

Abstract
Background: Orthopedic surgeons routinely prescribe opioids to manage post-operative pain. In the face of an opioid epidemic, a one-size-fits-all approach to pain management is no longer appropriate. Patient-centred prescribing practices should be used by surgeons; however, little is known about what influences patient attitudes toward postoperative pain and its management to inform such practices. We sought to explore patient attitudes toward postsurgical pain management, including opioids.
Methods: We conducted qualitative, semistructured interviews of 11 opioid-naive patients (age 16–46 yr) who were scheduled to undergo arthroscopic knee surgery. Transcripts were analyzed thematically using a framework analysis that involved familiarization, developing a thematic framework, indexing, charting and mapping, and interpretation.
Results: Participant attitudes toward postoperative pain and opioids were influenced by perceived tolerance to pain based on personal experience, perceived predisposition to addiction based on personal assumptions regarding addictive personality traits and risk factors, and perceptions of opioid use shaped by external influences, including family, friends and the media’s depiction of the opioid epidemic. Every patient expressed that preoperative counselling and education regarding postoperative pain management would be beneficial in improving their knowledge base, easing anxieties and clarifying misunderstandings.
Conclusion: Surgeons can address the patient-reported factors identified in this study to help optimize a patient’s perioperative experience without relying solely on prescribed analgesia. By improving accessibility to education and promoting safe, patient-centred prescribing practices, we may reduce reliance on opioids in orthopedic surgery.
In recent years, Canada has had an opioid crisis,1 with one of the highest per capita consumption rates of prescription opioids in the world.2 Prescribing practices, among other causes, have played a substantial role. In 2011, the medicinal opioid consumption (in morphine equivalents) was 812 mg per person in Canada — far greater than the global average of 62 mg per person.3
Health care providers play a fundamental role in ensuring safe and effective drug use. For surgeons, this can be challenging. Pain is typically part of most operative experiences, and despite advances in multimodal analgesic protocols and access to nonpharmaceutical interventions, opioid prescription remains a common tool in postoperative pain management.4
Surgery is a common setting in which opioid-naive patients are first exposed to opioids, with as many as 1 in 16 patients subsequently becoming long-term users.5 Many surgeons prescribe a default number of pills according to the surgery performed, rather than evaluating specific patient needs.6 Studies indicate that 70%–90% of prescribed opioids after surgery remain unused.7 Often, these are not disposed of properly, and may ultimately be an important reservoir for nonmedical and recreational use.
A better understanding of patient factors and perceptions may help to improve prescribing practices among surgeons. In this study, we sought to explore the factors that influence a patient’s perception of postoperative pain management after arthroscopic knee surgery.
Methods
We included opioid-naive patients aged between 16 and 65 years who were scheduled to undergo arthroscopic knee surgery. We defined “opioid naive” as the absence of opioid use for at least 12 months before surgery.8,9 We excluded patients if they did not speak English or had been prescribed opioids for conditions unrelated to their surgery. A single, university-affiliated orthopedic surgeon performed the surgeries between 2018 and 2019.
Recruitment and data collection
We asked eligible patients to participate in a study about opioid use by email. We provided details of the study in an information sheet and obtained informed consent over the phone or in person. A trained interviewer (A.A.) conducted all phone interviews, which explored patient attitudes and perceptions about post-operative pain and opioid use. Interviews were audio-recorded and followed a semistructured framework, developed collectively by the research team (Appendix 1, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.004321/tab-related-content). Using an iterative approach, the interviewer modified questions as needed between interviews, allowing for exploration of emerging insights and themes in subsequent interviews. The sample size was determined once data saturation had been achieved;10 in other words, we stopped data collection once no new concepts, themes or explanations emerged from the interviews.
Data analysis
A third-party service (CM Business and Transcription Services) transcribed the interviews. Anonymity was preserved using an alphanumeric identifier for each patient. Two members of the research team (A.A., J.A) independently coded the transcriptions in Microsoft Excel. Guided by the steps outlined in framework analysis,11 we created a thematic framework to organize, understand and interpret the data. The steps that were followed were familiarization, creating a thematic framework, indexing, charting, mapping and interpretation.
Ethics approval
This study was approved by the research ethics board at Michael Garron Hospital.
Results
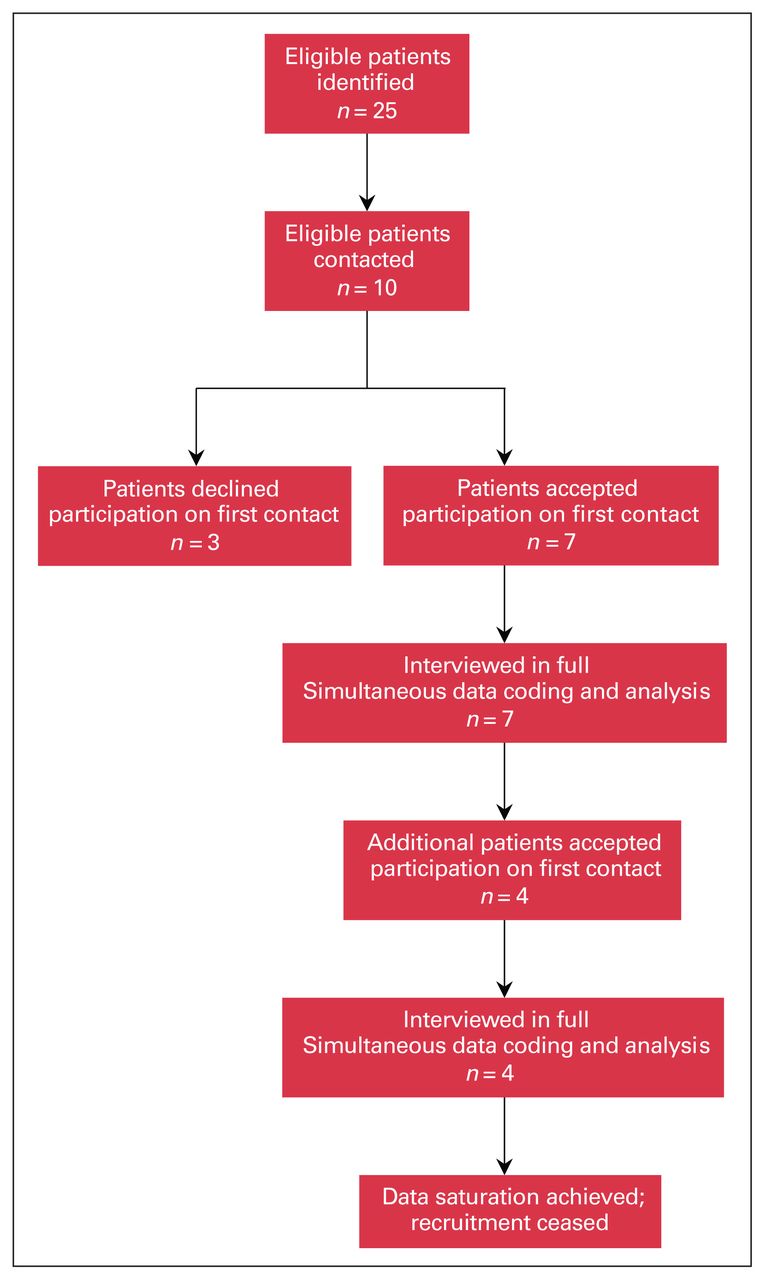
We interviewed 11 opioid-naive patients, aged 16–46 years (6 men, 5 women) before their arthroscopic knee surgeries (Figure 1). Scheduled surgeries, including arthroscopic meniscectomies and anterior cruciate ligament reconstructions, were performed after the interviews were conducted.

{kind=link}
Study flow diagram.
We found that participant perceptions around post-operative pain and intended opioid use were influenced by 3 main factors, namely perceived pain tolerance, perceived predisposition to addiction and perceptions of opioids, shaped by external influences.
Perceived pain tolerance
Patients often had preconceived notions about how they would respond to postoperative pain. For instance, despite any of our patients having previously undergone surgery, all of them expressed an opinion on how they would tolerate postoperative pain. Each participant self-characterized themselves as either having a high or low tolerance to pain based on their previous experiences.
Those who identified as having a low pain tolerance were characteristically more anxious and apprehensive about surgery. They often expressed difficulties coping with pain and were consequently occupied by their level of postoperative incapacity:
“I am very concerned [about the surgery] because I don’t take pain that well” (A03 [40–41]).
“I’m in a field of work where I have to be cognitively sharp in order to do my job, and if I’m in pain, I’ll be distracted” (A10 [72–81]).
In contrast, patients who described themselves as having a high pain tolerance described less anxiety about the procedure and their postoperative course. These participants, who made up most of our study population, found reassurance by reflecting on episodes where they managed traumatic pain successfully in the past. Many even drew inspiration from their ability to, thus far, cope with the pain from their existing knee pathology:
“With my knee, I sort of feel like I’m going through pain … I’m just going through the pain again [after the operation], so I’ll just work through [it]” (A01 [41–43]).
A select few individuals saw their operation primarily as a pain-relieving procedure. Thus, they inadvertently expected little to no pain afterwards:
“I was told that right after the surgery I should be able to walk and I shouldn’t have pain, so I don’t have much concern about that to be honest” (AO2 [31–33]).
Patients who identified as having a high pain tolerance had less concern about the effects of opioids. In comparison, those with low pain thresholds often described substantial apprehension about opioids and postoperative analgesics more generally:
“I do have a little bit of concern, just because I don’t know how my body will take [the medication] and how it will process them. And then what it would be like getting rid of them?” (A03 [121–123]).
Despite disparities in perceived pain tolerance, patients expessed similar strategies in managing postoperative pain. Almost all participants saw the role of analgesia as a means to minimize pain rather than to completely alleviate it. A multimodal approach to wean off narcotics was appealing to most participants, suggesting that this could be a healthy strategy for health care professionals to use.
Perceived predisposition to addiction
Most participants felt that they were not prone to addiction. Of the many reasons described, the most common was a perceived absence of an addictive personality. One patient contrasted his personality to that of his mother (who had previously suffered from opioid dependency):
“I don’t have an addictive nature like my mom … I’m not saying that I’d be immune to addiction, but I don’t think [I’d become] dependent on painkillers … I’d have to have a pretty bad headache or a pretty bad injury to take painkillers, so I don’t think I’d [get] addicted to them” (A07 [125–137]).
Another participant felt that her knowledge of opioids and their harmful effects would discourage any propensity for addiction. She had a very supportive network of friends and family around her, which she felt was also protective:
“… because of my awareness of the issues with addictions, I think that I would have the ability to cut myself off” [121–122]. “You hear about [addiction] in the smaller communities where they don’t have a lot of community supports … [164–165] I have a relatively good support system … so I’m not by myself in this. I imagine I’ll be okay” (AO9 [158–164]).
One participant who had used opioids for a previous injury described that the adverse effects he encountered with opioids served as a deterrent for any addiction:
“Between you and I …. when I hear people becoming addicted to these things and abusing them as recreational drugs, it baffles me. When I took them, I thought that the side effects were just not worth it. I hated the side effects” (A10 [124–129]).
These results highlight prevailing opinions about the notion of an addictive personality. They also show how knowledge of the risks and adverse effects of opioids, in addition to having a strong support network, was empowering and curtailed concerns about developing addiction.
Perceptions of opioids from external influences
Most participants had a negative outlook toward opioids, indicating that they would try to avoid using them if possible. Their views often stemmed from external influences, including first-hand experience in observing friends or family members develop addictions.
“… when I was watching my mom, it got to a point where I didn’t really know if it was about the pain any more … . She liked [the opioids] too much and it took her a while to wean herself off” (A07 [78–89]).
“The biggest concern [I have] with taking opioids is that people get really addicted. I’ve had family members who have been in hospital … on some type of opioid for pain management. And then when [they’ve left] … they would start to look for those same drugs but just not through the hospital … so I’ll probably do my best to stay away from opioids” (A04 [135–143]).
More commonly, aversion to opioids among our interviewees stemmed from how opioids are depicted in the media, particularly for our participants who did not have personal experience from which to base their opinions. Most participants agreed that the media’s focus on recreational opioid use has fueled a stigma against any potential therapeutic uses for opioids and against addiction disorder. One participant admitted that he did not even know about the therapeutic effects of opioids before conversations leading up to his surgery:
“[The coverage is] all negative right now and … I didn’t even know you could take [opioids for surgical recovery] and that’s why you took it. I didn’t even know that that was an option. There is not really the education out there” (A01 [264–268]).
None of the participants attributed discussions with health care professionals or health care resources in helping develop their perceptions regarding post-operative pain and analgesia. All patients felt that more in-depth conversations with their doctors about postoperative pain and analgesia protocols would be beneficial in setting expectations, easing anxiety and making informed decisions.
“… if you were to say to me I’m going to give you medication A and it’s going to help with pain but it’s going to slow down your healing process. Or I can give you medication B and it’ll deal with pain [to a lesser degree] but it won’t affect your healing process. I’m going to go with B because I would rather get the healing process underway …” (A10 [255–265]).
This indicates that a one-size-fits-all approach to postoperative pain management is not ideal and that patients would benefit from discussing multiple options of pain management.
An absence of shared decision-making could result in mistrust in prescribing practices:
“I would assume that there is some sort of incentive. Basically, I feel drug companies drive the fact that doctors are always so quick to prescribe opioids … I would assume that [they prescribe opioids] because they’re one of the more addictive prescriptions that you could get, and then that will fund the drug company further” (A04 [96–104]).
This highlights the need for increased communication between physicians and patients about selection of postoperative analgesia. Regular dialogue about peri-operative pain management can help patients play an active role in their postoperative care and strengthen the doctor–patient relationship.
Discussion
We investigated patient attitudes toward pain management and opioid use, and their influences, in preoperative patients undergoing knee surgery. Our findings suggest that perceived pain tolerance, proneness to addiction and external factors influence attitudes toward postoperative pain and opioid use. Our study also found that participants did not perceive themselves as likely to become addicted to opioids, and that conversations with their surgeons about postoperative pain management are lacking. Hence, we not only identified targetable, patient-endorsed areas to optimize the postoperative pain experience, but also potential contributions to the opioid crisis that continue to go unaddressed.
Although, historically, pain has been perceived as proportional to host tissue damage, recent orthopedic literature has shown that variations in pain intensity depend more on the psychosocial aspects of illness.12–14 Numerous studies have shown that objective indices of pathology, such as radiographic severity, correlate weakly with pain severity and disability.15–18 Hence, identifying the behavioural and psychological influences on clinical pain severity are important to optimize treatment outcomes for patients.19
An individual’s psychological perceptions of pain may ultimately affect their pain experience.20 Specifically, an inflated expectation of pain may lead to an increased pain experience. Koyoma and colleagues21 conducted a study with functional magnetic resonance imaging whereby different temperature stimuli were administered to patients. They found that expectations of increased pain (illustrated by longer waiting time between temperature stimuli) strongly activated neuronal processes that influence physical sensation. Conversely, expectations of decreased pain profoundly reduce both the subjective experience of pain and pain-related brain activation.21 The linear association between expectation and pain perception has been shown in surgical patients.22 These findings suggest that, in our cohort, patients who identified as having a high pain tolerance may be more prepared to manage pain after surgery. Conversely, those who biased toward low pain tolerance expressed more anxiety and saw pain as a threat. Such responses can lead to the development of negative psychological adjustments such as catastrophic thinking,23 which has been linked to amplified postsurgical pain and a higher likelihood of prolonged opioid use.24–26 Hence, identifying patients at risk of catastrophizing before surgery is critically important and may serve as part of the justification for preoperative counselling and education.
We found that many of our patients shared important misconceptions about addiction risk. For instance, many credited their lack of an addictive personality as protection from developing an opioid addiction. The current body of literature does not support this. Associations between specific personality traits and developing addictions are not well established,27 though some traits that are described include sensation-seeking and impulsivity.28,29 Risk factors that have been well established in predicting risk of developing addiction serve as the basis of the Opioid Risk Tool30 and include previous family history of dependency, owing to the strong genetic influence seen in opioid abuse.31 Several of our participants who had a family history of opioid dependency falsely assumed themselves not at risk because they felt they did not have an addictive personality — a premise without evidence base.
The media shaped many of the negative perceptions our participants had toward opioid use. One study that evaluated the content of media coverage pertaining to opioids between 1998 and 2012 found the news media was far more likely to frame opioid misuse as a criminal justice issue than as a treatable health condition.32 This one-sided portrayal not only propagates negative stigma toward opioids and those who use it, but also propagates the misconception that opioid use disorder is a willful choice rather than a medical illness.33 Other studies suggest that portrayals of the therapeutic uses of opioids can reduce stigma and reduce discrimination against opioid use disorder.34 Currently, only a third of news stories depict individuals engaging in treatment.32
When exploring strategies that would help address the concerns our subjects had with postoperative pain management and opioid use, there was universal appeal for increased counselling about expected postoperative course, pain and analgesic strategies. Counselling not only helps ease anxiety but also offers patients an opportunity to be involved in the decision-making processes of their postoperative care. The literature also supports this; education about perioperative care has been shown to reduce preoperative anxiety, postoperative pain and post-surgical calls at the office.35 Holman and colleagues36 set an expectation with orthopedic trauma patients that opioid provision would end 6 weeks after surgery. Their findings showed that the intervention group had a significant decrease in continued opioid use after 6 weeks. Alter and colleagues37 performed a prospective comparison of patients undergoing carpal tunnel release surgery to either receive preoperative counselling or not. They found significantly fewer opioid pills prescribed in the group that underwent counselling, with no significant difference in pain level experience. Similarly, Hah and colleagues38 conducted a randomized controlled trial that explored the effects of postoperative motivational interviewing and guided opioid tapering in patients undergoing total hip or knee replacement surgery. They showed quicker postoperative opioid cessation without any difference in persistent postsurgical pain and patient-reported recovery across all patient groups, including patients with pre-existing pain and opioid use.
A panel of orthopedic trauma surgeons recently issued guidelines about management of musculoskeletal pain.39 They strongly recommended department support in opioid education for prescribers and patients, highlighting that educational interventions, in addition to reducing opioid prescriptions, reduced risky behaviours associated with opioids, such as pill sharing, inappropriate disposal, driving and taking more medication than prescribed.39 Approaches such as pamphlets, web-based interactive education and clinician-led education all showed significant effects.40 Educational interventions for physicians were notably effective; introducing continuing medical education sessions about pain and addiction was met with decreased opioid prescribing and drug overdose deaths in New Mexico.41 Other strategies to improve on prescribing practices include emphasizing multimodal analgesic regimes, involvement of pain specialists and system drug monitoring programs. Moreover, these guidelines also highlighted the importance of addressing patient anxiety and recommended that clinicians incorporate psychosocial interventions, including cognitive behavioural therapy, to improve postsurgical pain and overall outcomes.39
Limitations
The main strengths of this study were its qualitative design and use of in-depth, semistructured interviews to understand how patients regard postoperative pain management. Another strength was that the interviewer was not involved in any aspect of care for the patients; thus, patients could feel free to share sensitive views about opioids without fear of compromising the patient–prescriber relationship. However, this study was subject to the limitations of any interview-based methodology. Patients who agreed to participate may have had divergent views from those who declined. This study was also limited to a patient population of 1 urban academic surgeon. Future investigations using a mixed-methods approach — combining qualitative measures of patient perceptions and quantitative analysis on analgesia prescribed — may better support this work and provide insight on prescribing practices.
Conclusion
Patients undergoing arthroscopic knee surgery identified their perceived tolerance for pain, predisposition to addiction and external influences as important factors that influence their attitudes on pain management and opioid use. By improving accessibility to education and promoting safe practices via a patient-centred approach to postoperative analgesia, we may reduce the reliance on opioids in orthopedic surgery and curtail their adverse effects that are evident in the current opioid crisis.
Footnotes
Competing interests: None declared.
Contributors: Amit Anand, Donal Roche, Vehniah Tjong and Jihad Abouali contributed to the conception and design of the work. Sarah Wright contributed to the acquisition, analysis, and interpretation of data. Amit Anand and Jihad Abouali drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was supported in part by the Michael Garron Hospital Collaborative Education Research Grant.
- Accepted August 23, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/