Article Text

Abstract
Reflection has become established as a key principle underpinning maintenance of standards within professional education and practice. A requirement to evidence reflection within performance review is intended to develop a transformative approach to practice, identify developmental goals, and ultimately, improve healthcare. However, some applications have taken an excessively instrumental approach to the evidencing of reflection, and while they have provided useful templates or framing devices for recording individualistic reflective practice, they potentially have distorted the original intentions. This article revisits the educational theory underpinning the importance of reflection for enhancing performance and considers how to enhance its value within current paediatric practice.
- Medical Education
- Reflection
- professional Development
Statistics from Altmetric.com
Introduction
Reflection is considered one of the key principles and values underpinning maintenance of Good Medical Practice.1 Reflection is defined as ‘a metacognitive (thinking about thinking) process that creates greater understanding of both the self and the situation so that future actions can be informed by this understanding’.2 The General Medical Council (GMC) revalidation procedures require all UK paediatricians to have used reflection as part of their evidence of professional development and all trainees are also expected to use reflection in the completion of their portfolio.3 ,4 Despite this emphasis on reflection within medical education and professional development, there is little discussion around the principles and policies that underpin these approaches in clinical practice as to what is reflection, how to effectively use reflection for professional development or even the evidence for its impact. The appearance of complying with requirements to ‘reflect’ becomes more important than the intended educational purpose. Reflection in professional practice is a way of thinking about productive work, not a strategy or technique.5
The importance of reflection for professional development
Reflection is an essential aspect of all of our lives. We have an experience, we think about why we reacted in a certain way and we then consider whether we need to take action and alter our response to similar experiences in the future. The human species has continued to survive across the millennia by effectively using this process. The obvious inference is that reflection could not only improve professional development but also ensure that there is an impact on patient care through improved judgement.6
The importance of this apparently innate process of reflection for the development of professional expertise has been the focus of many educational theorists (box 1). Donald Schon described how repeated exposure to a wide range of different experiences becomes progressively internalised so that intuitive responses can be quickly made when faced with the complex problems that are typical of professional practice.7 Schon proposed that reflection-on-action informed reflection-in-action. In other words, a deliberate process of thinking about a typical complex experience after the event has the potential to improve intuitive professional decision making.
Reflection and transformative learning; key points from educational theory
-
Reflecting critically on source, nature and consequences of situation.7
-
Identify underpinning ‘assumptions’ and evidence for proposed response.8 ,9
-
Communicative learning; challenge beliefs through discourse and dialogue (with self and/or colleagues through probing literature or discussion).9 ,11
-
Take action following transformed perspectives; make a decision and live with what has been decided until new evidence appears.9 ,11
-
Develop a critically reflective disposition; challenge assumptions, seek validity of evidence or actions, review situations, be open to discourse, look for wider implications of learning experience.9 ,10 ,12
John Dewey, a widely acknowledged educationalist, considered that reflection was a meaning-making process that could move superficial learning to deeper learning.8 He emphasised the importance of reflection as a ‘conscious, active and deliberate’ thinking process that requires the relationships between present and previous experiences to be linked together. An essential aspect is that recurrent patterns of thinking can be identified, challenged and, if required, also modified. Thinking is influenced by a variety of personal beliefs and values that need to be made explicit so that they can be challenged. The stimulus for this thinking and reflection is particularly pertinent when there is uncertainty on the ‘best’ course of action; for example, the clinician may be faced with an acutely wheezy child and feels uncertain about whether he/she should prescribe an antibiotic or not.
The work of Dewey has been expanded with the notion of ‘critical’ reflection for professional development. Jack Mezirow, another educationalist, highlights the need to challenge the way that ‘taken for granted’ assumptions can constrain the way that we perceive and understand our lives.9 It is only by reflection and questioning these assumptions that ‘transformative’ learning can occur, with a change in perspective that produces a change in practice. Following on from the clinical presentation above, the clinician may reflect on his/her uncertainty associated with prescribing an antibiotic and begin to realise that he/she is potentially being influenced by a previous experience rather than following the ‘evidence-based’ guideline. Chris Argyris, from the world of management science, and Donald Schon graphically summarised critical reflection as ‘single-loop’ and ‘double-loop’ learning, drawing on the analogy of a central heating thermostat.10 Single-loop learning merely considers whether we are doing things right, such as making slight adjustments to the heat source to maintain a constant temperature, whereas double-loop learning has a focus on the much more important deeper reflection on whether the right things are being done, such as why a particular room temperature has been chosen. In our wheezy child example, double-loop learning and reflection would promote considering how the guidelines have been developed and the influence of bias in conducting (or interpreting) the studies that informed these guidelines.
Effective reflection has the potential to change practice through transforming research or evidence into action and address the knowledge gap between ‘knowing’ and ‘doing’. This has been alternatively articulated as a ‘Model of Generative Change’ striving to generate insight to facilitate change.11 Four stages of ‘Generativity’ are described: reflection, introspection, critique and personal voice. Ball articulates that a conceptualisation of these stages allows individuals to engage with constructive reflection at different levels of development, based on one's individuality, commitment, own level of advocacy and level of current knowledge. This model intends that personal development is measured against progress, and use of these four phases ensures potential for change by increased performance, underpinned by a need to reflectively challenge assumptions to promote awareness, both at the cognitive and personal levels (table 1).
The process of development within the conceptual ‘Zone of Generativity’
We consider that reflection is at the heart of professional practice and also professional development. However, to achieve the potential of reflection for change in practice, it is essential that reflection has a prompt—a ‘disorientating dilemma’ or a time of uncertainty in what should be done—that leads to exploration with a critical perspective, challenging underlying assumptions, beliefs, motives and values.9 ,12 Practice is necessarily contextualised and does not exist outside of a particular setting, within a cohort of professionals, a community of activity or a set of social and professional engagements. This raises questions about expectations and potential impact of solitary and individual reflection.
Current approaches to reflection for professional development: ‘rituals?”
There is currently great emphasis on ensuring that doctors can demonstrate that they are engaging in the process of reflection on professional practice. Doctors are expected to write about how they have identified a prompt for reflection, a so-called ‘learning need’, from their usual encounters with a wide variety of patients and healthcare professionals. The type of identified learning need is not clearly specified, but could range from a simple lack of knowledge of a drug dose to making complex decisions about end-of-life care. This learning need is then subject to written reflection, with an expectation that the doctors will reveal their thoughts and values, as well as making suggestions as to how their personal initial learning need has been met. The purpose and approach to reflection may not be clearly stated, merely that it is expected of a ‘good doctor’ and there is an intention that it will improve patient care. A permanent record of the process of reflection is required as evidence that reflection has occurred. This record is then shown to an appraiser or trainer. These activities may or may not be effective in promoting reflection, but they have the potential to turn reflection into a procedure contrary to the necessary individualistic approach and intended transformative notion of reflection.5 ,13
Our anecdotal experience is that many doctors consider the above process as ritualistic and not having a tangible benefit on either professional development or improving patient care. A study of medical students’ attitude also indicates similar lacklustre perceptions of the value of reflection for changing practice.14 A simplistic view of reflection, such as the lack of knowledge about a drug dose, is hardly challenging and leading to transformative learning and professional development. The more challenging prompt of, for example, caring for a dying patient reflects the complexity of professional practice, especially when underlying assumptions, values and motives are considered. However, identifying a prompt for reflection in such circumstances requires insight and awareness. The process of reflection also requires thinking and developing meaning from the experience. As highlighted in the previous section, this is a highly personal process and disentangling the complexity of the various factors is challenging to both the personal and professional identities of the doctor. The doctor may be upset, and this can lead to self-protective approaches, including hindsight bias, with inaccurate remembering of thoughts and feelings, but also to selective attention to aspects that may not be perceived as being relevant, especially if these aspects are highly personal. Finally, there is an expectation that this emotive reflection is made public through written or verbal articulation. This presentation will be influenced by how the individual wishes to portray himself/herself to others, both as a person and as a professional. Figure 1 illustrates how this might work in professional practice.

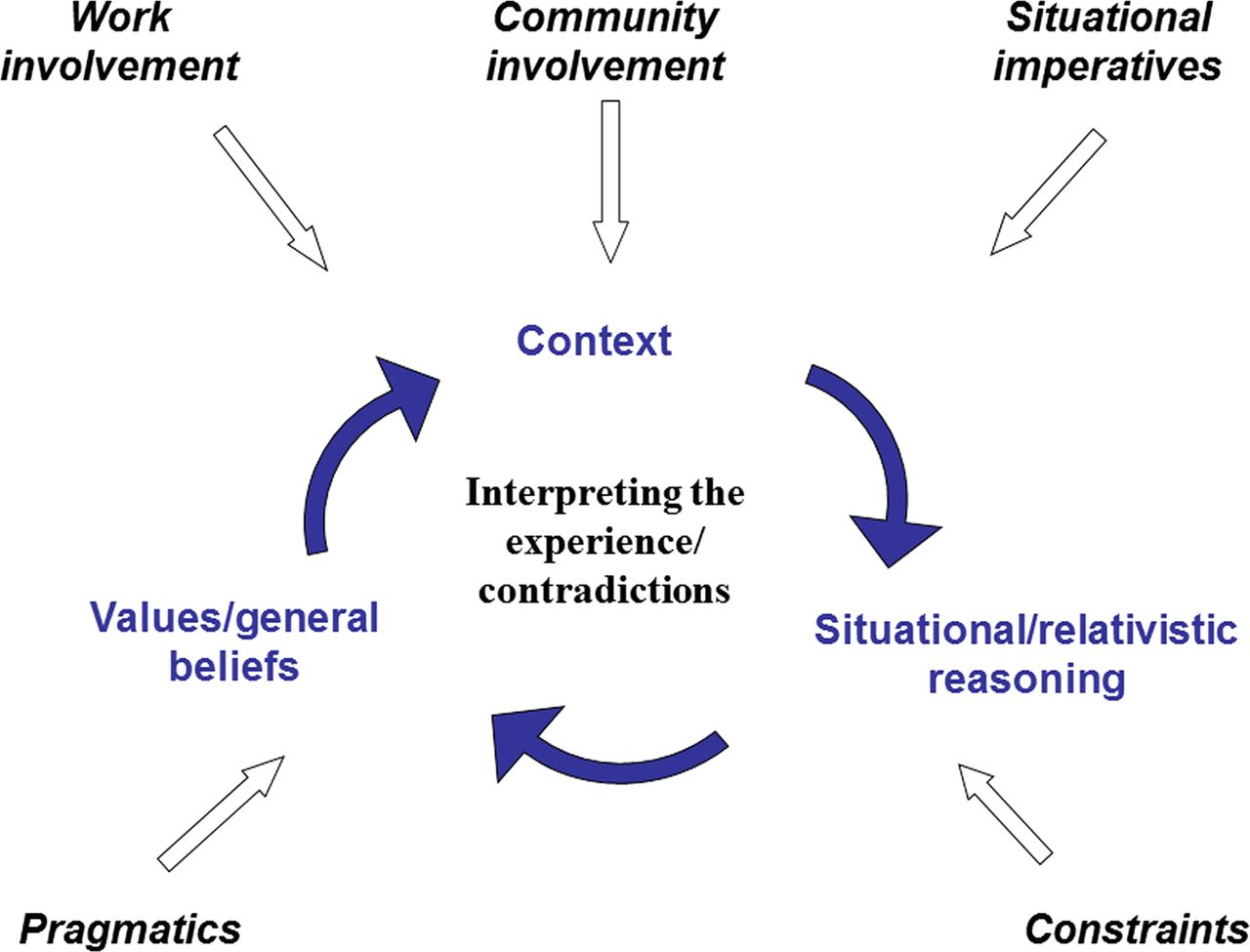{kind=link}
Dialectic reasoning: the practice of arriving at a conclusion by the exchange of logical arguments. The prompt of this model for effective reflection can be illustrated by the following example: consider your (or the clinical team's) deliberative discussions and thinking, and how you might articulate this after a difficult and emotionally challenging encounter, for example, participating in a clinical review on paediatric intensive care at which potential withdrawal of life support was discussed. The context, including the challenging nature of the decision-making processes with other professionals and their previous experiences in similar situations, will have influenced not only how they have considered and viewed the clinical situation, and how this may differ from yours. Constraints could have included aspects of the clinical decision making, including whether all management strategies have been explored and differing perceptions on further realistic and feasible therapeutic manoeuvres. Many other influences may impinge directly or indirectly upon the decision-making processes, including areas that may not have been articulated, for example, situational imperatives including bed pressures, expressed parental views or cultural assumptions, or even one of the players’ previous experience in a similar clinical situation.
A recent systematic review of reflection in health profession education highlighted the lack of convincing evidence that reflection enhanced competence through a change in clinical practice or improved patient care.15 However, there was evidence that reflection was associated with a deeper approach to learning that allowed new learning to be integrated with existing knowledge and skills. An important identified outcome was that diagnostic reasoning of complex and unusual cases could be improved by reflection. It is uncertain why reflection does not achieve its intended impact on healthcare, but it is tempting to suggest that current practice results in little depth to the reflection, with avoidance of the challenge of the essential critical aspects, such as that which produces double-loop learning. This may relate to a lack of intended action for the reflection and use of measures of reflection that mainly concentrate on self-reported change in practice or levels of reflection.2 ,16 This view is additionally supported by extensive research into the determinants of effective organisational learning to produce organisation change.17
Meaningful professional development from reflection?
We believe that reflection is an essential aspect of professional development and that it has the potential to achieve meaningful professional development that can improve patient care.6 However, we also consider that these intended outcomes will only be achieved if there is careful attention to the process of reflection. The main components must relate to challenging practitioners in a supportive environment, recognising that effective reflection for transformative change, which will ultimately enhance clinical practice, requires personal and/or group motivation for reflection, the development of personal metacognitive ‘thinking about thinking’ skills (including noticing, processing and action planning),13 ,18 the opportunity to have trained facilitation and a wider organisational system that recognises and supports these components.19––21
Motivation for critical reflection requires an appreciation of its importance in professional development and also that different learners will have a variety of preferred approaches. Appreciating the importance of reflection is often a slow and prolonged personal and professional journey. It is not simply related to single events but is an ongoing and cyclical process of inquiry in which a personal and professional life story can evolve through using insights gained from reflection about one experience informing subsequent experiences. Research with undergraduate students has highlighted the dislike of the use of written reflection, but offering alternative approaches, such as the use of digital multimedia storytelling, has improved both the engagement and depth of reflection.22 It seems likely that offering a wider use of different approaches to reflection may increase motivation in professional development. Provision of different stimuli, potentially as a choice of templates or questions to promote thinking, will appeal more to the variety of learner and facilitator preferences and is more likely to promote enhanced engagement with transformative reflective practice. Two examples are given in table 2 and box 223 ,24 and many more are available through professional and educational resource repositories.
An example of a Cumulative Reflective log template23
An example of reflective record for single identified event24
Nature of the learning activity
Date:
Briefly describe the learning activity: for example, learning a relevant article, attending a course, observing practice:
State how many hours this took:
Description of the learning activity
Describe why you chose the learning activity or how this opportunity came about; where, when and how you did the learning activity, the type of learning activity and what you hoped to gain from it?
Outcome of the learning activity – how did the learning relate to your work?
What effect had this learning on the way you work, or intend to work in the future? Do you have any ideas or plans for any follow-up learning?
Reflection is a natural process, but like most processes, needs personal development of skills, including recognition of a prompt that stimulates reflection. This prompt is likely to be at moments of uncertainty, especially when there is an associated feeling, such as frustration or anger (figure 1). Awareness of emotions can be developed internally through mindfulness training and externally through feedback from others on observed behaviours.25 Processing the information for reflection is essential for making meaning from experiences and, as highlighted above, this is likely to be developmental over time, especially for critical reflection. We have often found that making explicit the actions to be taken following thinking about the experience is rarely stated, yet the value of reflection is the generation of new insights to inform practice.
The individualistic nature of the current personal practice reflection may also be criticised in a world of team working and cross-professional collaboration. Reflection should be relocated in the many different contexts of practice.5 Identifying and addressing common concerns needs a different model of reflection. This may develop through critical incident review, for example, mortality and morbidity meetings or team debriefs, but pose significant organisational and cultural challenges from the recording of the process through to the safety of the participants. Key features of this so-called ‘productive reflection’ in professional practice illustrate this shift from individual reflective practice to embedding within a complex workplace26 (table 3). If organisations, and groups working within them, were able to predict with certainty where they were going, then productive reflection would not be needed! Productive reflection approach is intended to consider matters that do not have ready solutions, are not clearly formulated, and as such, cannot be rigidly predicted or controlled, or even managed as a routine procedure. It embodies a number of features of awareness, including contextualisation of practice, transdisciplinary and interdisciplinary working, emotional engagement and coproduction within the challenges of power imbalances.
Key features of ‘Productive Reflection’ in professional healthcare workplaces (generated from Cressey and Boud26)
Dialectic reasoning is a key skill within clinical practice through which individuals and groups attempt to arrive at a conclusion by the exchange of logical arguments. In this way, one challenges practice, and when used for reflection, can effectively identify influences and challenge assumptions (figure 1). The work of Schon,7 Dewey8 and Brookfield12 particularly highlights the importance of a systematic process of reflection that is guided by a trained facilitator or mentor. A facilitator, mentor or, as importantly, a colleague or peer should both support and challenge either the individual learner or the group irrespective of seniority or experience to ensure that not only are blind spots opened for discussion but also that critical reflection occurs that questions underlying assumptions and beliefs. The identification and discussion of emotive aspects of personal and professional lives can easily expose the ‘inner person’, and without appropriate support, this essential aspect of critical reflection may not occur in the first place or be blocked on subsequent occasions. Training and supervision of facilitators and mentors is a high investment in resources, yet without this essential aspect it is unlikely that transformative learning will be developed that can produce the intended change in both professional behaviour and improved patient care.7 ,9 ,12 ,16 ,20 ,21 There is a greater reliance on trained and committed educational supervisors, who potentially can fulfil the role of facilitator of enhanced reflective practice, and this is indicated in the enhanced GMC requirements for training of identified ‘Educational and Clinical Supervisors’.27 A single annual review may be pertinent for some areas of practice; however, the development of insight through guided challenge has implications for frequency of meetings and observation of clinical practice, and for different methodologies for recording of outcomes. This may, in some instances, involve a shift of onus onto the mentor or appraiser to record that meaningful reflection has been undertaken, for example, by recording of a work-based assessment, procedure or even simply the process of reflection without documentation of clinical detail.
The wider organisation within which reflection is expected to occur has a responsibility to ensure that facilitated critical reflection can take place, with appropriate allocation of resources, and that there are opportunities to implement the changes in professional behaviour to allow patient care to be improved. This requires cultural and organisational change to create a safe environment where challenges of existing policies and procedures are seen as an essential aspect of professional practice and will not lead to disciplinary action.
Conclusion
Reflection is part of the art of medical practice and ‘demands the development of specific skills, the brain and the mind, requires attention to high quality feedback and is subject to scientific investigation and understanding’.6 Concepts and frameworks are valuable; however, their role in facilitating reflection is not for simple recall and regurgitation but to help prompt, challenge and make sense of the complexity of experiences. We need to rethink our engagement in reflective practice in situations that are rich and complex, as epitomised by paediatric clinical practice. The principal role of reflection, that is, to enhance perception and ‘acquisition of wisdom’,6 is going to require more than ritualistic completion of reflection requirements, as is becoming common practice within formal performance review procedures. Enhancement of clinical practice and organisational change through reflection is inherently grounded within the requirement to have assumptions challenged; this will come through mentoring, and systems and policies that allow identification of aspects to focus on, rather than a bland generic, individualistic, broad-brush stroke approach.
Footnotes
-
Contributors All authors contributed to the planning, drafting, literature review, revising and final approval of the manuscript.
-
Competing interests John Sandars is medical education advisor to the RCPCH Education and Training Quality Committee.
-
Provenance and peer review Commissioned; externally peer reviewed.