of practice and hospital teaching status. A teaching hospital was defined as having residents or fellows rotating on the vascular surgery service at least 20% of the year. Respondents were then asked about their practice regarding discharge with home care nursing (at home or in the community) after 4 vascular procedures: carotid endarterectomy (CEA), open abdominal aortic aneurysm (AAA) repair, endovascular aneurysm repair (EVAR) and open or hybrid revascularization procedures for peripheral arterial disease (PAD). More specifically, they were asked about availability of home care nursing, defined as the possibility to prescribe it, if deemed necessary; pre-established local restrictions or standardized indications that dictate when home care can be prescribed within their institution or geographical area; and their perspective on procedure- and patient-specific criteria whereby a patient would benefit from home care nursing. Procedure-specific criteria related to any characteristic or complication of the procedure. Patient-specific criteria included patient characteristics (e.g., comorbidities, social status). Most procedure- and patient-specific criteria applied to all 4 major vascular procedures, with some exceptions that were specific to a single surgery type. For example, “complication of common femoral puncture” is a criterion that does not apply to carotid endarterectomy.
The online survey (Appendix 1, available at canjsurg.ca/001220-a1) was distributed to the 141 members of the Canadian Society for Vascular Surgery via its member email distribution list. An electronic informed consent form (Appendix 1) was provided along with the survey. We closed the survey after 1 month and 2 reminders. Survey responses were recorded by SurveyMonkey. Ethics approval for this study was granted by the Research Ethics Board of Unity Health Toronto.
Statistical analysis
The results were expressed in aggregate for all respondents and compared across procedure type, region and teaching status of the hospital (teaching v. nonteaching). We used Fisher exact tests for univariate comparisons, and we considered a 2-tailed p value < 0.05 the threshold for statistical significance. We included all questionnaires, even incomplete ones, in our analysis; the frequency denominator changes according to the number of respondents who completed each survey item.
Results
The survey response rate was 33% (46/141). Its completion rate was 89% (41/46). Responses originated from all regions of Canada: 35% (16/46) were from Ontario, 22% (10/46) were from the Prairies (Alberta, Saskatchewan and Manitoba), 15% (7/46) were from British Columbia, 15% (7/46) were from Quebec and 13% (6/46) were from Atlantic Canada (New Brunswick, Nova Scotia and Newfoundland and Labrador). A total of 62% (28/45) of respondents worked in a teaching hospital.
Availability, routine prescription and standardized indications for home care nursing
The reported availability, prescription and indications for home care nursing are shown in Table 1. Home care nursing was reported to be available by most respondents for CEA and EVAR, and by all respondents for open AAA repair and open or hybrid revascularization for PAD. When comparing specific nursing services across procedure types, wound care was available to all respondents after open or hybrid revascularization for PAD but not always for other procedures. If home care nursing was prescribed, the proportion of respondents making the referral themselves (as opposed to delegate such as a nurse practitioner or resident) was similar across procedure types. Home care nursing was routinely prescribed more frequently after open AAA repair and open or hybrid revascularization for PAD than CEA and EVAR. Restrictions or standardized indications for home care nursing were reported by a minority of respondents for all surgery types. None of the respondents who provided free-text comments suggested their practice was informed by any regional guidelines or procedure-specific restrictions. The comments centred around 3 main points: limited frequency of visits (e.g., “dressing change no more than once a day”), limited scope of services (e.g., “outpatient nursing care must provide a specific medical task and will not do routine care, such as removing staples”) and specified location of service (e.g., “most patients are now told to go to a clinic instead of the nurse coming to the home”).
Availability, indications and prescriber of home care nursing across vascular surgery procedures
Procedure- and patient-specific indications for home care nursing
The most frequently cited, procedure-specific indications for home care nursing were surgical site infection (25/42, 60%), outpatient negative-pressure wound therapy (18/42, 43%) and urinary catheter check or removal (16/42, 38%) for CEA; surgical site infection (32/41, 78%), lymphatic leak (31/41, 76%) and an open wound (27/41, 66%) for EVAR; an open wound (36/42, 86%), surgical site infection (33/42, 79%) and outpatient negative-pressure wound therapy (32/42, 76%) for open AAA repair; and surgical site infection, (36/41, 88%), lymph leak (36/41, 88%) and an open wound (36/41, 88%) for open or hybrid revascularization for PAD (Figure 1).
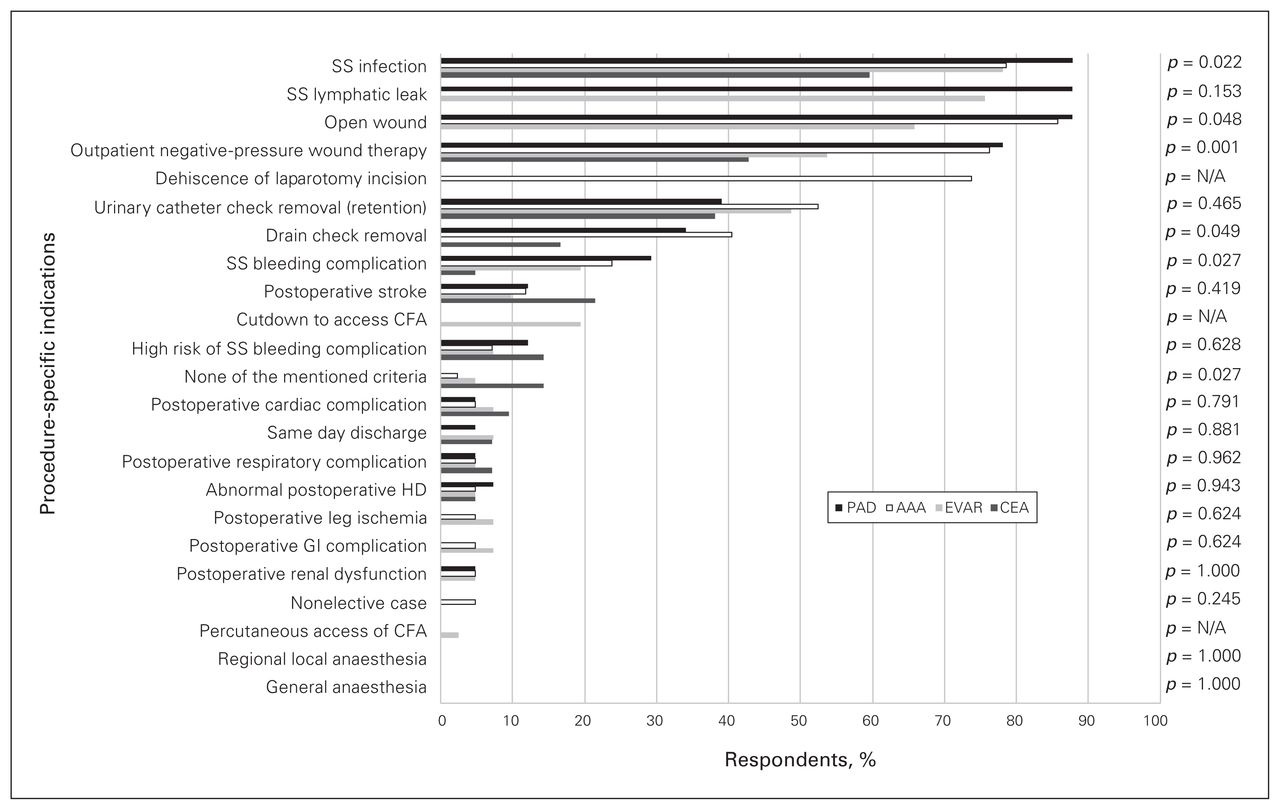
Procedure-specific indications for discharge with home care nursing after vascular surgery. AAA = open abdominal aortic aneurysm repair; CEA = carotid endarterectomy; CFA = common femoral artery; EVAR = endovascular abdominal aortic aneurysm repair; GI = gastrointestinal; HD = hemodialysis; N/A = not applicable; PAD = open or hybrid lower extremity revascularization for peripheral arterial disease; SS = surgical site.
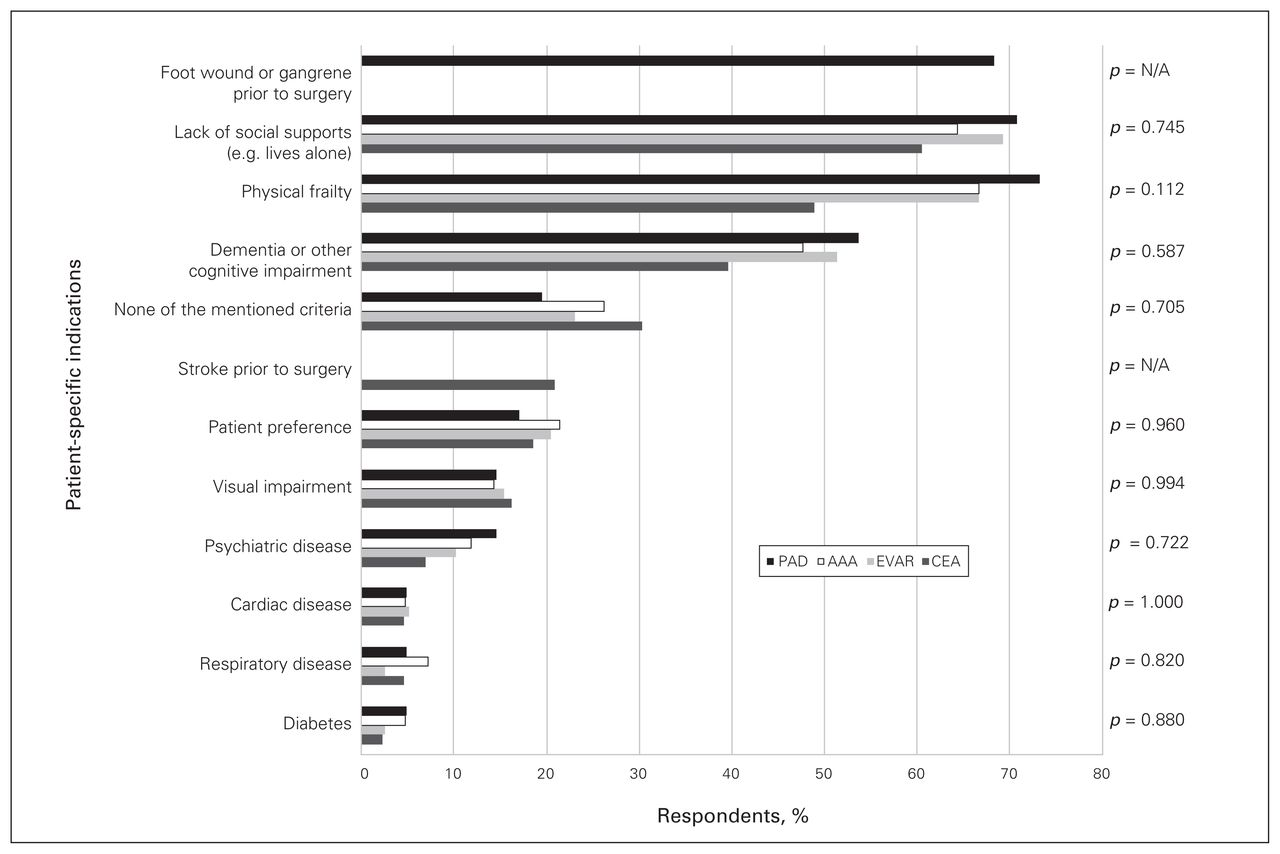
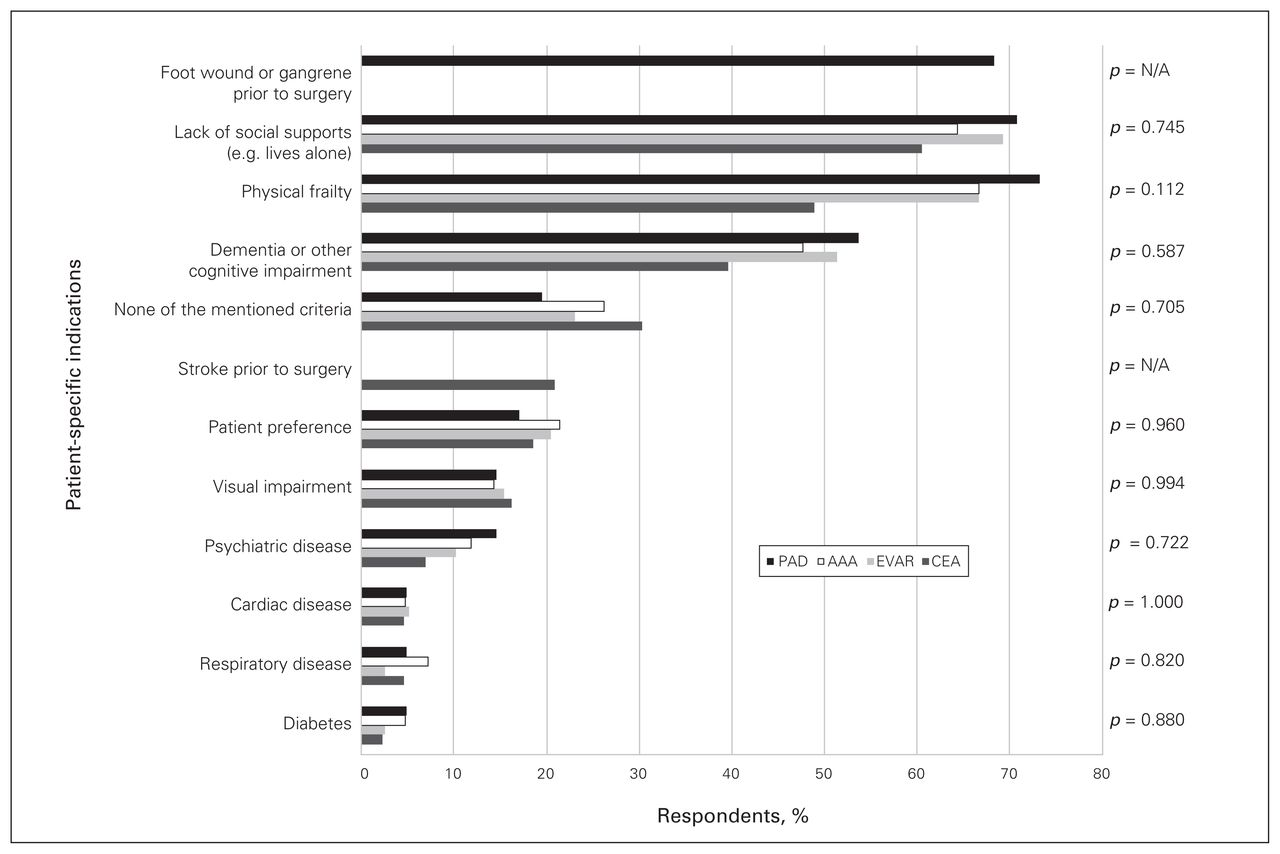
The most frequently cited patient-specific indications for home care nursing were the same for the 4 vascular procedures: lack of social support (60%–71%), physical frailty (49%–73%) and dementia or other cognitive impairment (40%–54%). There were no statistically significant differences observed between procedures (Figure 2).
{kind=link}
{kind=link}
Patient-specific indications for discharge with home care nursing following vascular surgery. AAA = open abdominal aortic aneurysm repair; CEA = carotid endarterectomy; EVAR = endovascular abdominal aortic aneurysm repair; N/A = not applicable; PAD = open or hybrid lower extremity revascularization for peripheral arterial disease; SS = surgical site.
Regional variation
Home care nursing was deemed to be similarly available across all regions, with the exception of home care nursing for administration of intravenous medication (Appendix 1, Tables S1, S2, S3 and S4). Furthermore, tendency to routinely prescribe home care nursing, and presence of restriction or standardized indications, did not vary significantly across region. Finally, there were no significant differences when regions were compared for patient-specific indications.
Variation by teaching status of the hospital
Comparing responses from respondents at teaching hospitals to those from community hospitals, there were no significant differences in home care nursing availability or tendency to routinely prescribe home care nursing (Appendix 1, Tables S5, S6, S7 and S8). The proportion of respondents indicating the presence of restrictions or standardized indications for home care nursing did not vary significantly by hospital teaching status. Respondents from teaching hospitals more frequently reported that patient preference is a relevant indication for home care nursing after CEA, EVAR and open AAA repair.
Discussion
This survey of Canadian vascular surgeons explored practice patterns and perceptions with regards to the prescription of home care nursing after vascular surgery. There were 4 main findings. First, the availability and routine prescription of home care nursing were higher following open AAA repair and revascularization for PAD than after CEA or EVAR. Second, there was general agreement on procedure-specific indications across all procedures (i.e., surgical site infection, outpatient negative-pressure wound therapy, lymphatic leak and open wound). Third, there was general agreement regarding patient-specific indications across all procedures (i.e., lack of social support, physical frailty and dementia or other cognitive impairment). Lastly, only a few respondents (about 10%) stated that their practice was informed by local restrictions or standards.
Data on the effect of home care nursing on readmission and health care cost after surgical interventions remains sparse, with a few recent examples relating to transurethral prostatic resection,5 joint replacement,6 pancreatectomy,7 day-case laparoscopic Nissen fundoplication8 and hemorrhoidectomy,9 short-stay programs after breast surgery10 and our group’s work on vascular procedures.2,3 Use of home care nursing internationally appears to be based on the opinion and training of health care providers. In the United States, eligibility for specifically covered Home Health Services under Medicare is left largely to the discretion of the physician.11 In the United Kingdom’s National Health Services, eligibility for funded home care support after discharge from the hospital also appears to be coordinated and determined by health care providers.12 A 2011 systematic review of home care across Europe identified a paucity of descriptive and comparative studies13 and led to increased interest and efforts to better describe home care, namely through the EURHOMAP (Mapping professional care in Europe) collaboration.14 Descriptive studies have shown that most eligibility criteria for home care are determined at a national, regional or municipal level for most countries.15 There are notable discrepancies among nations in the level of government involvement, informal care conditions and country wealth differences. All of these make transfer of home care policies among countries difficult.16 The EURHOMAP project has led efforts to raise awareness about ongoing demographic and social changes that increase the demand for home care17 and reinforce the importance of establishing clear criteria for home care, given the lack of consensus or guidelines.17 Although informative, these studies often fail to address home care eligibility specifically in the context of surgery, nor are they explicit on what constitutes appropriate referral criteria. Our study contributes surgeon-evaluated, relevant indications for discharging a patient with home care nursing after vascular surgery.
Several potential explanations exist for the increased tendency to prescribe home care nursing after open or hybrid revascularization for PAD and open AAA repair. Patients requiring revascularization frequently present with tissue loss, with rates as high as 84%.18 These require wound care for several weeks to months after revascularization to ensure proper healing and ongoing surveillance for infections. The fact that foot wounds and gangrene before PAD surgery were frequently cited as patient-specific indications for discharge with home care nursing further reinforces this hypothesis. Wound-related complication rates are also higher after surgical revascularization for PAD (14%)19 and after open AAA repair (7.1%),20 compared with 3.4% after EVAR21 and negligible rates after CEA.22 Open AAA repair also has high short-term complication rates20 compared with CEA or EVAR.23,24 For this reason, physicians may perceive that these patients are more likely to benefit from outpatient evaluation by a nurse before formal follow-up with the surgeon, even if no specific interventions, such as wound care or intravenous antibiotics, are mandated.
The similarities across regions and by hospital teaching status show a relative uniformity in the use of home care nursing across the country. However, in more sparsely populated areas, comprehensive follow-up may be more difficult to access and could result in a lower threshold to routinely prescribe home care nursing. In all settings, however, respondents identified a lack of local standards or guidelines. However, there did appear to be service limitations likely related to funding, as suggested by several comments. This reinforces the idea that evidence-based standards to guide patient selection for home care nursing after vascular surgery are needed to ensure that nursing care is prioritized toward those who benefit the most, especially in the context of scarce home care resources.
Limitations
Limitations of this survey should be made explicit. First, although our survey has captured a broad sample of vascular surgeons across Canada, the results may over- or underrepresent certain regions or practice types. Second, although the survey provides a nationwide perspective on home care nursing, discrepancies within regions could not be explored because of the small number of respondents and vascular surgeons currently working in Canada. Finally, the small sample size limits the power for statistical testing of differences across procedure types and regions.
Conclusion
Most polled members of the Canadian Society for Vascular Surgery had similar prescription patterns for home care nursing after vascular surgery and generally agreed on the potential indications for home care nursing. Although our data suggest general agreement among vascular surgeons, there remains a paucity of evidence to guide patient selection for home care nursing. Future research should focus on how patients benefit from home care nursing services after major vascular interventions. Our results should help define evidence-based standards of practice for home care nursing, which in turn will help best support patient recovery at home.
Footnotes
This work was presented at the University of Toronto Annual Research Day on June 21, 2019 in Toronto, Ont., and at the 19e Congrès annuel de la SSVq in Québec, Que., on November 21, 2019.
Competing interests: None declared.
Contributors: J. Jacob-Brassard and C. de Mestral conceived and designed the study. J. Jacob-Brassard acquired the data, which all authors analyzed and interpreted. J. Jacob Brassard and C. de Mestral drafted the manuscript, which all authors critically revised. All authors approved the final version to be published.
Funding: This work was supported by the Blair Foundation Vascular Surgery Innovation Fund, jointly established with the University of Toronto.
- Accepted April 18, 2020.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/