

Abstract
Background: The Continuing Professional Development (CPD) (Education) Committee of the Canadian Association of Thoracic Surgeons (CATS) has established a goal of describing the essential knowledge of thoracic surgery. We aimed to develop a national standardized set of undergraduate learning objectives for thoracic surgery.
Methods: We obtained these learning objectives from 4 medical schools in Canada. These 4 institutions were selected to provide a broad geographical representation of medical schools of varying sizes and of both official languages. The resulting list of learning objectives underwent critical review by the CPD (Education) Committee, made up of 5 Canadian community and academic thoracic surgeons, 1 thoracic surgery fellow and 2 general surgery residents. A national survey was developed and circulated to all CATS members (n = 209). Respondents were asked to indicate on a 5-point Likert scale whether each objective should be a priority for all medical students.
Results: Among 209 CATS members, 56 responded (response rate 27%). The mean length of experience in clinical practice among survey respondents was 10.6 (standard deviation 10.0) years. Respondents most commonly reported teaching or supervising medical students monthly (37.0%), followed by daily (29.6%). Eight of the 10 proposed objectives received a mean Likert score of 4/5 or higher and were selected for inclusion in the final list. A finalized list of 8 learning objectives was created, following a final review from the CATS Executive Committee.
Conclusion: We developed a standardized set of learning objectives for medical students that was reflective of the core concepts within thoracic surgery.
Medical students often have limited exposure to subspecialty surgery (including thoracic surgery) over the course of their education. At best, select students may have the opportunity to rotate through this service for a brief period of 2–4 weeks. Most students will enter nonsurgical residencies, most commonly family medicine and will have limited exposure, if any, to surgical training after graduation from medical school.1,2 However, there are certain skills and knowledge that are important for all future physicians, which may be best taught by subspecialty surgeons. A need exists to optimize the learning opportunities for students in subspecialty surgery by identifying a small number of key learning objectives in each area allowing students to learn what is important and to not focus their limited time and resources on other, potentially less important objectives. The Canadian Undergraduate Surgical Education Committee (CUSEC) is working with surgical specialty societies to create a set of nationwide, standardized learning objectives for medical students.3 Objectives and learning modules have been developed for specialties, such as urology and otolaryngology.4,5
A review of the learning objectives for thoracic surgery established by medical schools across Canada identified a high degree of heterogeneity. The Continuing Professional Development (Education) Committee (CPD [Education] Committee) of the Canadian Association of Thoracic Surgeons (CATS), in collaboration with CUSEC, has established a goal of describing the essential knowledge of thoracic surgery for family physicians and other nonsurgeons. We aimed to develop a national standardized set of undergraduate learning objectives for thoracic surgery.
Methods
Learning objectives for thoracic surgery were obtained from 4 medical schools in Canada: University of Alberta, University of British Columbia, University of Toronto and Université de Sherbrooke. These 4 institutions were selected to provide a broad geographical representation of medical schools of varying sizes and of both official languages, and these objectives were compiled and organized by topic. The learning objectives of the Medical Council of Canada (MCC) Qualifying Examination were reviewed to ensure all important topics for thoracic surgery were included in the master list. The resulting list of learning objectives then underwent critical review by the CPD (Education) Committee, made up of 5 Canadian community and academic thoracic surgeons, 1 thoracic surgery fellow and 2 general surgery residents. Redundant learning objectives were consolidated based on consensus, and standardized language was developed to describe each learning objective. Objectives primarily based on observation (e.g., observe esophageal procedure) without actionable and demonstrable concepts for the learner were excluded.
A national survey was then developed by the CPD (Education) Committee and circulated by the CATS. The survey was sent to all CATS members (n = 209). Respondents were asked on a 5-point Likert scale whether each objective should be a priority for all medical students (strongly disagree = 1, strongly agree = 5). Space was provided for comments regarding each objective, and respondents were asked to identify any key learning objectives that were not included (Appendix 1, Table 1, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.004222/tab-related-content). Data were also collected on the number of years in practice, the amount of time spent teaching medical students and the most common clinical setting during such teaching. The coefficient of variation (standard deviation [SD] divided by the mean) was calculated across the Likert score values of the survey responders for each learning objective. A threshold of mean approval of 4/5 on the Likert scale was used to select or exclude objectives from the final list. The survey was open for 4 months, with monthly reminders sent to all CATS members.
The results of the survey were reviewed by the CPD (Education) Committee, and consensus-based changes were made based on respondent feedback. The revised learning objectives were then reviewed by the CATS Executive Committee for final approval.
Results
The full list of learning objectives collected from the 4 medical schools and the MCC are shown in Appendix 1, Table 1, with a unifying learning objective drafted for each topic.
The objectives were refined by the CPD (Education) Committee and classified into 1 skill-based and 9 knowledge-based learning objectives. There was unanimous consensus among the CPD (Education) Committee regarding the exclusion of chylothorax as a learning objective. As this condition is uncommonly encountered outside of thoracic surgery and has nuances of management beyond the scope of primary practitioner.
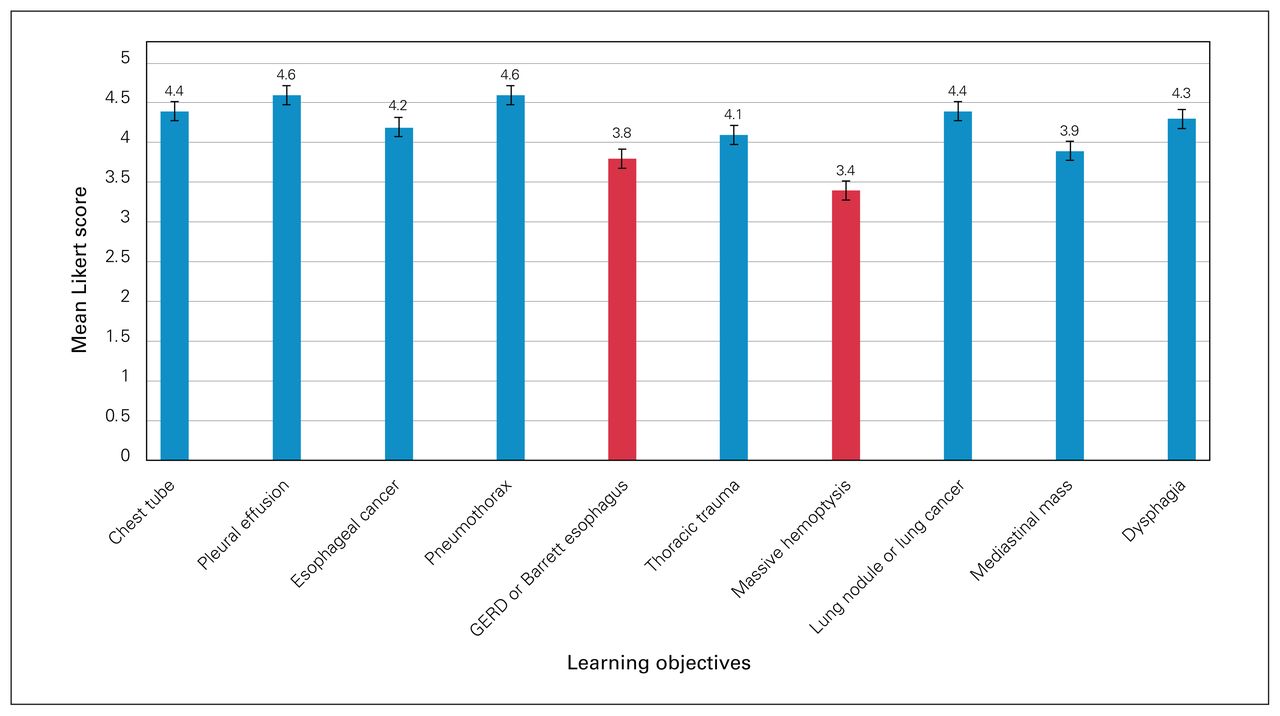
Among the 209 CATS members, 56 responded (response rate 27%). The mean length of experience in clinical practice among survey respondents was 10.6 (SD 10.0) years. All Canadian provinces except for Newfoundland and Labrador and Prince Edward Island were represented in the survey. The most common practice location of survey respondents was Ontario (38.9%). A minority of respondents were from the United States (7.4%). Respondents most commonly reported teaching or supervising medical students monthly (37.0%), followed by daily (29.6%). The most reported setting for teaching was the operating room (91.8%), followed by the outpatient clinic (71.4%), the inpatient ward (71.4%), small group teaching sessions (57.1%) and lecture or didactic teaching sessions (55.1%). Exploratory data analysis showed homogeneity of the data, with the coefficient of variation of the Likert scores across the 10 learning objectives calculated to be 16.8%. Eight of the 10 proposed objectives received a mean Likert score of 4 or higher and were selected for inclusion in the final list (Figure 1).

{kind=link}
The mean Likert score for the proposed thoracic surgery learning objectives from a survey of Canadian Association of Thoracic Surgeons members. GERD = gastroesophageal reflux disease.
Exclusion of thoracic trauma and massive hemoptysis
The learning objectives relating to thoracic trauma (mean Likert score of 3.8) and massive hemoptysis (mean Likert score of 3.4) did not meet the threshold for inclusion. Survey respondents considered thoracic trauma to have substantial overlap with trauma surgery and general surgery learning objectives, and massive hemoptysis was considered an advanced learning topic more appropriate for a surgical resident or fellow. Based on this information, there was consensus from the CPD (Education) Committee to exclude these learning objectives.
Revision of esophageal cancer learning objective
Several survey respondents suggested that the term basic management should be added to the esophageal cancer learning objective, which the CPD (Education) Committee approved by consensus. Esophageal cancer is an increasingly complex disease, and the goal of this learning objective was to highlight the overarching management categories of this condition.
Combination of lung cancer and lung nodule learning objectives
Multiple comments were received regarding the overlapping content between the approach to a lung nodule and lung cancer. This prompted the combination of these 2 learning objectives.
Exclusion of esophageal perforations
Multiple comments were received regarding the consideration of esophageal perforations as an additional learning objective. However, the CPD (Education) Committee decided against inclusion of this objective given the rarity of this condition, the complexity of the management and the likelihood that even in an acute presentation in a low-resource setting, the initial management would be guided remotely by a consulting thoracic surgeon.
Finalized learning objectives
With the above revisions, a finalized list of 8 learning objectives (7 knowledge-based and 1 skill-based [Table 1]) was created.
Final list of undergraduate learning objectives in thoracic surgery
Discussion
Initially developed by Sir William Osler in the 20th century, undergraduate medical education evolved from an apprenticeship model to a formalized medical clerkship.6 Clerkship, as a model for clinical education, suffered from a lack of standardization of the medical curriculum, prompting the Association of American Medical Colleges to call for learning objectives across disciplines.7 This led to the development and endorsement of discipline-specific learning objectives by national organizations.8,9 As the body of medical literature continues to expand, our understanding of the pathophysiology and management of disease processes changes. Thus, it is imperative to review learning objectives over time in a systematic fashion. After a review of institution-specific learning objectives in thoracic surgery, we used an expert-based approach to refine these objectives into a national standard.
The primary goal of these learning objectives was to identify the essential curriculum necessary for medical students with limited exposure to thoracic surgery. Many of these students will go on to pursue medical careers outside of thoracic surgery, and thus, it is important that the relevance of these objectives to various disciplines is emphasized. For example, the value of learning the proper indications and technique for chest tube insertion cannot be understated, as this is a potentially life-saving procedure and may need to be conducted in an emergency setting. We recognize the dynamic nature of clerkship does not always allow for formalized or didactic teaching sessions. Thoracic surgery, like most surgical specialties, can be divided into broad categories: the operating room, the clinic, ward management and emergency consultations. Certain learning objectives may lend themselves better to specific environments. Establishing a schedule with medical learners on service may facilitate the appropriate use of learning opportunities for these objectives.
Thoracic surgery is a diverse discipline with a broad scope of practice. We recognize that the proposed list of learning objectives does not encapsulate the entirety of conditions managed by thoracic surgeons. However, the proposed learning objectives appear consistent with the composition of thoracic surgeon caseloads, with lung cancer forming a large portion of most clinical practices.10 Excluded learning objectives were rejected only after extensive debate. Thoracic trauma as a learning objective has considerable overlap with trauma and general surgery learning objectives. Esophageal perforations, although unique to thoracic surgery, are exceedingly uncommon, and thus, this was not considered high-yield content for incorporation as a learning objective.11 Furthermore, the management of this condition is nuanced, making the establishment of a standardized learning objective challenging. Similarly, massive hemoptysis represents a complex clinical problem, and was considered to be beyond the scope of a general practitioner and to have some overlap with pulmonary medicine.12
The concern of subjectivity in the interpretation of the revised learning objectives was raised by the the CPD (Education) Committee. This was particularly relevant regarding the term basic management. This term is used for the lung cancer, lung nodule and esophageal cancer learning objectives, as well as the chest tube learning objective. Basic management for lung and esophageal cancer refers to the understanding of the overarching management of malignant disease, particularly the steps required to stage these patients appropriately and the subsequent distinction between surgical and medical management of these patients. Basic management does not refer to memorizing the specific stages of resectable compared with unresectable disease, or the specific type of surgical or medical therapies offered. Basic management for the chest tube learning objective refers to the understanding of pleural space physiology and how this relates to chest tube mechanics.
Limitations
This study is limited by the low survey response rate. The CATS members who did respond reported a high rate of interaction with medical students, suggesting that those who did not regularly work with medical students may have been less likely to respond. The responses that were collected may more accurately reflect the subset of CATS members with interest and expertise in undergraduate medical education. Feedback from the survey was only one of multiple measures employed in the development and validation of the learning objectives, with large contributions from the extensive review by the CPD (Education) Committee and the CATS Executive Committee, comprising thoracic surgeons with extensive academic experience. An additional limitation is the lack of input from family physicians. This may represent a selection bias, potentially over-emphasizing the importance of such learning objectives. It is also important to recognize that the content of some of the proposed learning objectives is not exclusive to thoracic surgery, sharing substantial overlap with other specialties. The implementation of such learning objectives should highlight the unique surgical perspective on these objectives, and recognize the scope and importance of other specialties. We have proposed a standardized set of learning objectives, but a lot of work remains on determining the optimal methods to teach, and subsequently assess these objectives.
Conclusion
We developed a standardized set of learning objectives for medical students using a systematic approach. The proposed learning objectives are based on feedback from thoracic surgeons across the country and have undergone an extensive review process by a committee of community and academic thoracic surgeons. These proposed learning objectives are intended to reflect the core concepts within the discipline of thoracic surgery, taking into consideration the constraints of time, educational level and diverse career paths of medical students.
Footnotes
Competing interests: Julius Poon received travel support from Intuitive Surgical and participated on an AstraZeneca Advisory Board. Nazgol Seyednejad received honoraria from Bristol Myers Squibb for a lecture given on neoadjuvant treatment in stage IIIA lung cancer. Simon Turner received institutional funding from Ethicon and advisory board consulting fees from AstraZeneca. No other competing interests were declared.
Contributors: All authors designed the study. U. Jogiat and S. Turner acquired and analyzed the data. U. Jogiat and S. Turner wrote the article, which all authors reviewed. All authors approved the final version for publication.
- Accepted January 23, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/