

Abstract
Background: Young men with osteoarthritis of the hip are a growing segment of the population requiring arthroplasty, and there is compelling evidence that the Birmingham Hip Resurfacing (BHR) system provides good functional outcomes and durability in young, active men. We reviewed the survivorship and clinical outcomes of patients who underwent BHR with a minimum follow-up of 10 years.
Methods: We analyzed survivorship using the Kaplan–Meier method. Functional scoring was performed using the Harris Hip Score (HHS), the University of California, Los Angeles (UCLA) Activity Score, and a visual analogue scale (VAS).
Results: In total, 211 patients (243 hips) were included in the study. Of these, 107 patients (127 hips) were available for long-term clinical follow-up, with a mean duration of 12.4 ± 1.4 years. The proportion of male participants with BHRs surviving past 13 years was 93.8% (95% confidence interval [CI] 87.9%–100%) compared with 87% (95% CI 77.8%–97.3%) of female patients. Eleven patients (11 hips) underwent BHR revision. Upon final follow-up, the median HHS was 93.9 in males and 93.6 in females (p = 0.27); median UCLA Activity Score was 8.2 in males and 7.2 in females (p < 0.001), and the median VAS score was 81.9 in males and 81.3 in females (p = 0.35). The median acetabular component inclination was 45.5° ± 6.0° (range 34.6°–57.2°) in males and 44.6° ± 5.9° (range 29°–58.9°) in females. The most common femoral head size was 50 mm with a 56 mm or 58 mm cup (36.3%).
Conclusion: This study confirms that BHR provides good to excellent functional outcomes, lasting functional improvements, and acceptable durability beyond 10 years in men. Survivorship following BHR is inferior in women; however, HHS and VAS scores were similar in women and men.
Young male patients with osteoarthritis of the hip are a growing and important segment of the population requiring arthroplasty.1 The success of total hip arthroplasty (THA) is well documented; however, there continues to be compelling evidence that hip resurfacing arthroplasty with the Birmingham Hip Resurfacing (BHR) system provides good functional outcomes and durability in young, active men. This is clinically relevant, as young men report decreased satisfaction following THA compared with BHR.2,3 There is growing evidence to suggest an improved return to high-level activities and sports following hip arthroplasty with a hip resurfacing.3 Other added benefits of hip resurfacing include the preservation of femoral bone stock, more accurate biomechanical restoration of the hip anatomy, decreased proximal femoral stress shielding, lower rates of dislocation, and superior patient-reported outcomes.4–6
A number of studies have reported mid-term outcomes5,7–11 and long-term (minimum follow-up of 10 years) outcomes12–21 of patients following BHR. However, most of those studies included patients with varying diagnoses, with no exclusions. We sought to report the 10-year survivorship and functional and radiological outcomes of consecutive patients who underwent BHR for osteoarthritis, performed by a single surgeon at a Canadian university hospital.
Methods
Study design
We conducted a retrospective study on consecutive patients who received BHR (Smith & Nephew Orthopaedics Ltd.) for osteoarthritis and had a minimum followup of 10 years. All operations were performed by a single nondesigner fellowship-trained arthroplasty surgeon (J.W.) at a Canadian university hospital between 2003 and 2009.
Following institutional review board approval, a retrospective chart review of the senior surgeon’s electronic medical records (EMR) was performed to identify all eligible patients. For the purpose of this study, only patients with an underlying diagnosis of primary osteoarthritis were included for analysis. Any patient who received BHR in the context of posttraumatic arthritis, avascular necrosis, inflammatory arthritis, or other conditions was excluded. Patients who met the eligibility criteria were contacted by telephone and offered an in-person follow-up appointment. If the patient was either unwilling or unable to attend the clinical appointment, they were considered lost to follow-up from the time of their last documented in-person appointment. Revision surgery was considered the end point of survivorship. We retrospectively collected data on patients’ baseline characteristics and, for those who underwent BHR revision, the date to failure and reasons for failure.
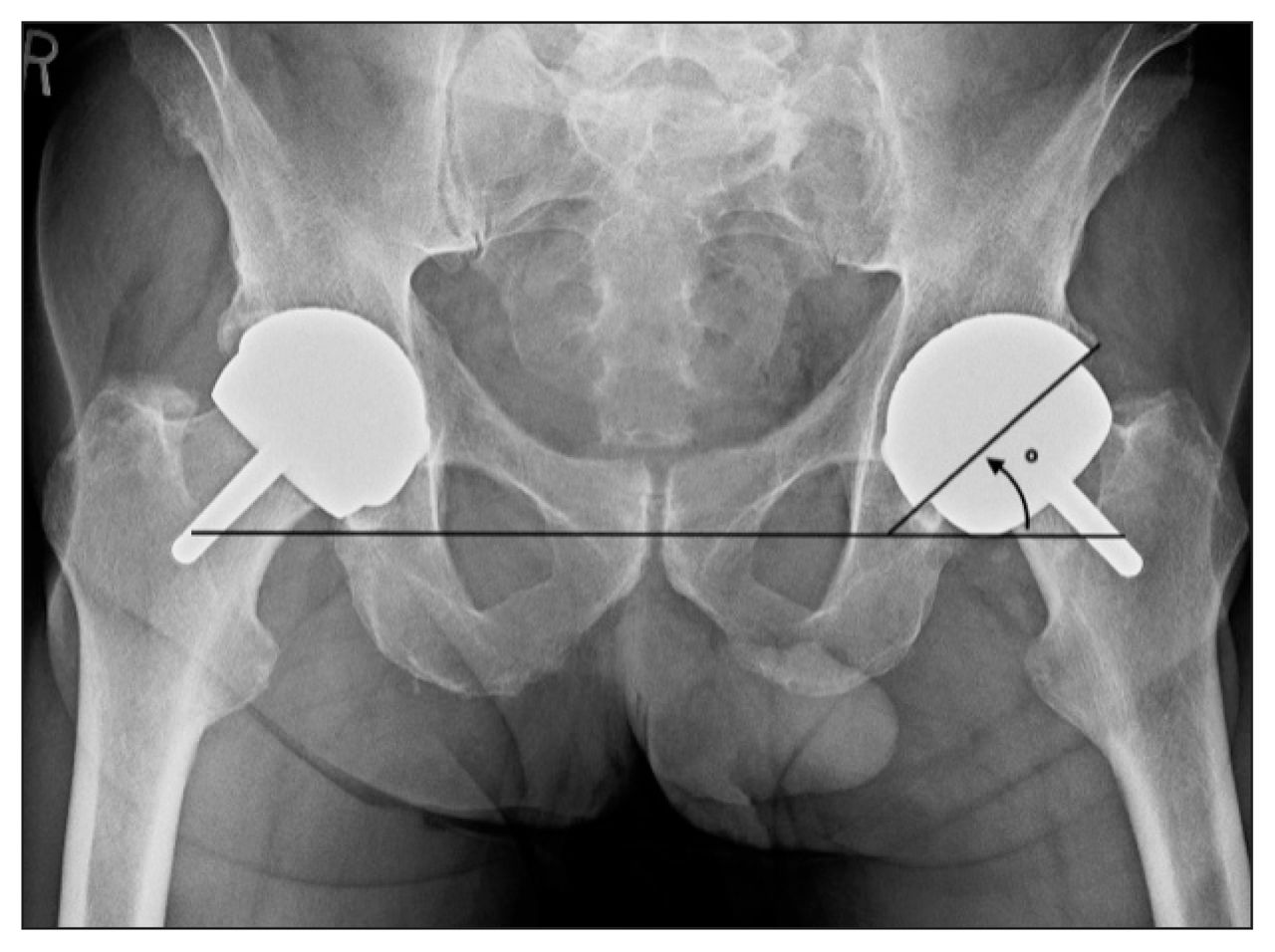
All patients’ follow-up appoinment in clinic occurred in June 2019, at which time we obtainded written informed consent from all participants. Patients underwent standard anteroposterior (AP) radiography (digitally recorded) before their follow-up in clinic in order for us to assess the implant position and identify any underlying osteolysis. Images were analyzed using IMPAX 6 software (AFGA Healthcare). Acetabular cup abduction angle (inclination) was recorded, as previously described by De Haan and colleagues22 (Figure 1). Osteolysis was defined as a radiolucency extending more that 2 mm from the surface of the prosthesis into the acetabulum or around the femoral stem.

Anteroposterior radiograph showing the measurement of the abduction angle (inclination) of the cup.
Functional scoring was performed using the Harris Hip Score (HHS) and the University of California, Los Angeles (UCLA) Activity Score. To improve the accuracy of our results, all patients were given the same instructions for completing the questionnaires. In addition, all patients were asked if there were any activities or sports that they ever avoided specifically because of their arthroplasty; we specified that avoidance could be for reasons including pain, instability, discomfort, or apprehension. Answers were recorded as a binary response (yes or no). Patients were also asked to grade their overall satisfaction with their BHR using a 100 mm visual analogue scale (VAS).
BHR technique
All operations involved a standard posterior surgical approach to obtain a 360° view of the acetabulum for optimal component positioning. Most patients received a spinal anesthetic at the time of the procedure; anesthetic type was left to the discretion of the anesthesiologist. Perioperative antibiotic prophylaxis consisted of a standard weight-based dose of cefazolin.
All acetabular components were uncemented, relying on the porous, hydroxyapatite-coated surface for long-term stability. The acetabula were underreamed to allow press-fit fixation. The acetabular components were then fully impacted with an intended 40°–45° of inclination and 15°–20° of anteversion. The external diameter of the acetabular components ranged from 48 mm to 62 mm. The diameter of the acetabular component was either 6 mm or 8 mm larger than the corresponding femoral component. Osteophytes around the acetabulum were removed to avoid impingement.
Osteophytes on the femoral neck were removed to ensure an accurate measurement of the head:neck ratio. Implant sizing based on the femoral neck also ensured adequate offset. The McMinn alignment jig was used for intraoperative femoral orientation. All BHR femoral components were cemented using Simplex T bone cement (Stryker). The femoral components were placed in 5°–10° of valgus relative to the femoral neck.
All patients followed a standard postoperative hip arthroplasty care pathway. This included receiving low-molecular-weight heparin (dalteparin) for 28 days postoperatively for venous thromboembolism prophylaxis and discharge from the acute care hospital within 24–48 hours postoperatively. Patients were encouraged to mobilize early, with immediate weight bearing as tolerated. All patients had clinical follow-up at 2 weeks, 6 weeks, 3 months and 1 year following surgery. Outpatient physiotherapy was instituted for all patients within 6 weeks postoperatively. A graduated return to sport was allowed without restrictions after 3 months.
Statistical analysis
All statistical analyses were performed with R software version 3.6.123 and R Studio24 using different packages.25–32 We analyzed demographic and clinical characteristics using frequencies and percentages for categorical data, and using mean and standard deviation or median and range for continuous data. Kaplan–Meier survival analysis was undertaken on the data sets, by gender, with 95% confidence intervals (CIs). Patients lost to follow-up were accounted for until their last documented clinic visit. The Shapiro–Wilk test of normality was applied to all unpaired (HHS and UCLA Activity Score) data. We used the Wilcoxon signed-rank and rank-sum tests for HHS and UCLA Activity Score data. We considered results to be significant at p < 0.05.
Results
In total, 211 patients (243 hips) met the inclusion criteria. Nine patients (12 hips) died from causes unrelated to surgery before this study. Eleven patients (11 hips) required a revision surgery. Forty-five patients were unable to be reached, and 33 patients declined to participate in the study. All these patients’ data were included for analysis up to the time of their last clinic visit and then considered lost to follow-up. Of the 113 patients scheduled for office follow-up, 6 did not show up to their appointment and were also considered lost to follow-up. Patient baseline demographic characteristics are presented in Table 1.
Baseline patient characteristics, by gender
The mean age of the remaining cohort (107 patients; 127 hips) at the time of surgery was 49.1 years (males: 50.3 ± 6.6 yr; females: 45.1 ± 8.1 yr). There were 39 bilateral procedures, 11 of which were performed simultaneously (7 males with a mean age of 46.9 ± 5.2 yr and 4 females with a mean age of 50.8 ± 2.3 yr). Of the 28 patients who underwent staged BHR, 19 had their second BHR performed less than 10 years before the final follow-up, and therefore their clinical and functional assessments account for only their first hip resurfacing. The mean duration of follow-up was 12.37 ± 1.4 years. The average body mass index (BMI) of our cohort was 28.27 ± 5.2 kg/m2 (males: 28.97 ± 5.0 kg/m2; females: 25.87 ± 5.2 kh/m2).
Survival analysis
Of the 211 patients available for study inclusion, 45 were unable to be reached via telephone. The EMRs of these patients were reviewed, and none underwent revision BHR surgery. The 33 patients who were contacted via telephone but declined to participate in the study did answer questions regarding failure of the procedure and whether they underwent BHR revision. Therefore, implant survivorship analysis was performed on all 211 eligible patients (243 hips).
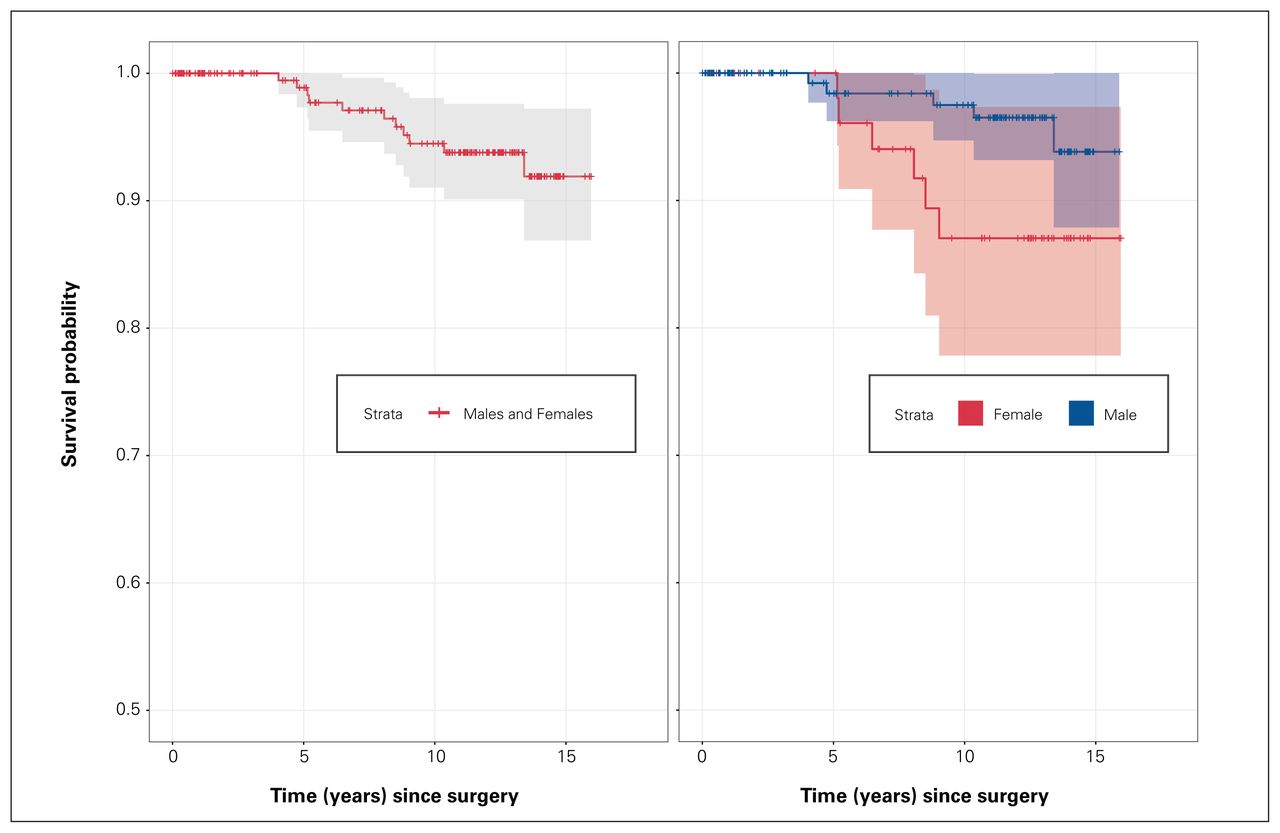
Kaplan–Meier survival curves are presented in Figure 2. The proportion of patients with a BHR surviving past 13 years was 91.9% (95% CI 86.9%–97.2%). The proportion of male participants with BHRs surviving past 13 years was 93.8% (95% CI 87.9%–100%), whereas the proportion of female participants with BHRs surviving past 13 years was 87% (95% CI 77.8%–97.3%).

Survival curves following Birmingham hip resurfacing.
Details of all 11 patients who underwent revision surgery, along with time to failure and reasons for failure, are presented in Table 2. Of this cohort, 11 patients (5 males and 6 females; 4.13%) underwent BHR revision. The average time to revision surgery was 98.6 ± 47 months (8.2 yr; range 48–160 mo) in males and 92.8 ± 19 months (7.7 yr; range 62–110 mo) in females.
Characteristics of the 11 patients who underwent BHR revision
Two of the patients developed symptomatic aseptic lymphocyte-dominated vasculitis-associated lesions (ALVAL) or pseudotumours, 2 developed acetabular cup loosening, 2 developed aseptic femoral loosening, 1 had vague hip symptomatology with elevated whole-blood metal ion levels (cobalt 7.12 ng/mL; chromium 9.66 ng/mL), 1 had a periprosthetic femur fracture, 1 developed femoral avascular necrosis with subsequent femoral implant subsidence, and 1 patient was symptomatic from anterior hip impingement. These 10 patients were ultimately revised to a THA.
One of the patients required their acetabular cup to be revised to a BHR dysplasia cup after the native BHR cup loosened (Figure 3). This patient agreed to follow-up with us in clinic as part of the study. The patient expressed their satisfaction with the revised prosthesis, and admitted to returning to a very active lifestyle involving regular participation in moderate-to high-impact sports.

{kind=link}
{kind=link}
{kind=link}
Radiograph showing a patient who required revision surgery for a loose acetabular cup. The patient would be revised to a BHR dysplastic cup. BHR = Birmingham hip resurfacing.
The average inclination angle for acetabular cups in these patients was 41.1° in males and 40.1° in females. Of the 10 patients who had their BHR revised to a THA, the average femoral head size of their original implant was 54 mm (range 50–58 mm) in males and 44 mm (range 42–48 mm) in females.
Radiographic analysis
All pelvis radiographs were independently reviewed by 2 senior orthopedic surgery residents (J.B.M. and J.L.) and the senior author (J.W.). There were no cases of osteolysis or changes in component position in any of the patients. One patient developed asymptomatic heterotrophic ossification (Brooker classification 2; bone spurs with ≥ 1 cm between pelvis and proximal femur projections). The acetabular cup abduction angle (inclination) was on average 45.5° ± 6.0 (range 34.6°–57.2°) in males and 44.6° ± 5.9 (range 29°–58.9°) in females (Table 3). The most common femoral head size was 50 mm with a 56 mm or 58 mm cup (36.3%). Second to these was a femoral head size of 46 mm with an acetabular cup of 52 mm (18.6%). Of note, the 46 mm femoral components (and smaller) in the BHR system are no longer available; the smallest femoral component now available is 48 mm. The complete implant size data are presented in Table 3.
Implant characteristics
Functional outcome
Functional scores as assessed by the HHS and UCLA Activity Score questionnaires are summarized in Table 4. The median HHS at final follow-up was 93.9 ± 9.3 (range 40–100) for males and 93.6 ± 11.7 (range 40–100) for females; a difference that was not statistically significant (p = 0.27). The UCLA Activity Score was 8.2 ± 1.3 (range 3–10) for males and 7.2 ± 1.6 (range 3–10) for females. The difference in UCLA score between men and women was statistically significant (p < 0.001). Lastly, patient satisfaction as measured with a VAS showed a median VAS of 81.9 ± 11.1 (range 50–100) for males and 81.3 ± 15.6 (range 25–100) for females (p = 0.35).
Mean patient-reported outcome scores at final follow-up
All but 2 patients (98.1%) admitted to returning to their preferred moderate-to high-level activities and sports (e.g., downhill skiing and mountain biking) and reported not feeling limited by their arthroplasty. The 2 patients who refrained from participating in activities or sports admitted this was because of apprehension rather than from objective functional limitations or hip symptomatology. Two patients reported having intermittent “squeaking” from the hip (1.6%), and 1 hip elicited a clicking sound (0.8%), yet these patients reported no pain or discomfort and had no objective signs at the time of the final follow-up.
Discussion
The aim of this study was to report the long-term survivorship and functional outcome of the BHR in a consecutive series of patients with osteoarthritis who had a minimum 10-year follow-up. Our findings corroborate the long-term efficacy of BHR in young male patients by demonstrating good implant survivorship (with 93.8% of male patients’ BHR surviving past 13 years), improvements in patient-reported outcomes, and sustained ability to participate in activities and sports beyond 10 years postoperatively. While many studies have reported long-term outcomes of the BHR,12–21 most had heterogeneous cohorts of patients who underwent hip resurfacing for different underlying diagnoses. Our study represents a large single-surgeon case series assessing 10-year survivorship, functional and radiological outcomes in consecutive BHRs performed for osteoarthritis. This study therefore extends on the current literature by focusing on implant survival and functional outcomes in patients who received a BHR specifically for osteoarthritis.
The continued use of BHR depends in part on its comparability to THA. The foremost challenge in performing THA in younger males has been to develop bearing surfaces that can withstand higher demands and expected greater longevity. Jonas and colleagues33 recently compared the long-term clinical and radiological results of patients with metal-on-polyethylene hybrid THA to BHR. They found that after 18 years, patients with a BHR remained more active and had a lower mortality rate than patients with hybrid THA. On the other hand, ceramic-on-ceramic THA provides excellent wear resistance owing to its hard-on-hard articulation resulting in minimal osteolysis and improved implant longevity.34–35 Mahiques-Segura and colleagues36 compared outcomes of 94 patients aged 20–40 years who received a cementless ceramic-on-ceramic THA (mean follow-up of 13.6 yr) to 90 older patients (mean age 64.7 yr) with the same implant. They reported an implant survivorship of 94.7% at 14 years in the younger patients compared with a survivorship of 98.3% in the older patients. These findings show that THA with an enhanced bearing surface is less durable in younger, active patients. In comparison, Scholes and colleagues37 reported on the survivorship of BHR in patients younger than 50 years with a minimum 10-year follow-up. They found a cumulative rate of survival of 96.8% at 15 years (99.4% for men and 93.8% for women). These findings are in keeping with those of an earlier study that reported a cumulative survivorship of BHR of 96.3% in patients younger than 50 years.19
Our study design allowed us to have patients return to our clinic for a long-term follow-up appointment during which up-to-date patient reported outcome scores (PROMs) were collected. To improve the accuracy of our results, all patients were given the same instructions for completing the questionnaires. The results obtained from the HHS questionnaires show that, on average, patients report good to excellent hip function at a mean follow-up of 12.4 years. These findings are in accordance with those of a previous study.18 We also found that HHS and VAS scores did not differ between males and females. The mean UCLA Activity Score, on the other hand, was significantly inferior in females than males in our study (7.22 v. 8.2, p < 0.001). However, regardless of sex, these results indicate that most patients continue to engage in high-level activities after surgery. Our results are consistent with those of other studies reporting long-term clinical outcomes following BHR.14,15 Treacy and colleagues14 showed a median UCLA Activity Score of 7.0 (interquartile range 5.0–8.0) in their series of 144 BHRs at a minimum of 10 years, whereas Holland and colleagues15 showed a median UCLA Activity Score of 7 at the 10-year review. Put together, our results are in line with the current literature supporting the intention of BHR, which is to relieve pain, restore hip function and permit an active lifestyle.
Limitations
While the present study has expanded on the current literature about the long-term sustained improvements following BHR for osteoarthritis, it should be interpreted in light of its limitations. The surgeries in this cohort were performed by a nondesigning surgeon and include some of the surgeon’s first BHRs completed in his independent practice, therefore accounting for the learning curve with this procedure. It is important to recognize the technical demands in performing a BHR. Though the results achieved in this study compare with those of other studies,13–15 they may not be achievable and reproducible when performed by other less technically familiar surgeons. In addition, another potential confounding variable that could not be controlled for because of study design is the documented primary diagnosis at the time of surgery. While we carefully triaged patients from the senior surgeon’s EMR, there may be inherent misclassifications; for example, underlying developmental dysplasia of the hip. Second, we acknowledge the lack of preoperative PROM scores, which hindered us from examining any long-term changes in these parameters. Finally, pelvic radiographs were obtained and reviewed during the latest follow-up. This offered an opportunity to identify any asymptomatic patients with radiographic evidence of osteolysis or implant failure. This was a limitation identified in previous long-term studies.16,20
Conclusion
We report good survivorship and functional outcomes of BHR, more so in male than in female patients, at an average age at surgery of 49.1 ± 7.3 years and with a minimum of 10 years of follow-up. These findings support the current evidence regarding the benefits of BHR in active young males with osteoarthritis.2,3
Footnotes
Competing interests: None declared.
Contributors: J. Bourget-Murray, S. Watt Kearns, J. Lukenchuk and J. Werle designed the study. J. Bourget-Murray, S. Watt Kearns, S. Piroozfar, J. Lukenchuk and J. Werle acquired and analyzed the data, which K. Johnston also analyzed. J. Bourget-Murray, S. Watt Kearns, J. Lukenchuk and J. Werle wrote the article, which all authors revised. All authors gave final approval of the article to be published.
- Accepted April 27, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/